
Abstract
Objectives:
The purpose of this study was to evaluate whether anticoagulation (warfarin or direct oral inhibitors) affected the success of endovenous treatment.
Methods:
Patients taking anticoagulation (warfarin or direct oral inhibitors) undergoing endovenous treatment in the form of endovenous laser ablation (EVLA) were matched against controls for sex, age, leg, and vein. Data were collected prospectively between January 2012 and March 2017. The primary endpoint was failure of treatment at 6-week postoperative duplex scan. The rates of major bleeding, hematoma, endothermal heat-induced thrombosis, venous thromboembolism, or pulmonary embolism were also compared between groups.
Results:
Two hundred eighty-four limbs underwent EVLA during the study period. Of this, 23/284 (8.1%) procedures were done in patients on anticoagulation. 21/23 (91.3%) limbs had venous occlusion at follow-up compared with 23/23 (100%) of controls (P = .49). The patient who failed treatment in the anticoagulation group had undergone small saphenous vein (SSV) ablation. There was no difference in the complication rates between groups.
Discussion:
This study demonstrates that anticoagulation does not affect success rates of EVLA though there was higher recanalization rate in patients undergoing SSV ablation. Anticoagulation can be continued safely in patients undergoing this procedure.
Keywords
Introduction
Endovenous treatment is now the first line for the management of superficial venous incompetence in anatomically suitable cases 1 with Level 1 evidence supporting the efficacy and safety of this modality. 2,3 A proportion of patients with superficial venous disease is on long-term anticoagulation therapy which may affect the long-term success rates of endovenous treatment. To date, there have been a small number of studies, with small total numbers of patients, looking at the effect of anticoagulation on the success rates of endovenous treatment. 4 –8 Anticoagulation was continued perioperatively in these studies with low recanalization rates. There has been one more recent study with a larger series of patients with similar findings. 9
In this study, we looked at whether anticoagulation affected 6-week recurrence rates following endovenous laser ablation (EVLA) in patients on warfarin or direct oral inhibitors compared to a well-matched control group.
Methods
Data were collected retrospectively on all patients who underwent EVLA for symptomatic (clinical, etiological, anatomical, and pathological elements [CEAP] 2-6), superficial venous incompetence of the great saphenous vein (GSV) or small saphenous vein (SSV) between January 2012 and March 2017 from a prospective collected database. Patients who were on anticoagulant therapy in the form of warfarin or direct oral inhibitors (rivaroxaban, apixaban) were matched against controls according to sex, age, leg (Right or Left), and vein (GSV or SSV). Patients were instructed to continue on anticoagulant therapy perioperatively as per their normal regime including taking the anticoagulation the day before the procedure as well as on the day after the procedure.
Pre- and postoperative duplex scans were performed in an accredited vascular laboratory. Postoperative scans were performed 6 weeks after EVLA to look for evidence of recanalization of the treated vein. All cases were performed by a single operator (A.T.) using a standard technique that has been previously described. 10 Briefly, EVLA was performed using a 1470 nm diode system (Vascular Solutions, Minneapolis, Minnesota) under tumescent anesthesia without sedation. Venous access was obtained with 19G needle with transverse ultrasound imaging. A 0.035-in safety-J guidewire was passed along the vein to the saphenofemoral junction or saphenopopliteal junction under transverse ultrasound imaging. A 4F sheath is passed over the wire to the junction. If the guidewire could not be passed through the full length of the vein, the vein was treated in 2 sections (segmental ablation). Ultrasound was used to guide injection of tumescent anesthetic solution (40 mL 1% lidocaine with adrenaline solution, 10 mL 4.2% NaHCO3 solution, 450 mL 0.9% saline) into the saphenous fascial compartment along the entire length of the vein to be treated. Treatment power used in this series was 10 watts continuous power. The sheath and catheter were withdrawn together continuously at 1 cm/8 seconds. The intended energy delivery was 70 to 90 Joules/cm for GSV saphenous vein and 50 and 60 Joules/cm for SSV. Once the saphenous trunk had been treated, ablation and patency of the deep veins were confirmed with ultrasound. Compression with a class 2 stocking was applied on the table. Immediate walking was encouraged. Continuous compression was advised for 7 days. Stockings were worn during the daytime only for a further 7 days. Oral analgesics to be used as needed were prescribed before discharge the same day. Most patients were able to resume normal activities by the next day.
All procedures on patients on anticoagulant therapy were performed under local anesthetic. This was also the case for the matched controls. A Fisher exact test was used to calculate whether there was a statistically significant difference in 6-week recanalization rates between the cases and matched controls.
Results
In total, 284 patients underwent EVLA for symptomatic superficial venous incompetence between January 2012 and March 2017. There were 19 patients (23 limbs) patients on long-term anticoagulant therapy. Ten (43.5%) procedures were performed in male patients and 13 (55.5%) were done in female patients. The mean age was 59.4 years (range: 32-83). The indication of surgery according to CEAP classification was C2: 8.3%, C3: 20.8%, C4: 54.2%, C5: 0%, and C6: 16.7%. There were 18 GSV and 5 SSV EVLA procedures. The mean diameters of treated GSVs and SSVs were 8.52 and 7.40 mm, respectively.
Indications of anticoagulation were atrial fibrillation (40%), DVT (30%), prosthetic heart valve (13%), transient ischemic attack (9%), pulmonary embolism (4%), and polycythemia (4%). Sixteen of the patients taking long-term anticoagulation were taking warfarin while 2 patients were on apixaban and 1 was on rivaroxaban. Patients also continued taking their antiplatelet drugs.
For the 23 limbs, 23 matched controls were selected according to sex, age, leg, and vein. The controls were selected in the absence of them being on anticoagulation, without evidence of deep venous reflux or history of DVT. The mean age of controls was 58.5 years which was not significantly different from the anticoagulant group.
In the study group, 21/23 (91.3%) were occluded on duplex at 6-week follow-up, whereas 23/23 (100%) were occluded in the control group. The difference was not statistically significant (P = .49). Both patients who had recanalization at 6 weeks were on warfarin for prosthetic cardiac valves and had SSV EVLA. One of these patients underwent repeat EVLA with successful occlusion while the other patient has a further failed EVLA despite the use of higher energy setting. The failure rate of patient undergoing SSV ablation was 2/5(40%) compared to no failure in GSV group. This was statistically significant (P = .006).
There were no major procedure-related complications such as major bleeding, hematoma, endothermal heat-induced thrombosis, venous thromboembolism, or pulmonary embolism in both groups. In the control group, 2 patients developed thrombophlebitis which resolved with conservative treatment.
With regard to 4 patients with active ulcers in the study group, all had completely healed except 1 patient who had partially healed but required further compression bandaging subsequently.
Discussion
The results of this study conform to the previous research conducted looking at the effect of anticoagulation on recanalization rates in patients undergoing endovenous treatment for superficial venous incompetence which has been summarized in Table 1. Generally, the complication rates are low in terms of major or minor bleeding in all the series. All the series except that of Sufian et al and ours utilized only warfarin as their anticoagulant though this is likely to change in the future with increasingly more patients being anticoagulated with direct oral inhibitors. This may affect the results as these have potential for increased risk of bleeding complications such as hematoma and a theoretical higher risk of recanalization, but there is not enough evidence to support this at present.
Summary of Published Outcomes of Patient Undergoing Endovenous Ablation While on Anticoagulation.
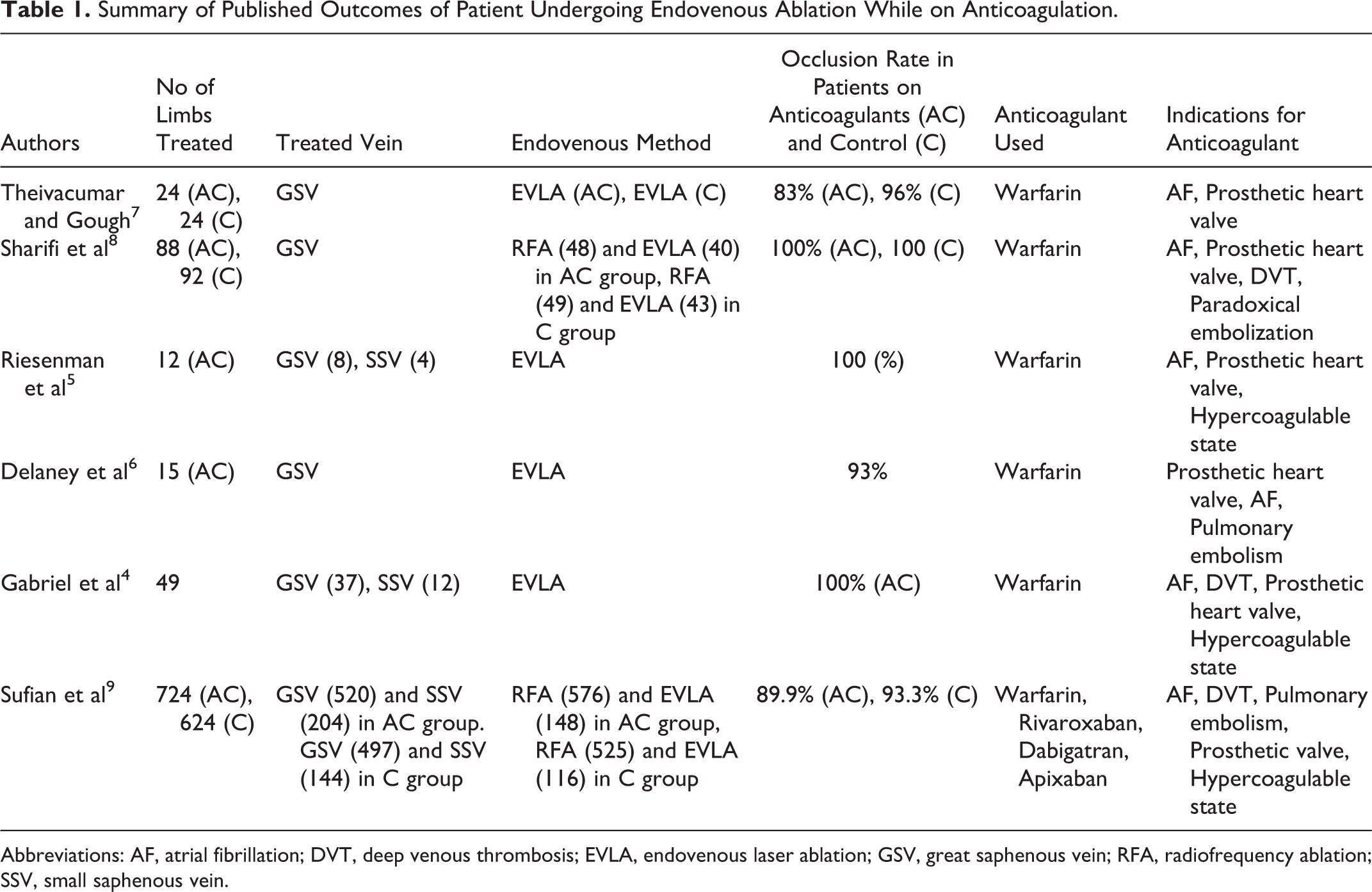
Abbreviations: AF, atrial fibrillation; DVT, deep venous thrombosis; EVLA, endovenous laser ablation; GSV, great saphenous vein; RFA, radiofrequency ablation; SSV, small saphenous vein.
Most of the studies have been small in patient numbers except that of Sufian et al, who recently published a much larger series of patients undergoing endovenous treatment in patients on anticoagulation. 9 Like our study, they looked at patients taking both warfarin and direct oral inhibitors. At 3 days post procedure, the rate of procedural failure was 5.6% in the anticoagulation group and 0.5% in the control group (P < .0001). This however did not persist at 1 month (10.1% in the anticoagulation group and 6.7% in the control group; P = .086). There were no significant differences in rates of DVT or hematoma between groups. However, in our series, all patient attended follow-up while in Sufian et al series only 63% patient attended follow-up at 1 month. Their control groups were also younger, lower number of males, and higher BMI compared to our series where patients were well matched.
Of note, both patients who developed recanalization in our series were on warfarin for prosthetic cardiac valves and were being treated for SSV reflux. One of these patients needed an international normalized ratio (INR) of between 3 and 4. From such small numbers, it is not possible to say with any assurance that a higher INR predicts recanalization (procedural failure); however, this may be an area that could be looked at further with a larger series of patients. The diameters of these veins were 8.2 and 7.9 mm, and both underwent repeated EVLA. This led to resolution in 1 case (7.9 mm); however, in the other case (8.2 mm), the repeated EVLA was unsuccessful.
There are some obvious limitations to this study in that these are small numbers; however, the total numbers are comparable to the previous studies conducted in this area. Preoperative INR levels were not routinely recorded prior to EVLA procedures as the policy is for the patient to continue their normal anticoagulation regime. This may have an impact on the likelihood of recanalization and may be an area to investigate further.
In conclusion, the results of this study demonstrate that continued anticoagulant therapy over the perioperative period in patients undergoing endovenous laser therapy does not affect 6-week postoperative recanalization rates. Continuing anticoagulation does not lead to increased bleeding or systemic complications, and this may also be utilized in patients who are at high risk of DVT to prevent this complication especially as patients undergoing EVLA are prone to this. 11
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.