
Abstract
Background:
Complete revascularization, achieving inline flow to the foot through at least 1 patent tibioperoneal artery, is considered to be desirable for treating critical limb ischemia (CLI). Hybrid procedure, combined femoral endarterectomy and endovascular treatment, is commonly performed on patients with CLI because they often present with complicated lower extremity lesions involving the common femoral artery. This study aimed to investigate the efficacy of complete revascularization (CR) achieved by hybrid procedure on limb salvage in patients with CLI.
Methods:
Between February 2010 and January 2016, 95 limbs (82 patients) were treated by lower extremity hybrid procedure; of these 95 procedures, 61 were for patients with CLI. We defined CR as achieving inline flow to the foot through at least 1 patent tibioperoneal artery. Complete revascularization was performed on 37 limbs, and incomplete revascularization (IR) was performed on 24 limbs. Specific variables, including patient age, male–female ratio, Rutherford classification, preoperative and postoperative ankle–brachial pressure indices (ABIs), follow-up duration (months), primary patency rate, assisted primary patency rate, secondary patency rate, and major amputation rate, were analyzed.
Results:
The mean age was similar between the groups 67.2 years in the CR group and 70.7 years in the IR group (P = .11). Limb ischemia severity was significantly higher in the CR group: 63% of the patients scored Rutherford 5 in the CR group, compared to 30% in the IR group (P = .027). Mean postoperative ABI was significantly higher in the CR group (CR: 0.87, IR: 0.53; P = .0001). Major amputation rate was higher in the IR group (CR: 2.7%, IR: 13%; P = .29), and major amputation-free survival rate at 3 years after the index procedure was higher in the CR group (CR: 97%, IR: 81%; P = .054).
Conclusion:
Complete lower extremity revascularization was beneficial for patients with CLI, avoiding major amputation.
Keywords
Background
Critical limb ischemia (CLI) deteriorates patients’ quality of life because it leads to severe pain, nonhealing wounds, uncontrollable infection, and higher mortality rates. 1,2 Notably, 40% of patients with CLI lose their limbs within 6 months if prompt revascularization treatment is not performed. 1 Advanced peripheral arterial disease (PAD) due to atherosclerosis is the leading cause of CLI, and recent improvements in endovascular techniques and treatment device development have enabled more patients with PAD to be treated in a minimally invasive manner. Endovascular treatment (EVT) has already had a major role in treating lower extremity arterial lesions, particularly lesions in the iliac artery and superficial femoral artery (SFA). However, EVT has inferior results in common femoral artery (CFA) lesions; thus, surgical endarterectomy of atherosclerotic plaques remains the standard treatment. 3
Patients with CLI typically present with multiple complex lesions in their lower extremities. When these lesions involve the CFA, a hybrid procedure, combining femoral endarterectomy and EVT, is a good treatment option. 4 One of the benefits of hybrid procedure is that both inflow and outflow lesions can be treated in a single procedure. Endarterectomy and patch angioplasty of the CFA provide convenient access for EVT of such complex lesions. Patients with PAD often have systemic comorbidities, such as diabetes, coronary artery diseases, cerebrovascular diseases, and renal dysfunction. When multilevel lower extremity revascularization is required for such patients, a hybrid procedure is less invasive than open surgery. Although patients with intermittent claudication of the lower extremities are well treated by inflow-only revascularization, 5 patients with CLI may require more aggressive revascularization, since complete revascularization (CR), achieving a direct blood supply to the foot, is theoretically favorable for limb salvage. However, accomplishing a complete revasclarization in patients with CLI can demand a lengthy, highly invasive procedure if it is attempted only by open surgery; hybrid procedure, on the other hand, may be a promising alternative for such—often morbid—patients. It also remains to be elucidated whether CR is superior to inflow-only revascularization for patients with CLI; therefore, the purpose of this study was to evaluate the efficacy of CR, achieved by hybrid procedure, for limb salvage in patients with CLI.
Patients and Methods
This retrospective study was approved by the institutional review board (Submission ID Number, 2016-0382; Internal Reference Code, e007). Informed consent was obtained from all patients. Before the surgery, each patient was evaluated by lower extremity arteriography, contrast-enhanced computed tomography (CT), contrast-enhanced magnetic resonance imaging (MRI), or their combination. We defined “lower extremity hybrid procedure” as a combination of femoral endarterectomy and subsequent endovascular procedure to treat the CFA and other arterial lesions in the ipsilateral side; of note, procedures such as a combination of femoral endarterectomy, EVT of ipsilateral iliac lesion, and ipsilateral infrainguinal bypass surgery were also included when they were performed simultaneously. We determined the quality of revascularization based on the findings of completion angiogram: When there was at least 1 inline flow to the foot through a patent tibioperoneal artery, we classified the quality “CR”; whereas, when there was no inline flow to the foot, we classified the quality “incomplete revascularization (IR).” After the index procedure, each patient usually continued the same antiplatelet agent as the one prescribed preoperatively. If there was no preoperative antiplatelet agent prescribed, we administered at least 1 antiplatelet agent, preferably clopidogrel bisulfate, postoperatively. The revascularized lesions were surveyed every 3 to 6 months primarily by duplex ultrasonography and ABI measurement. When further investigation was necessary, lower extremity angiography, contrast-enhanced CT, contrast-enhanced MRI, or their combination was performed on each physician’s discretion.
Our target patient cohort was patients with limb-salvageable CLI (ie, Rutherford classification 4 and 5) who underwent lower extremity hybrid procedure for the first time between February 2010 and January 2016. Patients with lower extremity intermittent claudication (ie, Rutherford classification 0 to 3) or those with nonlimb salvageable CLI (ie, Rutherford classification 6) were excluded from our analysis. The criterion of Rutherford class 4 was ischemic rest pain combined with resting ankle pressure <40 mm Hg, flat or barely pulsatile ankle or metatarsal pulse volume recording, or toe pressure <30 mm Hg; the criterion of Rutherford class 5 was minor tissue loss combined with resting ankle pressure <60 mm Hg, ankle or metatarsal pulse volume recording flat or barely pulsatile or toe pressure <40 mm Hg. 6 We divided such patients with CLI into 2 groups, CR group and IR group, according to the quality of revascularization. The primary end point was major amputation-free survival. We investigated the baseline characteristics of patients, including age, sex, history of hypertension, diabetes, hyperlipidemia, previous cerebrovascular disease, previous coronary artery disease, chronic obstructive pulmonary disease, chronic kidney disease of stage ≥ 3, hemodialysis, active smoking rate, and estimated glomerular filtration rate. We also investigated periprocedural factors and postprocedural outcomes including preoperative severity of ischemia (determined by Rutherford classification), target lesion details (Trans-Atlantic Inter-Society Consensus [TASC] classification 1 ), preoperative and postoperative ankle–brachial pressure index (ABI) values, procedure duration, revascularized site other than CFA lesion, groin infection or wound dehiscence rate, length of hospital stay, postoperative patency rate of target lesion, postoperative additional intervention for lesions other than the initial target lesion, follow-up duration, major amputation, and death. We calculated the primary, assisted primary, and secondary patency rates of the revascularized lesions (except femoral endarterectomized site) on the index hybrid procedure.
Statistical analyses were performed with JMP Pro 11.0.0 (SAS Institute Inc, Cary, North Carolina). Numerical data were analyzed by Student t test, categorical data were analyzed by χ2 test, and graft patency rate and major amputation-free rate were analyzed by log-rank test. P < .05 was considered to indicate a statistically significant difference.
Lower Extremity Hybrid Procedure
Our typical hybrid procedure begins with an open femoral endarterectomy. A longitudinal groin skin incision is made above the femoral artery, and the CFA, SFA, and profunda femoris artery (PFA) are exposed and encircled with vessel loops. When the plaque extends into the external iliac artery (EIA), the EIA is secured at the level where the arterial wall is soft enough to place a vascular clamp. Following intravenous administration of heparin, maintaining an activated clotting time >200 seconds, a longitudinal arteriotomy is performed on the anterior wall of the CFA. The arteriotomy is carried out distally until a clear end point of the plaque is detected; proximally, the arteriotomy is intentionally not extended beyond the inferior epigastric artery branch or deep iliac circumflex artery branch even when the plaque extends into the EIA so that subsequent angioplasty of the EIA can be carried out safely. Endarterectomy of the femoral artery is performed as much as possible, and profundaplasty is performed as required. A patch, typically a bovine pericardial patch, is applied to close the arteriotomy. For subsequent endovascular procedures, the patch is punctured, and a guidewire is inserted to secure vascular access. Retrograde puncture is performed to treat aortoiliac lesions, whereas antegrade puncture is performed to treat lesions below the CFA. Primary stenting may be indicated for long-segment occlusions or flow-limiting dissections as determined by the surgeon. For patients of Rutherford class 5, wound debridement of necrotic tissue and/or minor amputations of gangrenous toes were added at the end of procedure, on each surgeon’s discretion.
Results
Between February 2010 and January 2016, 95 limbs (82 patients) were treated using lower extremity hybrid procedures in total. Of these 95 limbs, 33 (35%) limbs were treated for moderate to severe claudication (Rutherford classification 2 or 3), 61 (64%) limbs were treated for limb-salvageable CLI with pain at rest, minor tissue loss, or nonhealing ulcers (Rutherford classification 4 or 5), and 1 (1%) limb was treated for nonlimb-salvageable CLI with major tissue loss (Rutherford classification 6). The 61 limbs treated for limb-salvageable CLI (Rutherford classification 4 or 5) were divided into CR group and IR group. There were 37 limbs (37 patients) in the CR group and 24 limbs (22 patients) in the IR group. Baseline characteristics of patients were similar between the 2 groups (Table 1).
Patient Demographics.
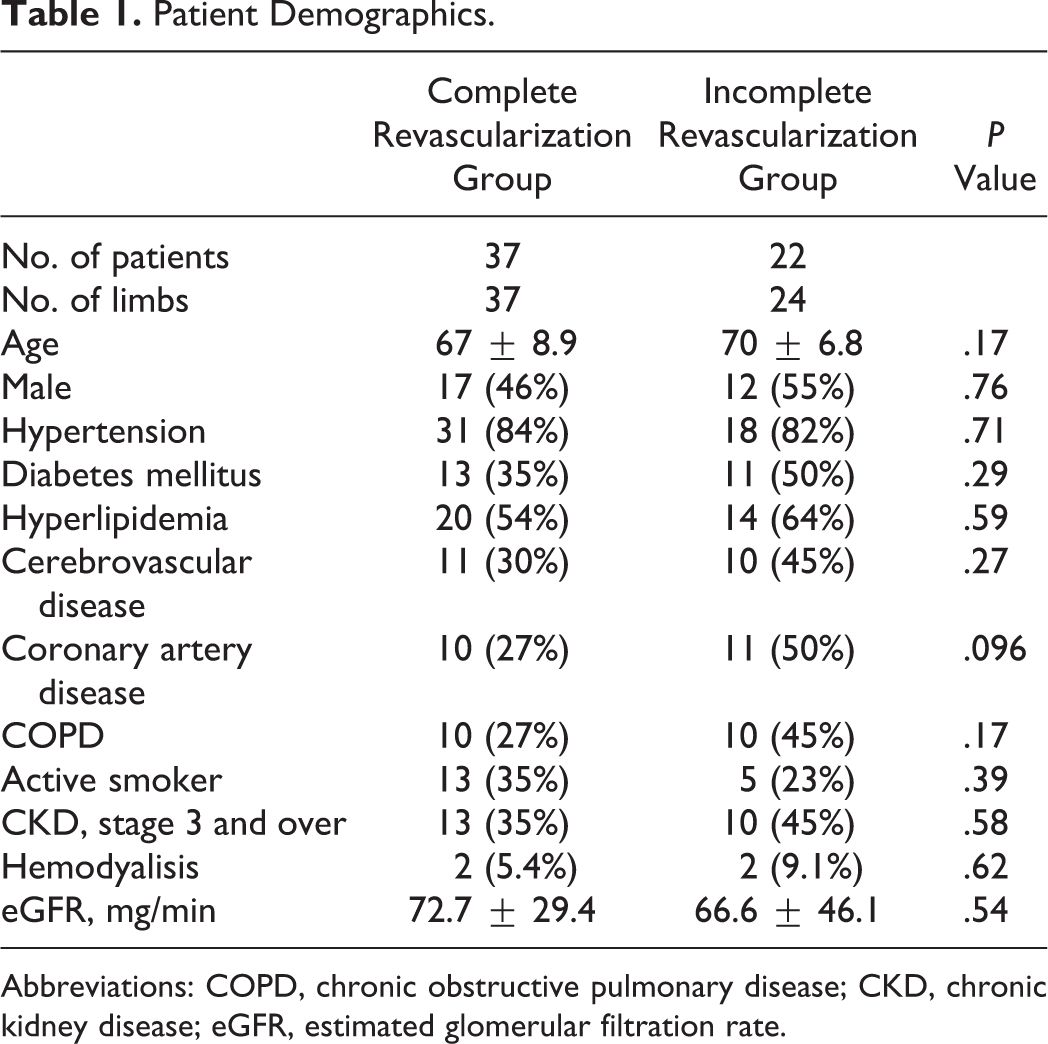
Abbreviations: COPD, chronic obstructive pulmonary disease; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate.
Procedure details and outcomes are shown in Table 2. The proportion of procedures for Rutherford-5 CLI performed in the CR group was significantly greater than that in the IR group (62% vs 33%; P = .037). Preoperative mean ABI values were similar between the CR and IR groups (0.42 vs 0.34; P = .23), whereas postoperative mean ABI value was significantly higher in the CR group (0.87) when compared to the IR group (0.55; P < .001). Mean procedure duration was similar between the CR and the IR groups (294 minutes vs 333 minutes). In terms of sites other than the CFA lesion that were revascularized, there were significantly more iliac-only revascularization procedures performed in the IR group (75%) than in the CR group (32%; P = .0016), whereas there were significantly more iliac and infrainguinal revascularization procedures carried out in the CR group (41%) when compared to the IR group (13%, P = .023). Five (14%) of 37 in the CR group and 3 (13%) of 24 in the IR group required both antegrade and retrograde EVTs at the time of the index procedure. Mean length of hospital stay was similar between the CR and the IR groups. Additional, metachronous interventions for lesions other than the initial target lesions were more frequently performed in the IR group postoperatively (25%) when compared to the CR group (2.7%). Mean follow-up duration was similar between the CR and IR groups (18 months vs 13 months). More major amputations were performed in the IR group (13%) when compared to the CR group (2.7%). The breakdown of 4 major amputations was as follows: 1 patient of Rutherford class 5 in the CR group, 1 patient of Rutherford class 4, and 2 patients of Rutherford class 5 in the IR group. There was no difference in mortality between the 2 groups (14% in the CR group and 17% in the IR group).
Procedure Details and Outcomes.
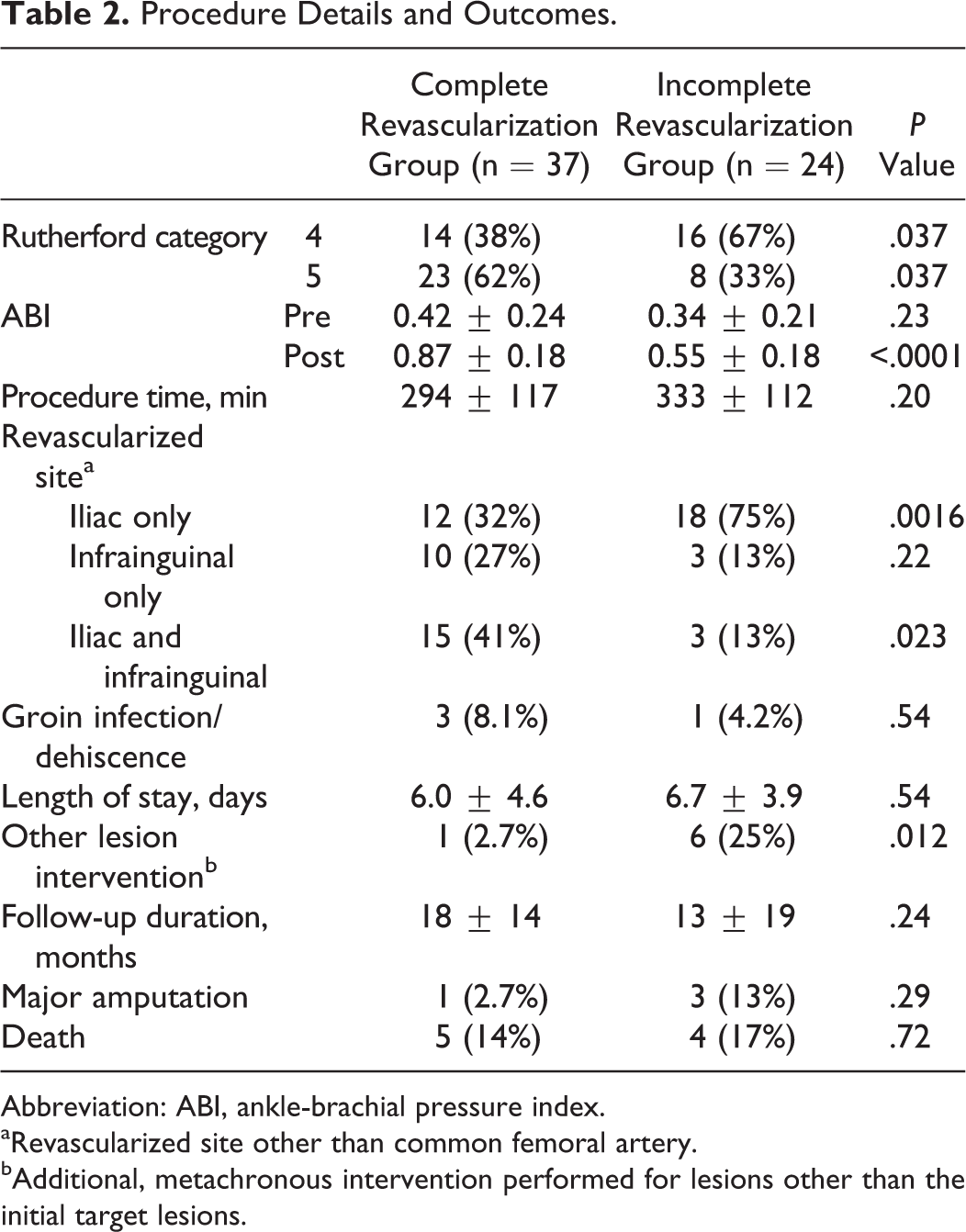
Abbreviation: ABI, ankle-brachial pressure index.
aRevascularized site other than common femoral artery.
bAdditional, metachronous intervention performed for lesions other than the initial target lesions.
Table 3 presents details of the target lesions in each group. There were more iliac artery lesions in the CR group than in the IR group. The severity of iliac lesions was similar between the groups: The majority were TASC-C lesions, followed by TASC-D lesions. Femoropopliteal lesions were significantly more common in the IR group: 27 (73%) in the CR group versus 24 (100%) in the IR group (P = .004). The severity of femoropopliteal lesions was similar between the groups: The majority were TASC-D lesions, followed by TASC-B lesions. Eight of total 23 TASC-D lesions were revascularized by bypass surgery instead of EVT. In terms of the run-off arteries at the end of index procedure, all patients in the CR group had at least 1 patent tibioperoneal artery, while 21% in the IR group had no patent tibioperoneal artery (P = .007). There were a total of 5 tibioperoneal EVTs (4 in the CR group and 1 in the IR group) at the time of index procedure. Three of them were patent without any additional intervention, one needed open thrombectomy for acute thrombosis, and one ended in major amputation.
Details of Target Lesion.
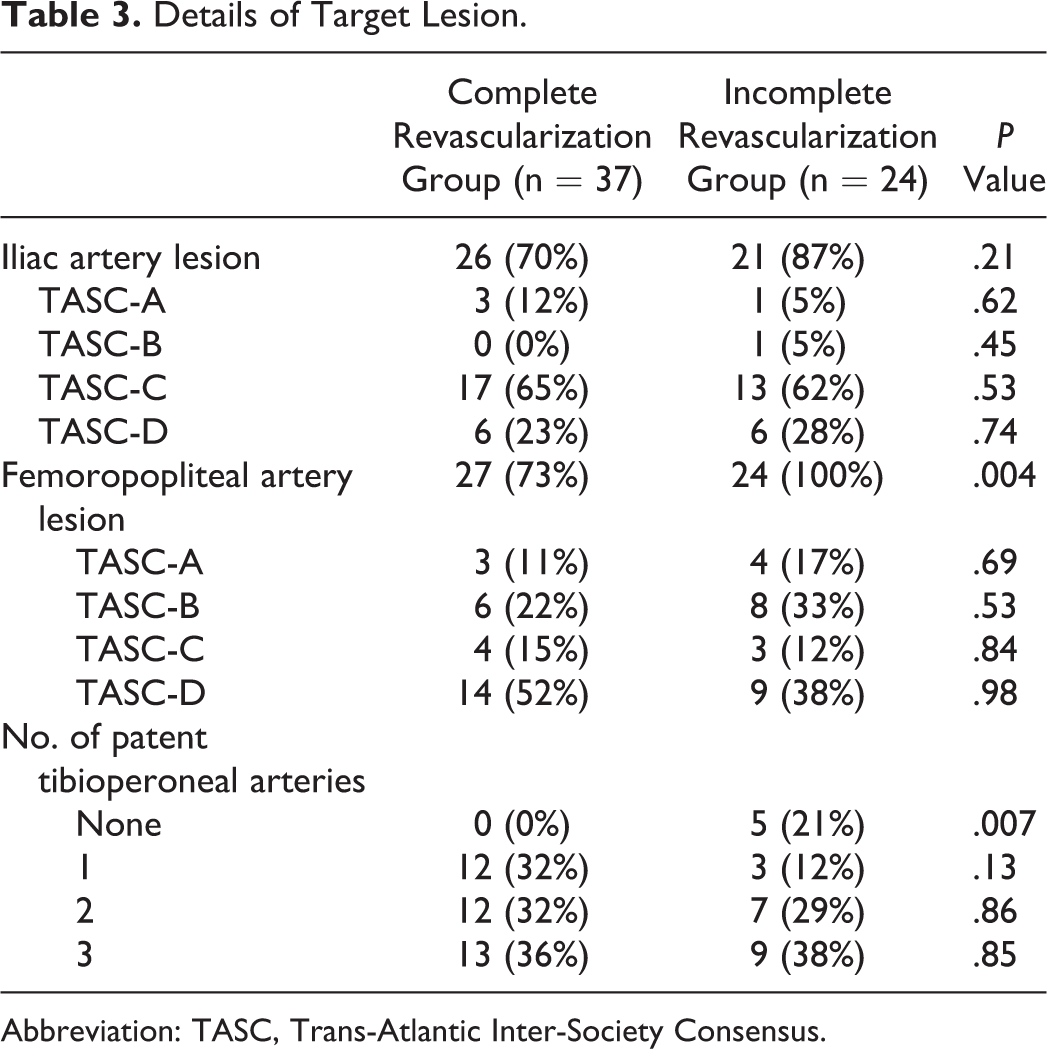
Abbreviation: TASC, Trans-Atlantic Inter-Society Consensus.
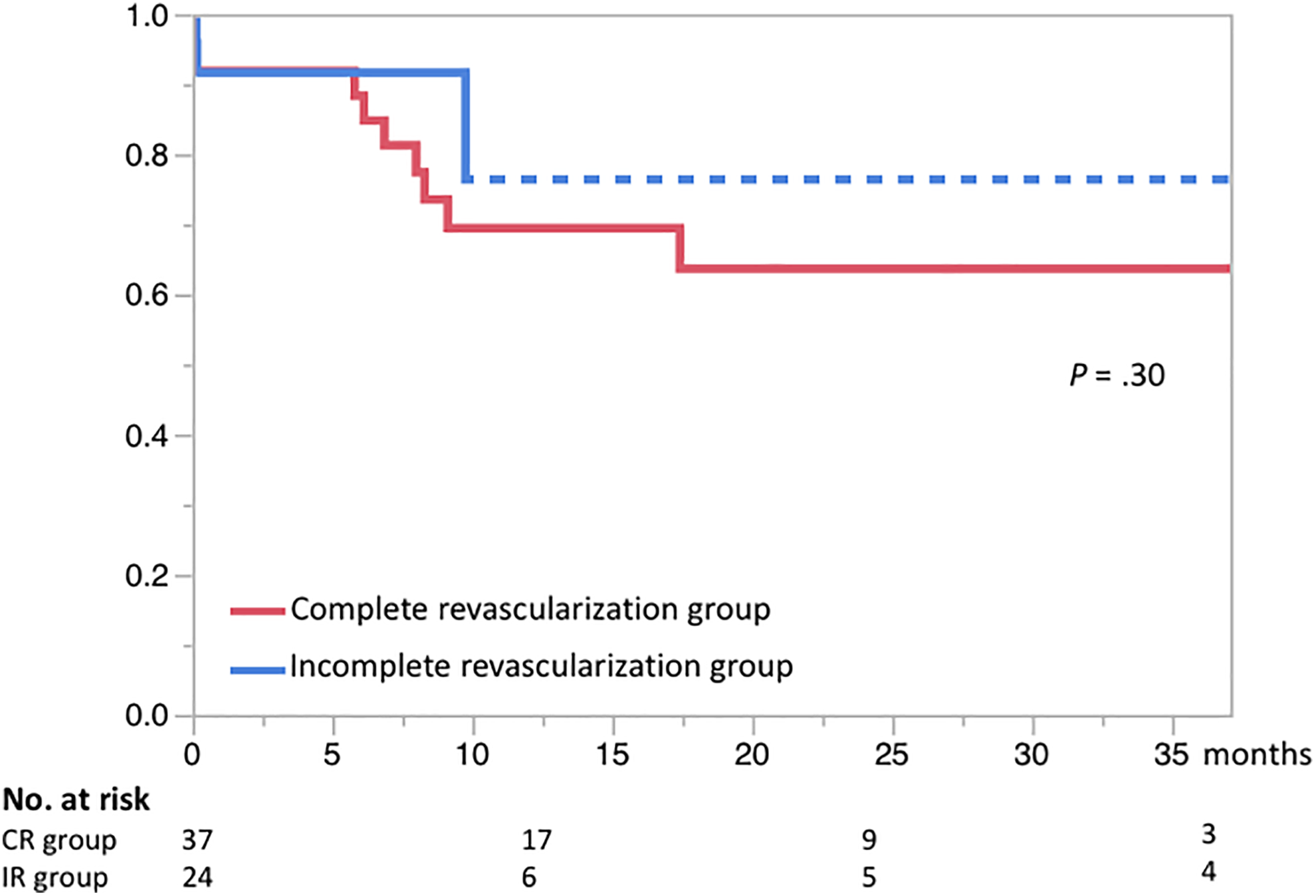
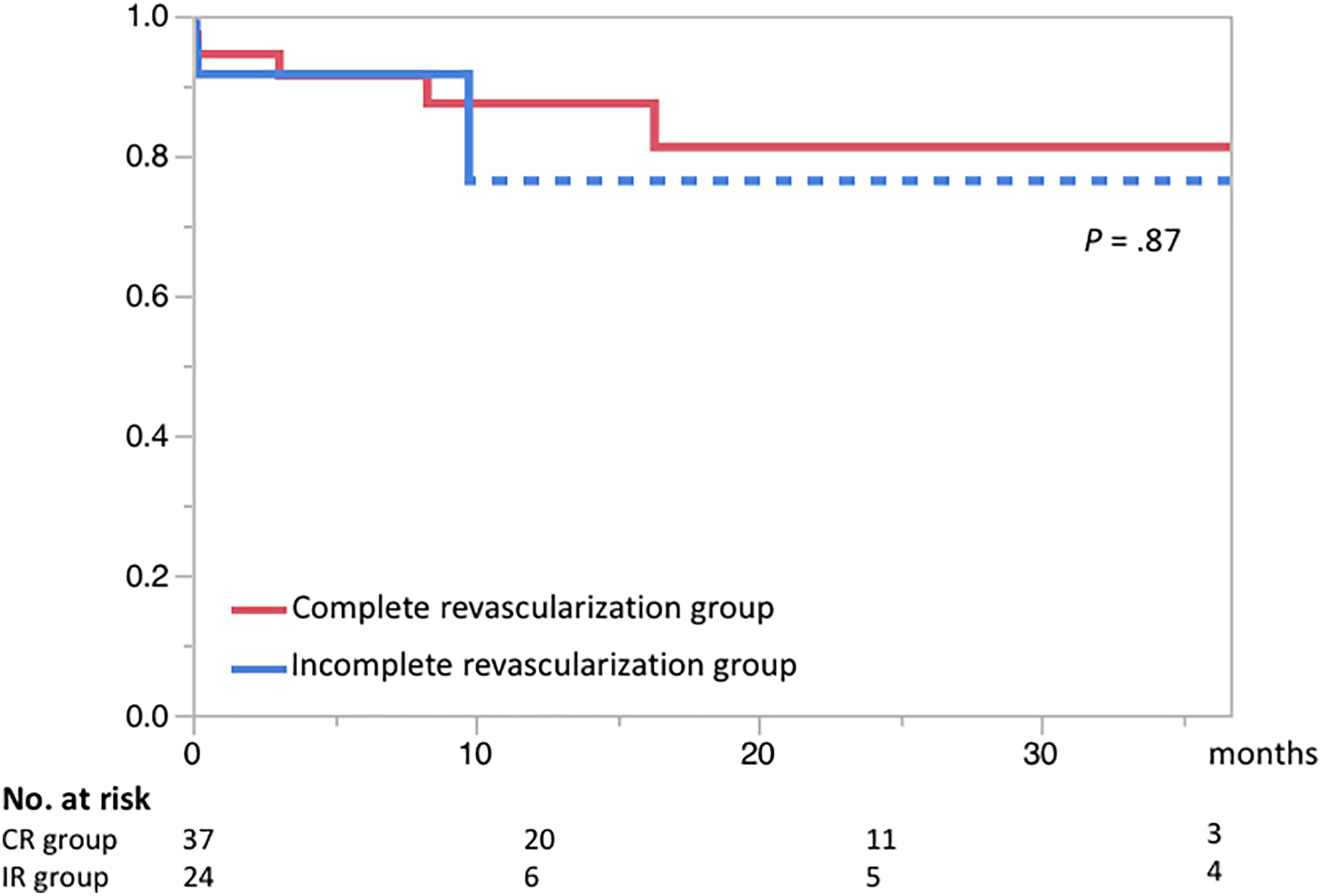
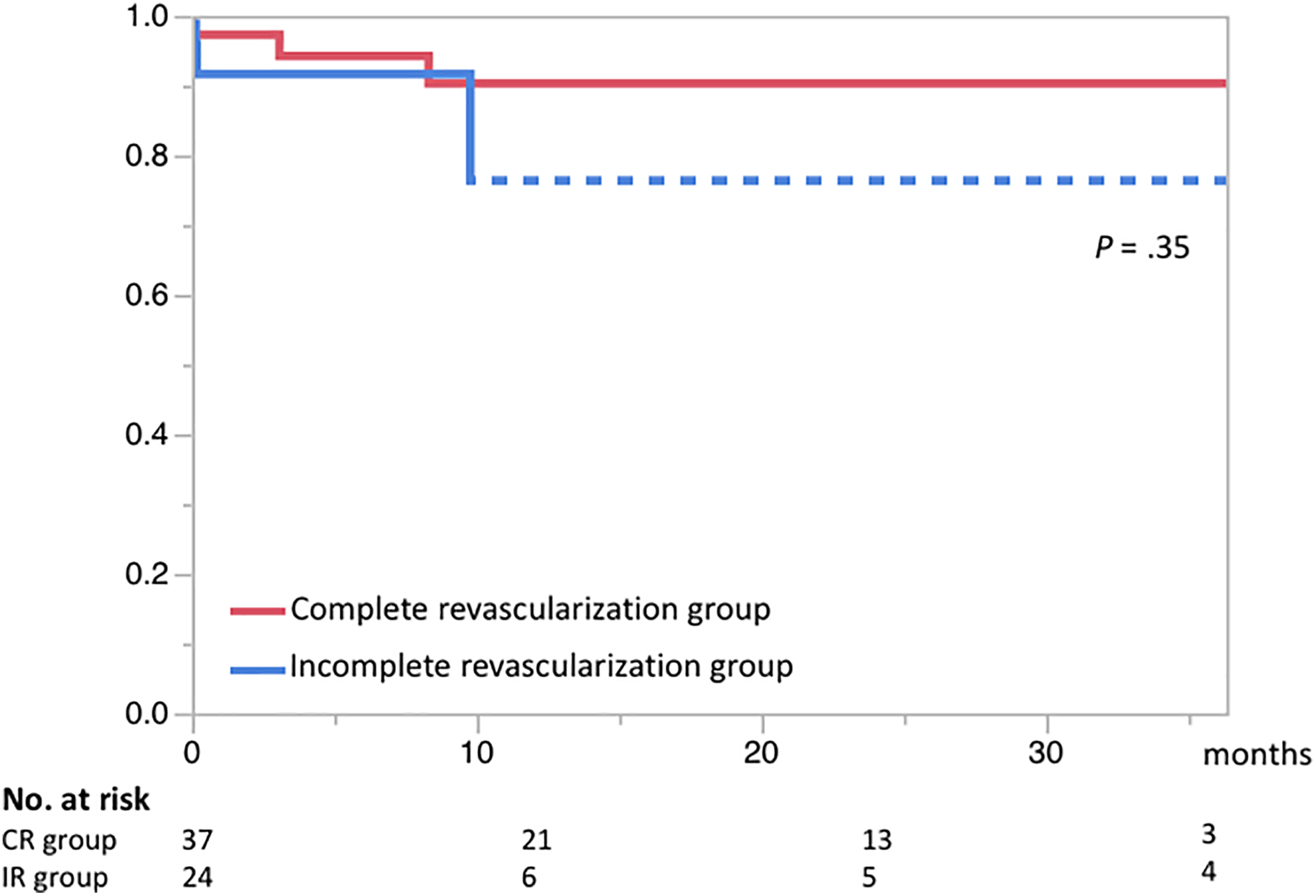
The primary patency rate at 3 years after the procedure was 64% in the CR group and 76% in the IR group (Figure 1). The assisted-primary patency rate at 3 years after the procedure was 81% in the CR group compared to 76% in the IR group (Figure 2). The secondary patency rate at 3 years after the procedure was 90% in the CR group and 76% in the IR group (Figure 3). The major amputation-free survival at 3 years after the index procedure was 97% in the CR group compared to 81% in the IR group (Figure 4).
Primary patency rates after the index hybrid procedure. Dotted line indicates standard error > 10%.
Assisted primary patency rates after the index hybrid procedure. Dotted line indicates standard error >10%.
Secondary patency rates after the index hybrid procedure. Dotted line indicates standard error >10%.
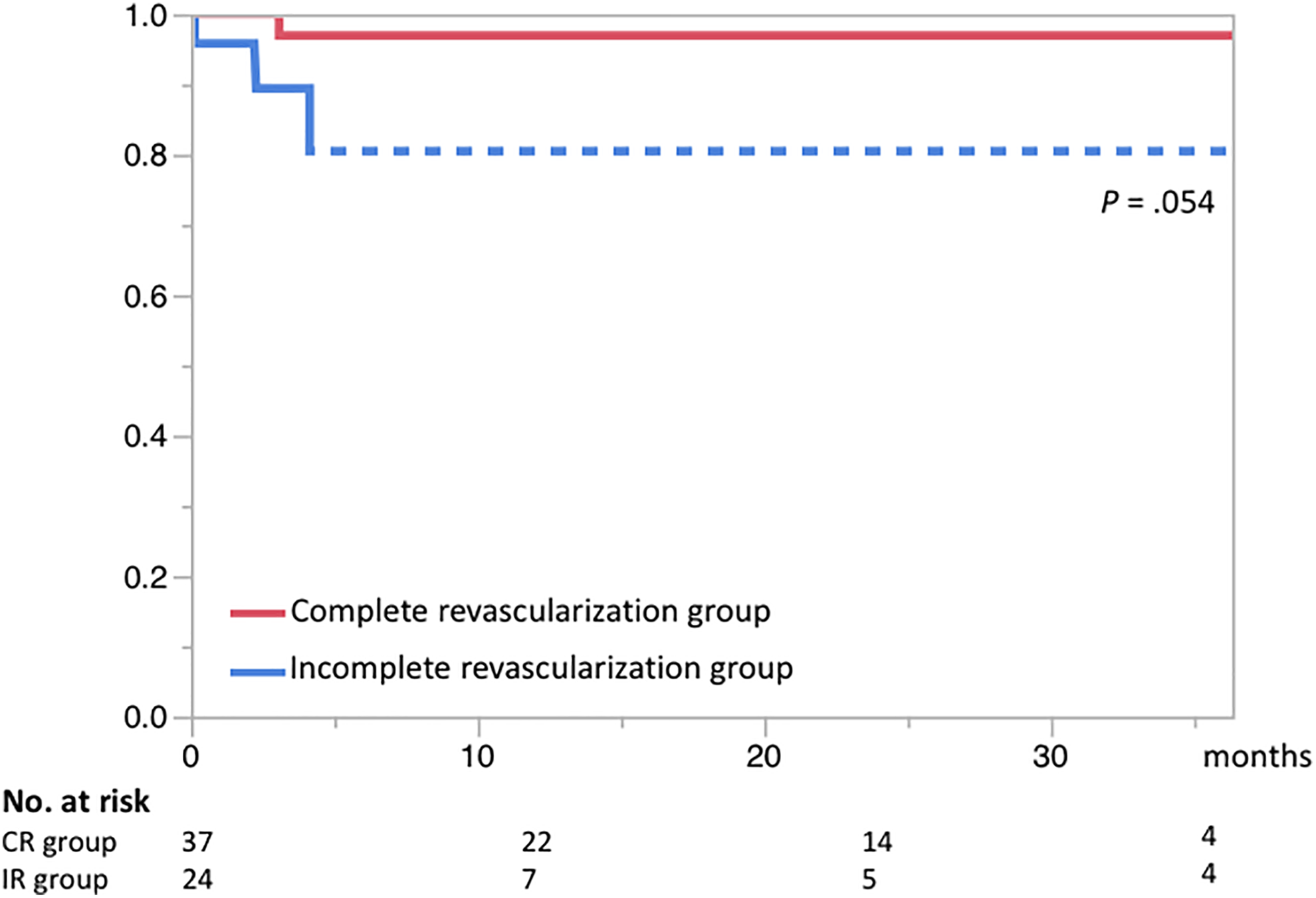
Major amputation-free survival rates after the index hybrid procedure. Dotted line indicates standard error >10%.
Discussion
For patients with CLI having multiple lower extremity arterial lesions involving the CFA, our study revealed that CR achieved by the hybrid procedure had more favorable outcomes than IR. In patients who underwent CR, fewer major amputations were required than in those who underwent IR, with higher postoperative ABI values and fewer reinterventions. Complete revascularization provides the ischemic foot with a direct blood flow, which improves wound-healing potential and drastically reduces the patient’s pain. Complete revascularization also benefits the patency of the target lesions by providing a better runoff vascular bed. The present results suggest that all patency indicators—primary, assisted primary, and secondary patencies—were superior in the CR group. Notably, procedure durations for CR and IR were similar, which does not necessarily mean that CR was easy and convenient but may indicate that patients with less complex lesions should undergo CR. In particular, the existence of tibioperoneal lesions affected the procedure. In our patient series, there were more patients with no tibial or peroneal runoffs in the IR group, whereas the TASC-II classifications of iliac and femoropopliteal artery lesions were similar between the groups.
Some clinicians advocate multiple tibioperoneal runoffs over a single tibioperoneal runoff for patients with CLI; we set our definition of CR as the achievement of at least 1 inline flow to the foot. Kobayashi et al, who analyzed 123 patients with CLI having foot tissue loss undergoing tibial angioplasty, reported that patients with 2 tibial artery runoffs had superior limb salvage rates at 3 years to those with 1 tibial artery runoff (93.9% vs 85.6%). 7 It is logical that multiple supply lines are superior to single supply line; however, this is not always achievable in real patients. We believe that our major amputation-free survival rate at 3 years (97.3%) is high enough to justify our definition of CR.
To devise a treatment strategy for patients with CLI having multiple levels of lower extremity arterial lesions, it is useful to categorize the lesions into 4 segments: (1) aortoiliac segment, (2) CFA and PFA segment, (3) SFA and popliteal artery segment, and (4) tibioperoneal artery segment. First, for aortoiliac segments—in other words, inflow segments—EVT is already the first-line therapy, and its long-term durability is well established. 8 –10 In our series, despite 89% of aortoiliac lesions being TASC-C or D, 96% of lesions were successfully treated by EVT. The remaining 4% were treated via femorofemoral crossover bypass.
Second, for CFA and PFA segments, open endarterectomy remains the gold standard, despite recent developments in endovascular technology. Atherosclerotic plaques in CFA are often bulky and heavily calcified; thus, placing a metallic stent in CFA is undesirable as CFA is located in the highly flexible hip joint and the CFA is an important access point for various endovascular procedures. Endovascular treatment is not suitable for the PFA. Profunda femoris artery lesions are often complicated with SFA occlusions, and in these circumstances, the PFA provides a critical collateral network bypassing the SFA. When attempting revascularization of PFA for such patients, technical success should be guaranteed, as jeopardizing the PFA blood flow often results in a major amputation. An open endarterectomy of the femoral artery, direct removal of atherosclerotic plaque, and patch angioplasty with profundaplasty as required through a minimal incision is, therefore, a reliable treatment option, as it warrants technical success with long-term durability and patency of the femoral artery. 3,11 Furthermore, endarterectomy with patch angioplasty can maintain the accessibility of CFA for simultaneous and future endovascular procedures.
Third, for the SFA and popliteal artery segments, TASC-II guidelines recommend EVT for TASC-A and B lesions and open bypass surgery for TASC-C and D lesions. 1 Recently, however, TASC-C and D lesions have been commonly treated by EVT, and acceptable long-term results have been reported. 12 –14 New devices, particularly drug-eluting stents and drug-coated balloons, are promising in this segment. 14 More EVT options for patients with CLI are urgently required, particularly as the baseline conditions of such patients are often too poor to perform a bypass surgery that requires general anesthesia. In our series, 100% of TASC-A, B, and C femoropopliteal lesions and 77% of TASC-D femoropopliteal lesions were treated by EVT.
Fourth, for tibioperoneal artery segments, EVT is not commonly utilized, as the lesions in this segment are often diffuse and highly calcified in naturally small arteries. Our first treatment choice for tibioperoneal lesions was bypass surgery using vein graft. We routinely screened the quality of great saphenous vein, small saphenous vein, and arm veins preoperatively by duplex ultrasonography on all patients. When there was no good-sized veins available, our second treatment choice was EVT. Lack of high-quality veins, therefore, could impact on our outcomes. In fact, there was 1 patient with long occlusion of posterior tibial artery, lacking good-sized veins. We tried to recanalize the lesion by bidirectional approach, antegradely from the endarterectomized site and retrogradely from a puncture at the distal posterior tibial artery. Despite our efforts, however, we failed to recanalize the lesion due to its length and severe calcification. According to Muir et al who reported outcomes of EVT for patients with CLI having tibioperoneal occlusive disease, the presence of more than 2 diseased vessels was associated with higher reintervention and amputation rates. 15 Stenting in this segment may be harmful; a single-center randomized controlled trial involving patients with CLI from infrapopliteal lesions reported that the 1-year primary patency rate of balloon angioplasty was 66% and that of primary stenting using bare-metal stent was 56%. 16 A drug-coated balloon technique also failed to prove its benefit in a randomized controlled trial. 17 Open bypass surgery is, therefore, still the most reliable option for patients with CLI having diffuse, long-segment tibioperoneal lesions.
Taking all aforementioned factors into consideration, creating a treatment plan for a patient with CLI having multiple lower extremity arterial lesions requires a decision on how to combine the 3 major treatment arms—EVT, open endarterectomy, and open bypass surgery—based on the target lesion complexity and the patient’s underlying conditions. Specifically, when the CFA (along with the proximal PFA) is involved, a hybrid procedure provides the widest range of treatment options, aiming for CR via minimal invasion. 4,18 Once the plaque build-up in CFA has been removed via endarterectomy, subsequent EVT procedures can be performed seamlessly for both inflow and outflow lesions via direct access. Even for in the most challenging of situations, for example, a patient with CLI having 4 diseased segments, recanalizing the inflow by EVT following femoral endarterectomy and performing bypass surgery for extensive outflow lesions will ultimately accomplish a CR as long as the patient has a good bypass target with an appropriate bypass graft conduit. In the meantime, our study data indicated that the limb outcome of patients who failed to accomplish a CR was not horrible. The major amputation-free survival rate at 3 years after the index procedure in the IR group was 81%. This result suggests that maximum effort of revascularization on the index procedure combined with careful postoperative maintenance cares warrant reasonable outcomes for patients with CLI, even without a good bypass target or an appropriate bypass graft conduit.
In our study cohort, there were 4 patients with hemodialysis in total (2 in each group). Although the hemodialysis rates did not differ significantly in 2 groups, higher major amputation rate in the IR group could be attributable to its higher hemodialysis rate. Hemodialysis patients’ limb outcomes were indeed poor in both groups; 1 patient in the CR group and 2 patients in the IR group resulted in major amputation. In other words, 3 of 4 major amputations occurred in patients with hemodialysis. These results suggest that clinicians pay special attention to patients with hemodialysis.
There are some limitations to the present study. This is a retrospective, single-centered study with a small patient group, and the follow-up period had a wide range. As a result, we had to combine Rutherford 4 and 5 patients together to increase the reliability of statistical analysis. We also failed to show statistically significant differences between the 2 groups on several important variables, including major amputation-free survival rate, although our results still suggest the benefit of CR for patients with CLI. We attribute this failure to the lack of power, and consistent results from a prospective, randomized controlled trial or a well-designed outcome study with a large number of propensity-matched patients would support our findings.
Conclusion
For patients with CLI having multiple lower extremity arterial lesions involving the CFA, the present hybrid procedure provides a wide range of treatment options. Complete revascularization, which was defined as the achievement of at least 1 in-line flow to the foot, was beneficial in terms of avoiding major amputation, without a longer procedure or hospital stay, when compared to IR.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.