
Abstract

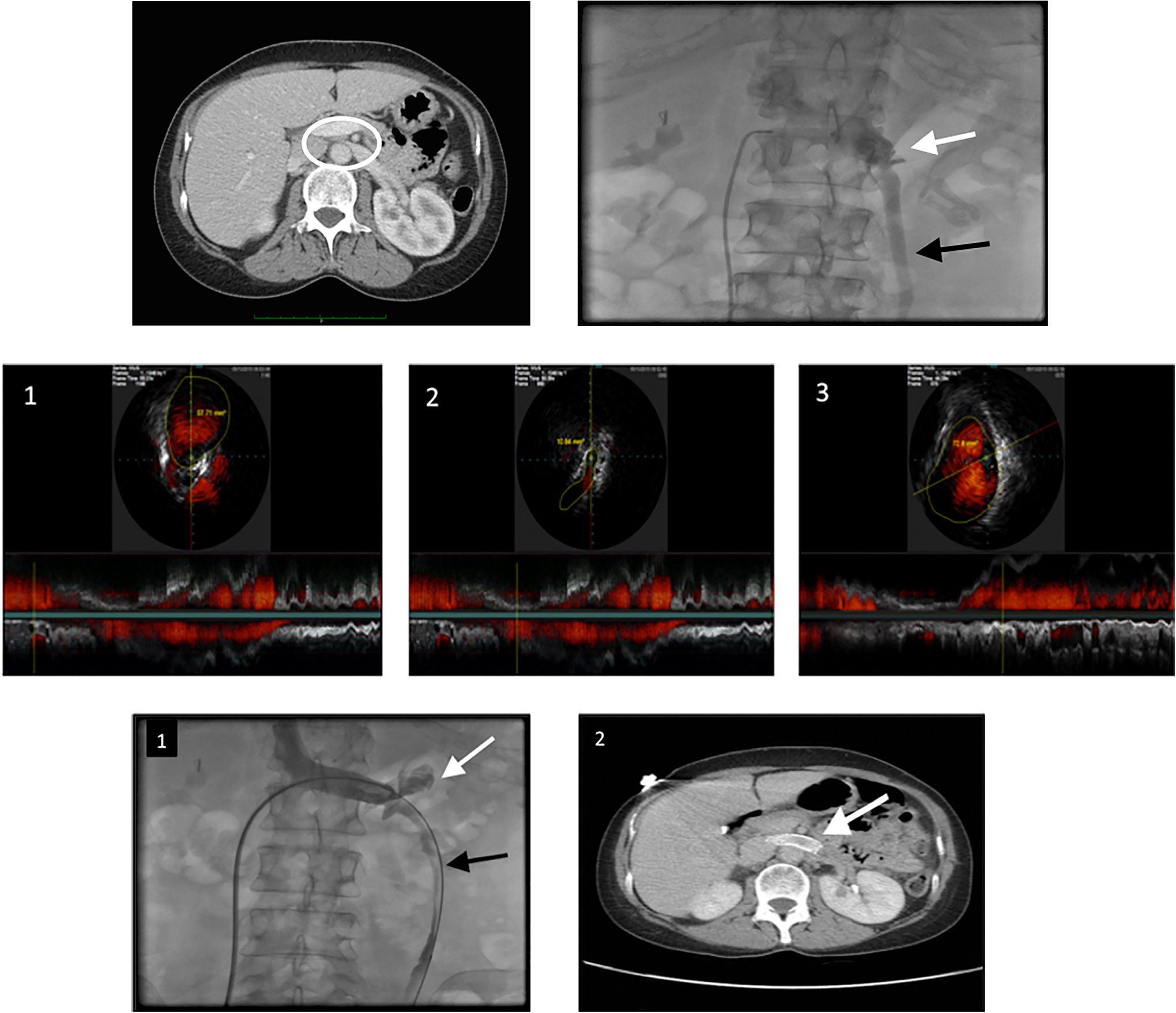
A 53-year-old female with a history of hypertension, carotid artery disease, and hyperlipidemia was referred for endovascular management of nutcracker syndrome (NCS). She presented with left-sided abdominal pain and microscopic hematuria. Diagnosis of NCS was made based on elevated peak velocity in the left renal vein (LRV) at the aortomesenteric junction in Doppler studies and severe compression of the LRV between the superior mesenteric artery and the abdominal aorta (circle) causing significantly enlarged left kidney with signs of pelvic venous congestion on computed tomography (CT) scan with contrast (Panel A). The LRV was engaged with 5F, JR4 diagnostic catheter, and venogram was obtained which showed severe compression of proximal–mid segment of the LRV (white arrow) with dilated left ovarian vein (black arrow, Panel B; Supplemental Video 1). The LRV was then wired with Supercore and further evaluated with intravascular ultrasound (IVUS), which confirmed severe compression of proximal–mid segment (Panels C1-C3; Supplemental Video 2). The affected segment was treated with percutaneous angioplasty using Evercross 5 × 40 mm followed by 10 × 40 mm Optapro balloons at low pressures. Post angioplasty, a 12 × 40 mm Protege stent was deployed in the LRV. This immediately improved the antegrade flow in the left gonadal and renal veins leading to significantly reduced flow to the collaterals (Panel D1; Supplemental Video 3). The vessel was then reevaluated with IVUS, which demonstrated well-apposed stent. She subsequently had alleviation of her symptoms. She was maintained on dual antiplatelet therapy with aspirin 81 mg and clopidogrel 75 mg for 3 months. The CT scan performed 6 months later for a different indication showed patent stent in the LRV and significant reduction in the size of the left kidney (Panel D2). Nutcracker syndrome is a clinical syndrome secondary to the compression of the LRV between the aorta and the superior mesenteric artery. 1 It is traditionally treated with open surgical correction and a number of surgical techniques have been described. 1 More recently, endovascular stenting is being used to treat NCS. 2–3 We performed IVUS-guided endovascular stenting of the LRV. The use of endovascular imaging such as IVUS in sizing and assessing the apposition of stents may prevent potential stent-related complications such as stent migration.
A, Computed tomography (CT) scan with contrast—Severe compression of the left renal vein (LRV) between the superior mesenteric artery and the abdominal aorta (circle) with significantly enlarged left kidney. B, Severe compression of proximal–mid segment of the left renal vein (LRV; white arrow) with dilated left ovarian vein (black arrow). C, Intravascular ultrasound (IVUS) showing compression of the left renal vein in proximal–mid segment (1 distal to the compression, 2 site of compression, and 3 proximal to the compression). D1, Venogram after stent deployment with significantly improved antegrade flow in the left renal vein (white arrow) and the gonadal vein (black arrow) with reduced flow to the collaterals. D2, Follow-up computed tomography (CT) scan showing patent stent in the left renal vein with significant reduction in the size of the left kidney.
Footnotes
Authors’ Note
Informed consent has been obtained from the patient for publication of the case report and accompanying images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.