
Abstract
Cancer-associated vein obstruction (CAVO) is a common complication in oncological patients, but the effective therapeutic options are scant. We report a patient with reiterative recurrent CAVO who was successfully treated with intraluminal brachytherapy using a self-expandable stent loaded with linear radioactive iodine-125 seeds (RIS) strand. During follow-up, her clinical symptoms were well improved. Three-month imaging follow-up revealed satisfactory patency of the iliofemoral vein, and the stents combined with RIS strands performed well. No serious complications associated with the implantation of stent and RIS strands were documented in any of the sessions. Intraluminal brachytherapy using a self-expandable stent loaded with linear RIS may be a safe and effective option for CAVO as long as it includes not only blood flow restoration but also brachytherapy administration for cancer.
Introduction
Cancer-associated vein obstruction (CAVO) is a common complication in oncological patients. The symptoms are nonspecific, and patients commonly present with intractable recurrence of thrombi. 1 Epidemiological studies have suggested that the cumulative risk of recurrence in these patients is as high as 21%. 2 Stent implantation after transluminal balloon venoplasty is widely accepted as a palliative treatment because of its ability to promptly restore the natural blood flow and thus improve quality of life. However, stent dysfunction, primarily in the form of tumor ingrowth, overgrowth, or mucosal hyperplasia in the stent, remains challenging. 1,3 –5 These problems continue to occur despite the emergence of various novel stents, including covered stents and drug-eluting stents. 3 Cancer-associated vein obstruction can compromise quality of life and increase financial burdens. Currently, the therapeutic options for CAVO are limited.
Recently, intraluminal brachytherapy using radioactive iodine-125 seeds (RIS) was reported to be safe and effective for portal vein tumor thrombosis (PVTT). 4,5 Therefore, we hypothesize that this approach may also benefit patients with CAVO. To the best of our knowledge, this treatment has not been previously reported. We report a case in which a self-expandable stent combined with linear RIS was used to treat CAVO recurrence. The outcome was relatively positive.
Case Report
We obtained written informed consent from the patient for the use of clinical materials for research purposes. We also obtained approval from the Institutional Ethics Board of the Nanjing First Hospital, Nanjing Medical University (Nanjing, China).
Clinical History
A 75-year-old Chinese woman was readmitted to the interventional radiology department with recurrent symptoms of reddish swelling, pain, and difficulty with walking on the right leg, which she experienced intermittently for approximately 10 months. The physical examination was unremarkable, except for severe pitting edema of the right thigh and ankle. The difference in circumference between the patient’s lower extremities was 4.6 cm (left, 31.5 cm; right, 36.1 cm). The ankle was tender to palpation with positive Homans and Moses signs. Laboratory results were remarkable for

Supplementary ascending venography via the dorsal vein and CTV of the right lower extremity. A-D, Venography confirming extensive occlusion of the trunk of the right femoral vein, iliac vein, and inferior vena cava, with extensive collaterals. E and F, Computed tomography venography revealed intrastent thrombi. CTV indicates computed tomographic venography.
Her medical history was significant for moderately differentiated rectal adenocarcinoma 5 years prior to presentation. The cancer stage was IIA. At that time, she underwent radical surgical resection in addition to 6 courses of chemotherapy (CapeOx therapy, L-OHP 200 mg intravenous glucose tolerance test on day l, and Xeloda 1.0 g orally days 1-14) and 3 cycles of radiotherapy. Approximately 10 months prior to presentation, the patient developed progressive pain and swelling in the entire right lower extremity. A duplex scan revealed substantial thrombotic masses in the right common iliac vein. She underwent 1 week of anticoagulant therapy with continuous low-molecular-weight heparin (LMWH). However, her symptoms did not improve, and she was admitted to our department. Venography findings indicated complete occlusion of the trunk of the right iliofemoral vein extending anterograde into the IVC, with no floating thrombi below the iliac vein. After obtaining informed consent, the patient underwent initial percutaneous transluminal angioplasty (PTA) with a 10-mm × 80-mm-diameter balloon catheter (Cordis Corporation, Miami, Florida) followed by a combination of 12 mm × 120 mm stent implantation (Luminexx; C. R. Bard, Murray Hill, New Jersey) and repeat PTA (10 mm × 80 mm; Cordis Corporation) due to concern regarding greater than 50% narrowing of the diameter of the vein. Subsequently, she was treated with alteplase (Actilyse; Boehringer-Ingelheim, Ingelheim am Rhein, Germany) through a multiside hole catheter for 24 hours. However, repeat venography revealed persistent obstruction in the stent. Therefore, repeat PTA was performed, and 14 mm × 90 mm and 12 mm × 90 mm stents (Wallstent; Boston Scientific Co, Ltd, Marlborogugh, USA) were implanted. Simultaneously, we aspirated thrombi through the catheter for pathological examination, which confirmed differentiated adenocarcinoma. Immunohistochemistry revealed ck7(−), ck20(−), cdx2(3+), satb2(2+), cd31(−), and ki-67 (60%). Three months after the first interventional treatment, she experienced recurrent swelling and pain in the right extremity, similar to her previous symptoms. She underwent catheter-directed thrombolysis (CDT) with alteplase administered at 0.01 mg/kg/h in normal saline (20 mg in 500 mL of 0.9% saline). Forty-eight hours later, complete venography revealed improvement in the occlusion volume. However, residual irregular intrastent stenosis remained. She was discharged to home. One month later, she was readmitted and underwent CDT once again as previously described in addition to adjunctive PTA with a 12 mm × 80 mm balloon (Cordis Corporation). Two months after the last interventional treatment, the patient was readmitted to our department for the same symptoms. During every treatment, LMWH (Hebei Changshan Biochemical Pharmaceutical, Shijiazhuang, China) therapy was overlapped with 15 mg of oral rivaroxaban twice a day.
Treatment
Upon admission, we initiated anticoagulant treatment with subcutaneous LMWH at a bolus dose of 4100 units per 12 hours. After appraising her condition, we developed a therapeutic plan: placement of a self-expanded stent loaded with RIS (Junan Pharmaceutical Ltd, Ningbo, China) to manage the recurrent obstruction. The RIS used were composed of cylindrical titanium capsules, 0.8 mm in diameter and 4.5 mm in length, and the radioactive dose per seed was 0.54 mCi, as previously described. 1 The RIS strand was constructed using 40 RIS (estimated by software) arranged linearly in a 4F sterile plastic tube (Wallstent; Boston Scientific Co, Ltd). The ends of the catheter were sealed by heat. The seed strand was expected to extend 10 mm proximal and distal to the stricture to prevent tumor invasion of either end.
Under regional anesthesia with lidocaine, percutaneous access to the thrombosed vessel was achieved through the dilated right femoral vein, and a 7F sheath (Neff Set; Cook, Bloomington, Illinois) was introduced. After confirmation of placement in the true lumen, an H1 catheter (Cordis Corporation) was passed through the occluded segment with the assistance of a 0.035-in guide wire (Cook) and advanced into the IVC. Then venography was performed through a multiside hole catheter (Figure 2A). Next, 0.035-in, 260-cm-long stiff wires (Terumo, Tokyo, Japan) were exchanged and left in place. Secondary venous access was achieved approximately 5 cm below the 7F sheath. A 5F, 30-cm sheath was introduced. The patient underwent initial intrastent PTA with a 12 mm × 60 mm balloon (Cordis Corporation; Figure 2B). According to the measured length of the occlusion, a 14 mm × 90 mm self-expandable stent (Wallstent; Boston Scientific Co, Ltd) was deployed along the stiff wires across the occluded segment (Figure 2C). The distal segment of the first stent was placed into the proximal segment of the IVC, whereas the proximal segment of the second 12 mm × 90 mm stent (Wallstent; Boston Scientific Co, Ltd) was situated within the previously placed stent. Then 12 mm × 80 mm balloon dilation (Cordis Corporation) was performed to facilitate stent insertion (Figure 2D). An RIS strand was placed through the 5F sheath. When the sheath was withdrawn, the RIS strand was fixed in place between the stent and the vessel wall (Figure 2E). However, postprocedure venography revealed acute intrastent thrombosis. After 18 hours of CDT, blood flow was restored, and satisfactory stent patency and good positioning of the radioactive seeds were observed (Figure 2F). In addition, the patient was advised to return to our department 3 months after the last intervention.
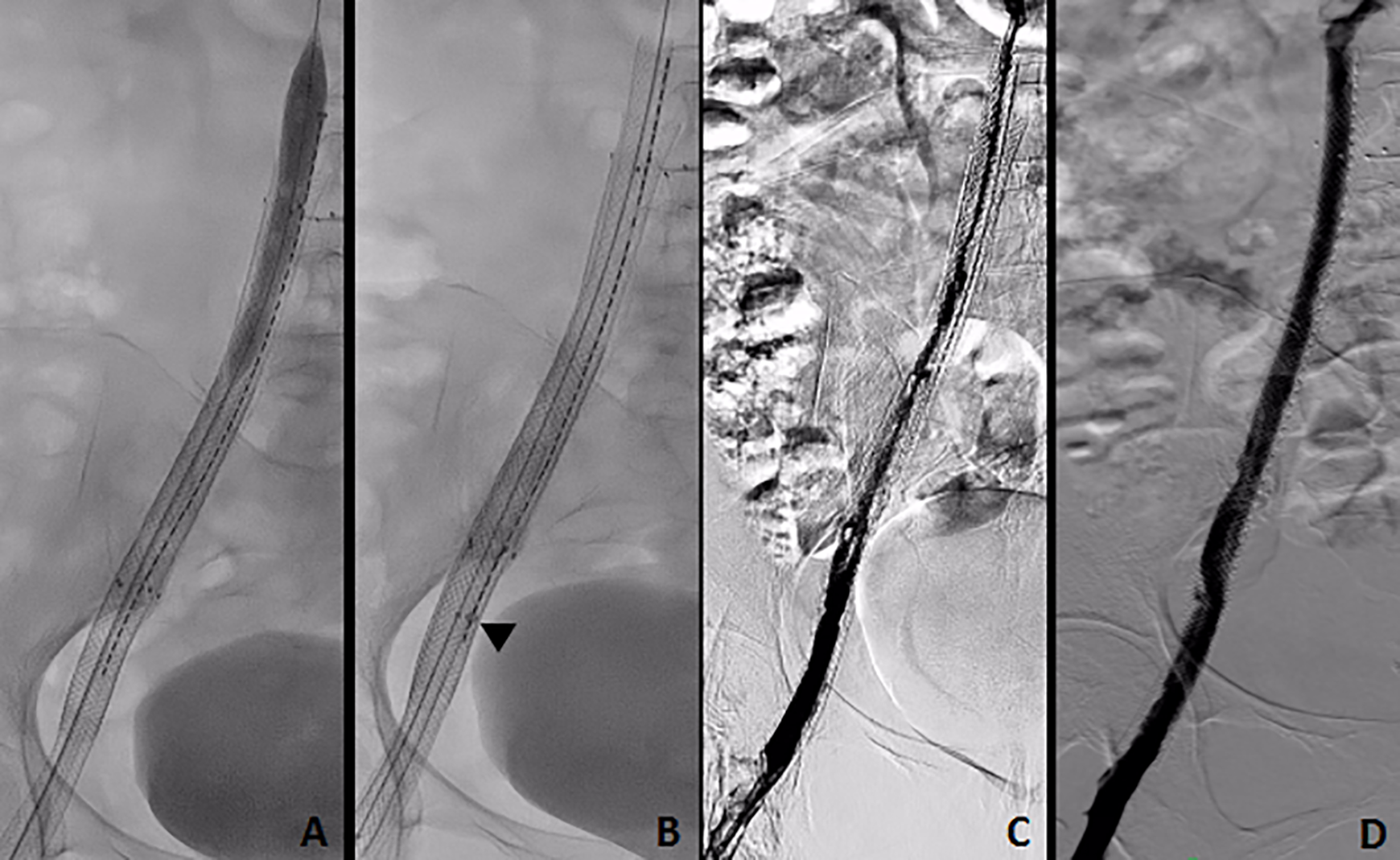
Treatment procedure and outcome before discharge. A, Intraluminal venography through the inserted catheter. B, Initial intrastent PTA of the obstructed segments. C, Two self-expandable stents and RIS strands loaded with 40 radioactive seeds were placed across the occluded segment. D, Balloon dilation was performed to facilitate stent insertion. E, The sheath was withdrawn (arrow), and the RIS strand was fixed in place between the stent and the vessel wall. F, After 18 hours of CDT, blood flow was restored, and venography revealed satisfactory stent patency and favorable positioning of the radioactive seeds. CDT indicates catheter-directed thrombosis; PTA, percutaneous transluminal angioplasty; RIS, radioactive iodine-125 seeds.
Outcome and 3-Month Imaging Follow-Up
The follow-up period began after the date of RIS stent implantation. The outcome was assessed at discharge and 3 months after treatment. All clinical symptoms, including swelling, pain, and difficulty with walking, were improved, and the difference in circumference between the patient’s lower extremities was 0.5 cm (left, 31.5 cm; right, 32 cm). The patient’s quality of life was evaluated using a validated Norwegian version of the generic quality of life instrument, the EuroQol (EQ-5D) self-report questionnaire, which includes 5 items: mobility, self-care, activity, pain, and anxiety. 6 The patient’s score was 0.824, reflecting high quality of life. At 3 months, pelvic contrast-enhanced computed tomography images revealed a slightly reduced tumor size without the occurrence of new lesions. Venography demonstrated satisfactory patency of the iliofemoral vein, and the stents combined with RIS strands performed well (Figure 3A-D). The patient had no serious complications associated with stent and RIS strand implantation. One month later, the patient was followed up via telephone, and she reported that she was doing well, with a similarly high EQ-5D score compared to her previous score. Oral anticoagulation was continued.
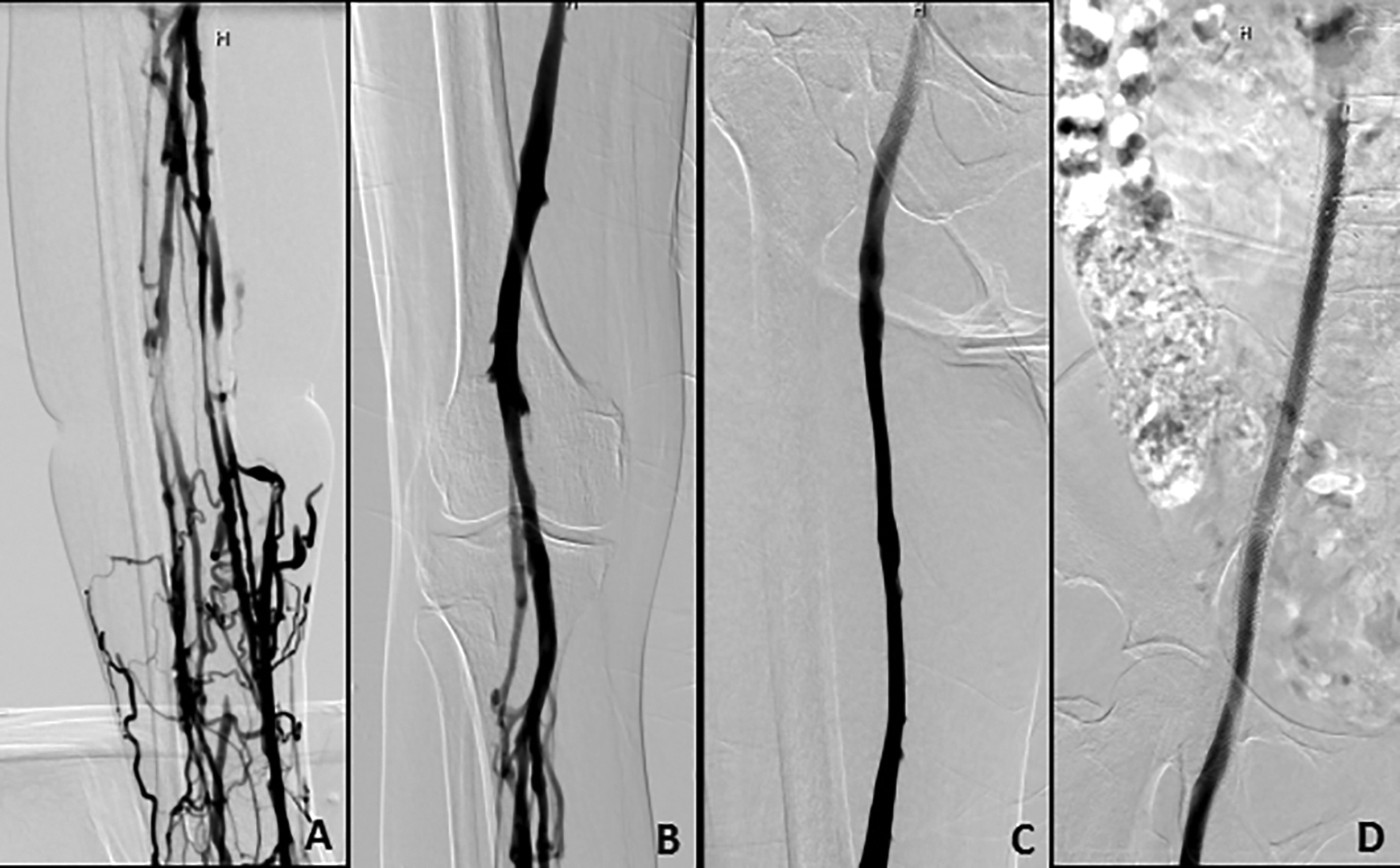
Repeat venography at the 3-month follow-up. A-D, Satisfactory patency of the iliofemoral vein, with good performance of the stents combined with RIS strand. RIS indicates radioactive iodine-125 seeds.
Discussion
No substantial progress has been achieved for the treatment of vein obstruction caused by malignant cell invasion. Nevertheless, radical correction may be considered the preferred therapy when possible. However, for patients with cancer in advanced stages, surgical resection may not be indicated. Various treatment modalities, including anticoagulation, CDT, chemotherapy, and radiotherapy, remain the conservative methods for inoperable patients. However, these methods are unsuitable as primary therapy for CAVO due to poor associated responses and prognoses. Furthermore, blood flow cannot be restored immediately using these methods alone.
For palliative management of vein obstruction, stent implantation remains a viable option. Symptoms can be relieved rapidly as a result of obstruction resolution by bare metal stent insertion, thus enabling subsequent therapy. However, this approach offers minimal benefit in the absence of regional therapy for gradually growing tumors. Occlusion, which is almost inevitable for long-term survivors, is mostly caused by tumor overgrowth, as reported by Lee et al 7 and as observed in our patient. Therefore, further control of tumor growth following stent insertion is required. Unfortunately, no consensus has been reached regarding the treatment of these patients. Recently, brachytherapy with interstitial RIS implantation has been used with promising results for the treatment of solid tumors, particularly in prostate tumors. 8 The insertion of self-expandable stents loaded with RIS has been established as a new treatment strategy, combining the advantages of rapid patency achievement and continuous brachytherapy administration to prevent obstruction. The modality was initially applied to treat unresectable esophageal cancer and was subsequently extended to biliary obstruction caused by various adenocarcinomas. 9,10 Recently, the use of stents loaded with RIS has been widely expanded from nonvascular to endovascular treatments, including PVTT venoplasty, where it has been shown to be safe and effective. 1 To the best of our knowledge, treatment of recurrent CAVO following multiple stent placements has not been reported.
In this report, a self-expandable stent loaded with linear RIS strand was an effective treatment for our patient with recurrent CAVO. After she underwent irradiated stent placement in addition to adjunctive CDT, her symptoms of swelling and pain secondary to great vessel obstruction were relieved. Blood flow was restored in the obstructed vessel, and the high venous pressure caused by tumor thrombi was reduced. Simultaneously, the growth of the tumor thrombi slowed. This report actually describes RIS-loaded stent-in-stents. The stent-in-stent style may increase mesh density. Furthermore, the patient was treated with linear RIS strand using the appropriate number of RIS within a 4F tube according to the length of the occluded segment based on venography. Therefore, the device resembles a covered stent with radioactivity. Sustained low-dose irradiation causes cell death by apoptosis. The RIS strand in the vein delivers sustained irradiation to the tumor and can oxygenize hypoxic cells, thus increasing the tumor cells’ sensitivity to irradiation, as reported previously. 11 Intraluminal brachytherapy was expected to play a role in antihyperplasia and antitumor ingrowth and therefore ensures a higher stent patency rate. In addition, this approach has several advantages: (1) avoiding vascular injury caused by repeated puncture, (2) accurate fixation of an RIS strand in tumor thrombi with expansion of the stent, which prevents RIS loss or displacement, and (3) decreased damage to surrounding normal tissues due to the long half-life (59.43 days) and short radiation distance. Conversely, inhibition of tumor cell replication, apoptosis, and neointimal hyperplasia reduce the incidence of restenosis after stent placement, thus prolonging stent patency. 12
Although there was a concern that the stent loaded with RIS may lead to procedure-related adverse events, including adjacent organ injury and vessel wall injury, these events did not occur during delivery, deployment, or the follow-up. Neither the stent nor the RIS strand migrated based on imaging. Therefore, we consider this technique to be an effective method for restoring blood flow. Currently, no standard recommendation is available regarding the radiation dose for RIS used in brachytherapy of vessels. Sindelar and Kinsella 13 reported that the radiation tolerance dose of great vessels is greater than 800 Gy. The radiation dose delivered by RIS is inversely proportional to the distance from the seeds, which can deliver a high radiation dose to the target tissues that decreases rapidly with increasing distance from the seeds, resulting in low radiation doses delivered to surrounding tissues. Therefore, RIS enable the delivery of a high radiation dose to tumor tissues while minimizing injury to normal tissues. In this study, the average absorbed doses were apparently lower than the tolerated dose.
Conclusion
A 75-year-old woman with recurrent CAVO from resected rectal cancer was successfully treated with a self-expandable stent loaded with linear RIS strand, resulting in restoration of blood flow and enabling intraluminal brachytherapy. This technique may represent a novel approach for prolonging vessel patency in these patients. This case report may provide guidance for future studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Clinical Medicine Science and Technology Projects of Jiangsu Province, China (BL2014013) and the Nanjing Medical Science Fund, China (YKK14087).