
Abstract
Background:
Pregnancy is a hypercoagulable state, conferring an increased risk of venous thromboembolism (VTE). However, treatment algorithms for deep venous thrombosis and pulmonary embolism are based on studies of nonpregnant patients.
Methods:
A literature review of cases in which thrombolysis was used for the treatment of VTE during pregnancy was conducted using the PubMed (National Institutes of Health) database.
Results:
A PubMed database search of English language articles for reports of thrombolysis for the treatment of VTE in pregnancy identified 215 cases, including 183 cases of systemic thrombolysis, 19 cases of catheter-directed thrombolysis, and 13 cases of mechanical thrombectomy. For systemic thrombolysis, the maternal complication rate was 4.40% and the fetal complication rate was 1.65%. For catheter-directed thrombolysis, the maternal complication rate was 14.75% and the fetal complication rate was 5.2%. In cases of mechanical thrombectomy, there were no reported maternal or fetal complications.
Conclusions:
Although conservative strategies are preferred in pregnancy, thrombolysis is an adjunct for limb or life-threatening VTE. Review of past reports suggests low rates of maternal and fetal complications following systemic thrombolysis and mechanical thrombectomy but higher rates of complications after catheter-directed thrombolysis in the treatment of VTE during pregnancy.
Keywords
Introduction
Venous thromboembolism (VTE) complicates 2 of 1000 deliveries 1 and is a major contributor to maternal morbidity and mortality. 2,3 Pregnant women are 5 times more likely to develop VTE than nonpregnant women, with the highest risk during the third trimester and postpartum period. 1,4 Although catheter-directed thrombolysis (CDT) has been established as a safe and effective treatment for VTE in nonpregnant patients, pregnant patients were excluded from these trials. 5,6 We review indications, techniques, and maternal and fetal outcomes following systemic thrombolysis, CDT, and mechanical thrombectomy from case reports in the available literature.
Mechanisms and Complications of Hypercoagulability During Pregnancy
Normal pregnancy is associated with a myriad of hematologic changes, resulting in a hypercoagulable state. Platelet count, protein S, and activated protein C levels fall, while procoagulant factors VII, VIII, IX, X, XII, fibrinogen, and von Willebrand factor rise. 7,8 Endogenous fibrinolytic activity decreases due to reduced tissue plasminogen activator (tPA) activity and increased plasminogen activator inhibitor 1. 9
The risk of deep venous thrombosis (DVT) and pulmonary embolism (PE) increases throughout pregnancy, as procoagulant factors continue to rise in the third trimester. 7 Venous thromboembolism risk is increased 5-fold in pregnant women compared to nonpregnant women and can be up to 20-fold in the postpartum period. 1 Risk factors for VTE in pregnant women include African American race, previous VTE, inherited hypercoagulable disease, age over 35 years, multiparity over 4, cesarean delivery, smoking, and hyperemesis gravidarum. 10 –12
Complications of PE and DVT pose particular danger to mother and fetus. Pulmonary embolism is a leading cause of maternal mortality, 13 and PE with hemodynamic compromise endangers placental perfusion and fetal outcomes. In the long term, surviving patients with PE report functional limitations in 50% of cases, with residual abnormal pulmonary artery pressures and right ventricular function remaining in up to 30% of surviving patients. 14
Postthrombotic syndrome (PTS) occurs in 50% of patients with DVT and is secondary to thrombotic inflammation and injury to venous valves. 15 Risk factors for PTS include female gender, obesity, preexisting varicose veins, and iliofemoral location of DVT. 16 Although nonfatal, PTS is associated with reduced quality of life and can lead to venous stasis ulceration and infection. 17
Fetal complications of maternal VTE include fetal loss and intrauterine growth restriction. Maternal thrombophilias such as deficiencies in antithrombin, protein C, and protein S are associated with recurrent fetal loss, 18 suggesting an association between hypercoagulability and abortion or stillbirth. Similarly, women with preeclampsia or intrauterine growth restriction are more likely to have factor V Leiden mutation than healthy pregnant controls. 19 These findings suggest that maternal predisposition to VTE translates to poor fetal outcomes.
Materials and Methods
We utilized the MEDLINE (National Institutes of Health, Bethesda, Washington) database of indexed, peer-reviewed literature to identify English language articles with permutations of relevant search terms. Cases were excluded if patients did not receive treatment for VTE until the postpartum period. Major bleeding was defined in accordance with recommendations from the International Society on Thrombosis and Haemostasis as fatal bleeding, symptomatic bleeding in a critical area or organ, surgical site bleeding requiring reintervention, bleeding requiring transfusion of 2 units of packed red blood cells, or bleeding leading to hemodynamic instability. 20
For our review of systemic thrombolysis in pregnancy, all permutations of the search terms “thrombolysis,” “systemic thrombolysis,” “pregnancy,” “deep vein thrombosis,” “pulmonary embolism,” and “venous thromboembolism” were used.
For our review of CDT in pregnancy, all permutations of the search terms “catheter-directed thrombolysis,” “pregnancy,” “deep vein thrombosis,” “pharmacomechanical thrombectomy,” “pulmonary embolism,” and “venous thromboembolism” were used.
For our review of mechanical thrombectomy in pregnancy, all permutations of the search terms “mechanical thrombectomy,” “pregnancy,” “deep vein thrombosis,” “pulmonary embolism,” and “venous thromboembolism” were used.
Results and Review of Maternal and Fetal Considerations During Treatment for VTE
Systemic Anticoagulation During Pregnancy
Low-molecular-weight heparin (LMWH) is the preferred anticoagulant for pregnant patients with VTE. 21 Nelson-Piercy et al conducted a multicenter retrospective analysis of 1267 pregnancies that were treated with LMWH for VTE. In 262 pregnancies receiving therapeutic dosages of LMWH, the live birth rate was 98.9%, with 2 stillbirths and 1 termination, but no miscarriages. Low-molecular-weight heparin was also efficacious in treating VTE at a 2% recurrence rate, with 1 DVT and 4 PEs occurring after treatment. In the prophylaxis and treatment group combined, there were no maternal deaths, heparin-induced thrombocytopenia, or hematomas associated with neuraxial anesthesia. 22 Although LMWH in preventing PTS in pregnant patients has not been studied prospectively, studies of nonpregnant patients have shown that the treatment of DVT with LMWH is associated with significantly lower rates of PTS compared to treatment with a vitamin K antagonist. 23
Low-molecular-weight heparin is preferred over unfractionated heparin (UH), due to the latter’s association with reduced postpartum bone mineral density and increased risk of heparin-induced thrombocytopenia. 24,25 Multiple randomized controlled trials have shown noninferiority of LMWH to UH in treatment of acute DVT and nonmassive PE. 26,27
Warfarin is not recommended for use during pregnancy for VTE. Use of low-dose warfarin has been reported in pregnant women with mechanical heart valves with a 0.4% to 2.4% incidence of embryopathy and 8.4% to 24.7% incidence of fetal loss. 28 Warfarin’s low molecular weight enables passage through the placenta and its use is associated with abortion or stillbirth. 29 In surviving fetuses, the stereotypical features are nasal hypoplasia and epiphyseal stippling on radiographic imaging. 30 Less consistent but reported presentations include cleft lip, aortic coarctation, choanal atresia, or intraventricular hemorrhage. 31
Inferior Vena Cava Filter Placement During Pregnancy
There are no randomized controlled trials comparing inferior vena cava (IVC) filter placement in pregnancy to anticoagulated or nonanticoagulated controls. A systematic review of 124 pregnancies in which IVC filters were placed found 1 case of recurrent symptomatic pulmonary embolus and no instances of fatal PE. 32 An 8.87% complication rate included instances of failed retrieval, filter migration, and filter fracture. The 2012 American College of Chest Physicians Guidelines recommend placement of an inferior vena cava filter in patients with proven acute VTE in which anticoagulation is contraindicated, with a preference for retrievable filters in order to reduce long-term risks of complications in a generally young patient population. 21,33 Suprarenal placement is often performed to avoid uterine compression and subsequent fracture or migration of the filter. 34,35
Systemic thrombolysis during pregnancy
Recombinant tPA, streptokinase, and urokinase have not been shown to have teratogenic effects in animal studies. 36 –38 Given that pregnant women were excluded from trials utilizing thrombolysis for treatment of VTE, the advantages of one thrombolytic over another in treatment of VTE during pregnancy is not established. However, biochemical differences between recombinant tPA, streptokinase, and urokinase pose theoretical considerations for use in pregnant patients.
Compared to the other thrombolytics, recombinant tPA is more specific, activating plasminogen only in the presence of fibrin. 39 This offers a mechanistic advantage in reducing widespread thrombolytic activity and fibrin degradation products. Streptokinase is purified from Streptococci bacteria and is antigenic, reducing its ability to be used repeatedly. 40, 41 Urokinase is nonantigenic but also lacks the substrate specificity of recombinant tissue plasminogen activator (rtPA). 41
Our MEDLINE search for cases of systemic thrombolysis in pregnancy yielded 26 relevant case reports with 183 patients (Table 1). 41 The mean patient age was 28.8 years, with an average gestational age of 25.8 weeks. The most common indication was DVT (86.3%). The most commonly used thrombolytic was streptokinase (85.2%, N = 156), followed by alteplase (6.0%, N = 11) and urokinase (2.2%, N = 4). Only 2.1% of patients were found to have a hypercoagulable disorder during evaluation, which included antithrombin III deficiency, prothrombin G20210A mutation, and factor V Leiden mutation. However, the extent of a hypercoagulability workup was ambiguous in most reports, making it difficult to adjudicate whether the hematologic status of the remaining 97.9% of patients was negative or missing. Follow-up was only described in 4 reports and ranged from 5 months to 3 years, with no reports of PTS or PE recurrence.
Reports of Systemic Thrombolysis for Treatment of Maternal Venous Thromboembolism.
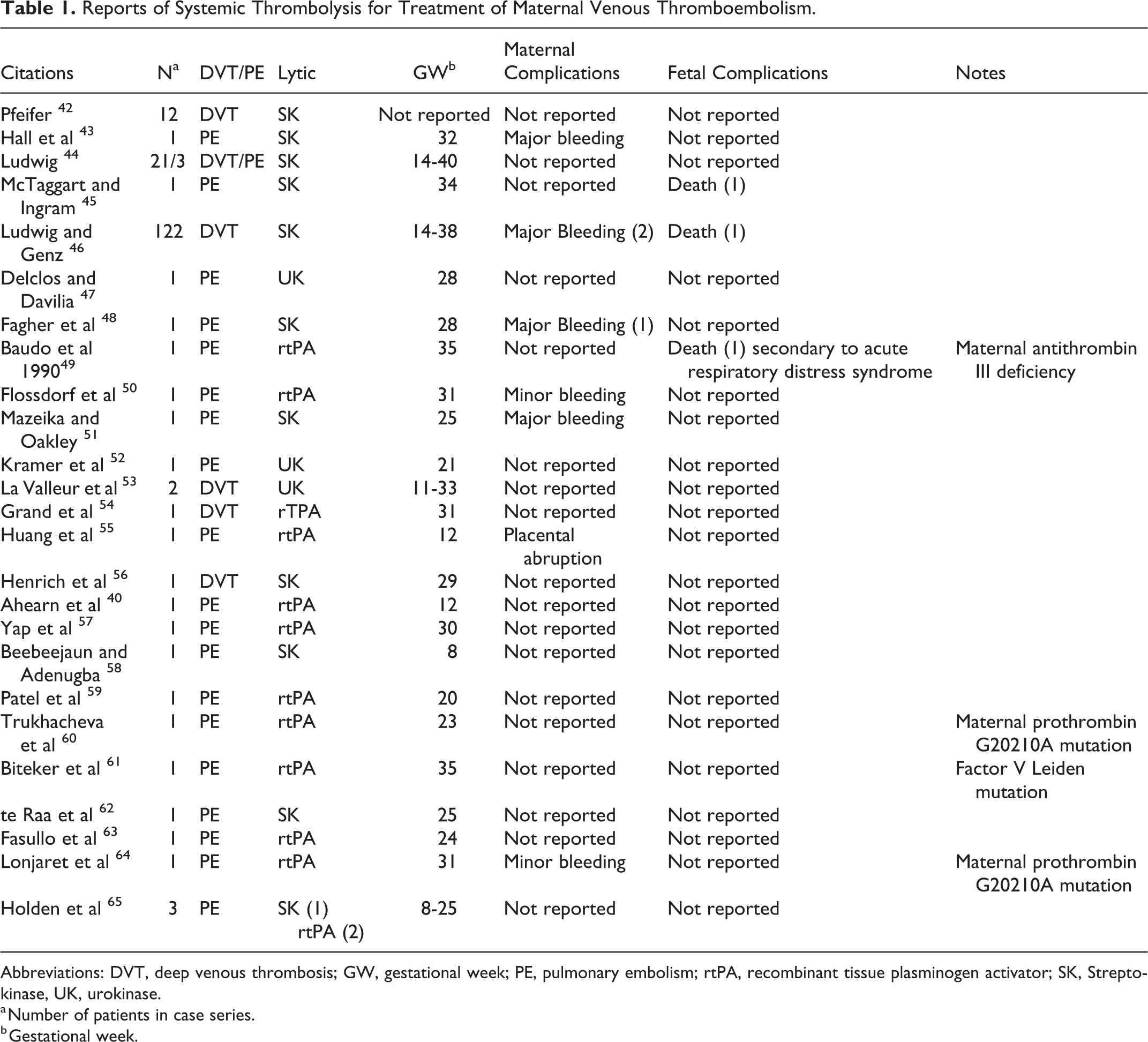
Abbreviations: DVT, deep venous thrombosis; GW, gestational week; PE, pulmonary embolism; rtPA, recombinant tissue plasminogen activator; SK, Streptokinase, UK, urokinase.
a Number of patients in case series.
b Gestational week.
The largest case series was reported by Ludwig and Genz who reported 122 cases of DVT treated with systemic streptokinase, with 2 events of maternal major bleeding and 1 fetal demise. 46 The maternal complication rate was 4.40%, with a 2.75% occurrence of major bleeding and 1 (0.55%) case of placental abruption. The fetal complication rate was 1.65%, entirely represented by fetal demise.
Catheter-Directed Thrombolysis During Pregnancy
In nonpregnant patients with DVT, there are few randomized controlled trials on the use of CDT. The catheter directed thrombolysis versus standard treatment for acute iliofemoral deep vein thrombosis study found a significantly lower rate of PTS in patients undergoing CDT with a higher risk of bleeding compared to systemic anticoagulation, 5,66 but only the latter finding was corroborated by the recent acute venous thrombosis: thrombus removal with adjunctive catheter-directed thrombolysis study. 67 In nonpregnant patients with DVT, the American College of Chest Physicians guidelines suggest that CDT is most likely to benefit patients with iliofemoral DVT with symptoms for less than 14 days, with good functional status, life expectancy of over 1 year, and a low risk of bleeding. 68
Our MEDLINE search yielded 6 relevant case reports with 18 patients (Table 2). The mean maternal age was 28 years, with an average gestational age of 31.6 weeks (range: 6-35 weeks). Two patients, or 10.5% of the cohort, were found to have a hypercoagulable disease (protein S deficiency, factor V Leiden mutation). The most common indication was DVT (78.9%), and the most common fibrinolytic was rtPA (73.6%, N = 14), followed by urokinase. No cases using streptokinase were reported. The most common adjunctive therapy was stenting in 11 (57.9%) cases. Inferior vena cava filter placement was performed in 4 (21.1%) cases . Mechanical thrombolysis was performed in at least 3 cases but was described without enumeration by Herrera et al 72 Maternal complications included 2 episodes of major bleeding (10.5%) and 1 (5.25%) episode of preeclampsia . Aside from elective terminations, there was 1 (5.2%) episode of fetal demise. Patency rates for patients presenting with DVT ranged from 54.5% at median 1.7-year follow-up for Bloom et al 74 to 90.9% patency at mean 1.3 years for Herrera et al. 72 There were no reports of PTS and 1 (5.25%) episode of recurrence.
Reports of Catheter-Directed Thrombolysis for Treatment of Maternal Venous Thromboembolism.
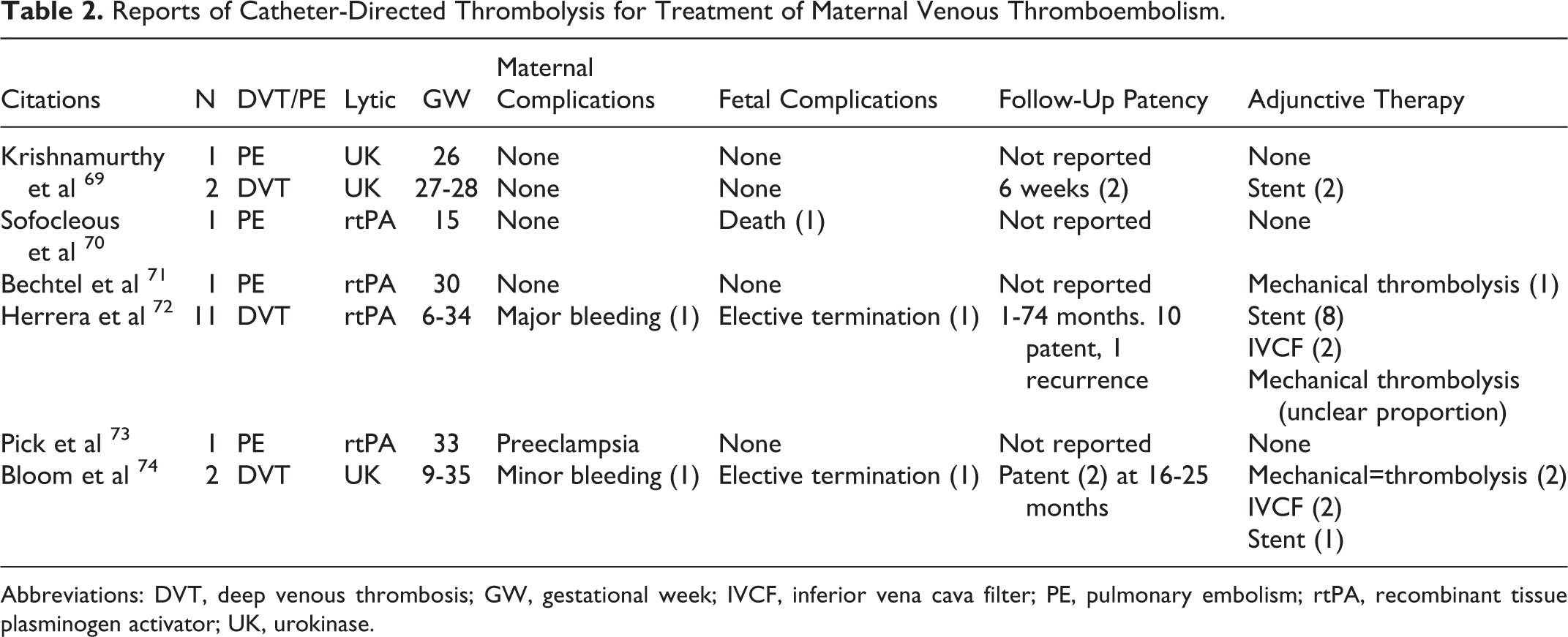
Abbreviations: DVT, deep venous thrombosis; GW, gestational week; IVCF, inferior vena cava filter; PE, pulmonary embolism; rtPA, recombinant tissue plasminogen activator; UK, urokinase.
Mechanical Thrombectomy During Pregnancy
A PubMed (National Institutes of Health) search of English language articles with all permutations of the search terms “mechanical thrombectomy,” “pregnancy,” “deep vein thrombosis,” “pulmonary embolism,” and “venous thromboembolism” yielded 3 relevant case reports with 13 patients (Table 3). Average maternal age was 29.6 years, with gestational ages ranging across all trimesters. No patients were found to have a hypercoagulable syndrome.
Reports of Mechanical Thrombectomy for Treatment of Maternal Venous Thromboembolism.
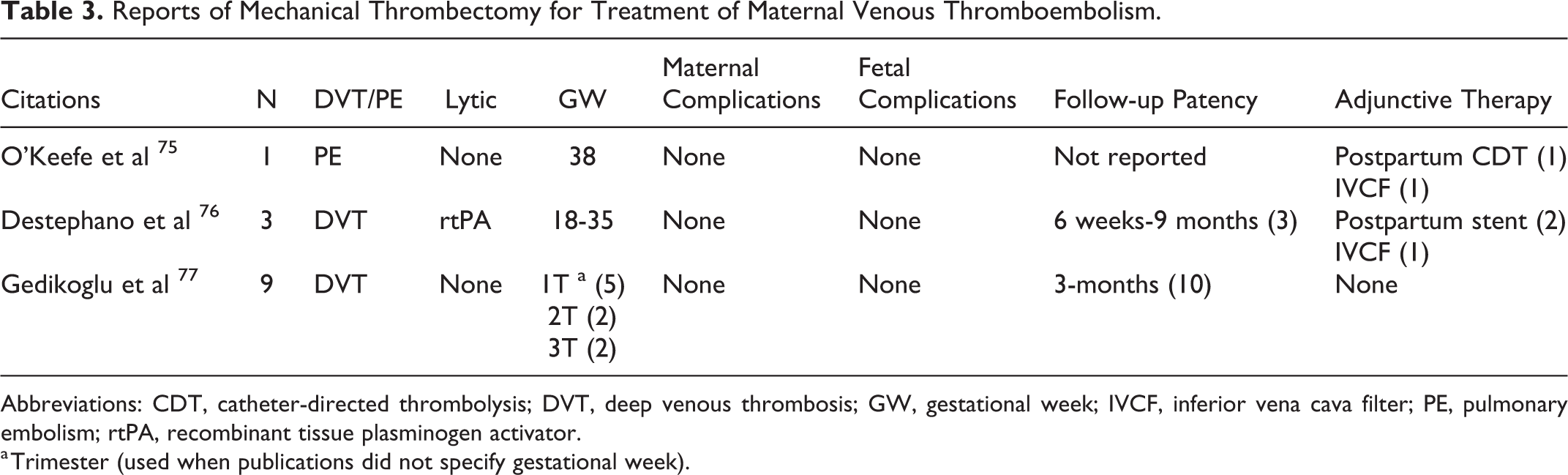
Abbreviations: CDT, catheter-directed thrombolysis; DVT, deep venous thrombosis; GW, gestational week; IVCF, inferior vena cava filter; PE, pulmonary embolism; rtPA, recombinant tissue plasminogen activator.
a Trimester (used when publications did not specify gestational week).
No maternal or fetal complications were reported. Follow-up patency ranged from 6 weeks to 9 months in 13 patients when reported. Adjunctive therapy included IVC filter placement in 2 (15.35%) patients , postpartum CDT in 1 (7.69%) patient , and postpartum stent in 2 (15.38%) patients . In patients undergoing treatment for DVT, there were no reports of PTS or reocclusion during a follow-up time ranging from 6 weeks to 3 months.
Discussion
The thrombotic complications of pregnancy pose a clinical challenge for vascular specialists who are familiar with thrombolytic techniques but may have limited exposure to pregnant patients. Our review of the literature suggests a paucity of reports of endovascular thrombolysis in pregnancy, including CDT and mechanical thrombectomy.
Across all patients with VTE undergoing systemic thrombolysis, we found a 2.75% rate of maternal major bleeding and 1.65% rate of fetal demise. Complication rates were higher in patients presenting with PE, with a 12.5% rate of maternal major bleeding and 8.33% rate of fetal demise. These findings are consistent with those in reviews conducted by Ahearn et al in 2002 and Gartman in 2013, although the latter included patients who deferred treatment until after delivery. 40 A lack of reports after 2011 also suggests that the practice has become less common, perhaps due to a preference for endovascular techniques or conservative management. The predominance of streptokinase as a fibrinolytic agent of choice is indicative of this, as intravenous alteplase was not approved for use in the United States until 1987, after the largest study found in our review. 78
In pregnant patients undergoing CDT, there was a 5.2% rate of maternal major bleeding and a 5.2% rate of fetal demise. This was slightly less than double the major maternal bleeding rate and over 3 times the rate of fetal demise in patients undergoing systemic thrombolysis. Our finding of increased major maternal bleeding in CDT is consistent with those of randomized controlled trials of nonpregnant patients. However, these percentages reflected only one instance of major bleeding and fetal demise in a small patient cohort. Analogously, while no maternal or fetal complications were reported during mechanical thrombectomy, conclusions are limited by a small sample size.
Follow-up data in patients undergoing thrombolysis for deep vein thrombosis are lacking, making it difficult to adjudicate rates of recurrence or PTS in pregnant patients. Most reports declined to state follow-up times, and only 1 report followed patients up to 2 years. Since PTS is a long-term, insidious complication, afflicting 23% to 60% of patients with DVT 2 years after their initial presentation, 79 the prevalence of PTS in pregnant patients treated for DVT cannot be ascertained without extensive follow-up.
The effects of fetal ionizing radiation are dependent on the dose and timing of exposure. Calculated dose equivalent exposure over 0.5 Gy has been associated with pediatric leukemia, 80 while exposure over 0.05 Gy has been associated with spontaneous abortion, growth restriction, and mental retardation. 81 The fetus is particularly susceptible from 2 to 15 gestational weeks of age, during which organogenesis and early development occurs. 81 Ultimately, given the retrospective nature of these studies and efforts to limit radiation in pregnancy overall, detailed prescriptions for radiation exposure during pregnancy are limited. Although none of the studies reported in our review suggested any defects secondary to radiation, many of the associated conditions are subtle and impossible to diagnose without extended follow-up.
As such, we recommend vigorous efforts to reduce radiation time for any endovascular procedure during pregnancy. In addition to standard techniques to reduce radiation during endovascular surgery, such as the use of collimators and reduction in fluoroscopy time, draping the patient’s pelvis with a lead apron can provide additional coverage. 82
In all, our review identified 183 cases of systemic thrombolysis, 19 cases of CDT, and 13 cases of mechanical thrombectomy in pregnancy for VTE. The immediate maternal major bleeding rate ranged from 0% to 5.2% in all procedures. Fetal complications ranged from 0% to 5.2%. Ultimately, more reports with longer term follow-up are necessary to reach reliable conclusions on the durability and efficacy of thrombolytic interventions for this at-risk population.
Conclusion
Reported cases of thrombolysis during pregnancy for VTE have demonstrated low rates of maternal and fetal complications for systemic thrombolysis and mechanical thrombectomy, with higher rates of maternal and fetal complications in CDT. Comparisons of outcomes are limited by small sample sizes and lack of follow-up data for each treatment modality. In order to ascertain a role for CDT in pregnancy-related VTE, more longitudinal studies are needed to assess the outcomes and long-term patency of these interventions in the pregnant population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.