
Abstract
Introduction:
Although endovascular therapy is becoming an alternative to open surgical repair of splenic artery aneurysms (SAAs), reports on the use of stent grafts for SAA repair are limited. We present our experience of endovascular therapy using a stent graft for the treatment of an SAA that had ruptured into the gastric lumen. We also reviewed 18 cases of stent graft repair for SAAs, including the present case.
Case Report:
A 43-year-old man was admitted due to hematemesis. Endoscopic examination and contrast-enhanced computed tomography (CT) revealed a dissecting SAA that had ruptured into the stomach. Two 10 × 100 mm Viabahn (W.L. Gore, Flagstaff, Arizona) stent grafts were used to exclude the aneurysm. No complications occurred during the procedure. Although postoperative CT showed complete exclusion of the aneurysm, endoscopic examination showed a discharge of purulent matter from the aneurysm. Therefore, surgical debridement and omental implantation were added to avoid stent graft infection. Follow-up CT obtained 1 year later showed the residual aneurysm almost disappeared without any evidence of infection.
Literature Review:
A literature search in the PubMed database returned 17 cases with sufficient data. Review of these cases, together with the present case, revealed a 100% technical success rate, 11% splenic infarction rate, 94% graft patency rate, and 0% reintervention rate.
Conclusion:
Endovascular repair of SAAs using stent grafts appears to be safe and effective. In terms of preserving the blood flow and avoiding splenic infarction, it may be superior to coil embolization. Even in a case with aneurysm infection, stent graft repair may be an acceptable method to minimize invasion of concomitant surgical intervention.
Introduction
Aneurysmal degeneration of the visceral branches of the abdominal aorta is a rare but potentially life-threatening condition. Splenic artery aneurysms (SAAs) are the third most frequent intra-abdominal aneurysms, following abdominal aortic aneurysms and iliac artery aneurysms. 1 They account for 60% to 70% of all visceral artery aneurysms. 2,3 Stanley identified SAAs in 0.8% of 3600 patients who underwent nonselective abdominal angiograms. 4 Splenic artery aneurysms are being diagnosed more frequently than before because of the increased availability of computed tomography (CT) imaging. 5 Almost all SAAs are asymptomatic and are discovered incidentally. Rupture of SAAs is reported to occur in 2% to 10% of patients as the initial presentation, 6 but gastrointestinal bleeding caused by SAA rupture is very uncommon. We present a case of an SAA rupturing into the stomach that was successfully managed by endovascular stent grafting. We also conducted a review of the available literature on endovascular therapy for SAAs using a stent graft.
Materials and Methods
We used the PubMed database as the source for a literature review and searched for manuscripts published in English. The search terms used were “splenic artery aneurysm” and “stent graft.” The corresponding author reviewed the search results and decided which of these articles should be incorporated into this study. A written informed consent was obtained from the patient and the institutional review board of our hospital approved this report.
Case Report
A 43-year-old man was admitted to a local hospital due to hematemesis. Emergent endoscopic examination of the upper gastrointestinal system showed an approximately 5-cm submucosal mass with an ulcer at the top (Figure 1). Bleeding, seemingly from the ulcer, appeared to have stopped at that time. Contrast-enhanced CT imaging revealed a 38 × 43 × 64 mm dissecting aneurysm spanning the proximal and middle part of the splenic artery and projecting into the stomach (Figure 2). Another saccular aneurysm, measuring 28 mm in diameter, was also observed near the splenic hilum. Because of concerns about rebleeding, the patient was referred to our hospital. Both open surgical repair and endovascular intervention were discussed as therapeutic options among several departments. The proposed surgical option was aneurysmectomy together with splenectomy and distal pancreatectomy because the SAA was spanning so extensively, which was deemed to be unacceptably invasive. Therefore, endovascular therapy using a stent graft was chosen as a minimally invasive treatment option for the larger dissecting aneurysm. And, the aneurysm of the distal splenic artery was determined to be managed conservatively.
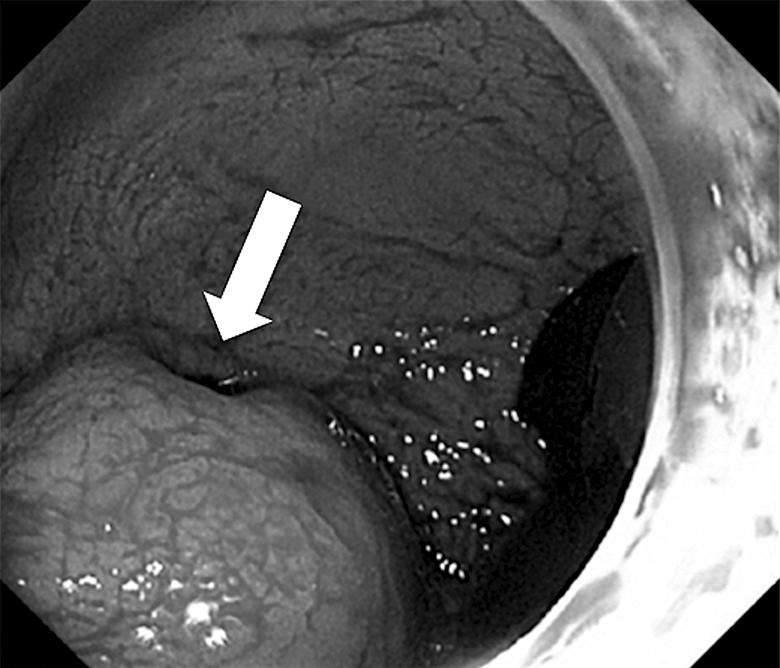
Upper gastrointestinal endoscopy shows a 5-cm submucosal mass with an ulcer (arrow) on top.
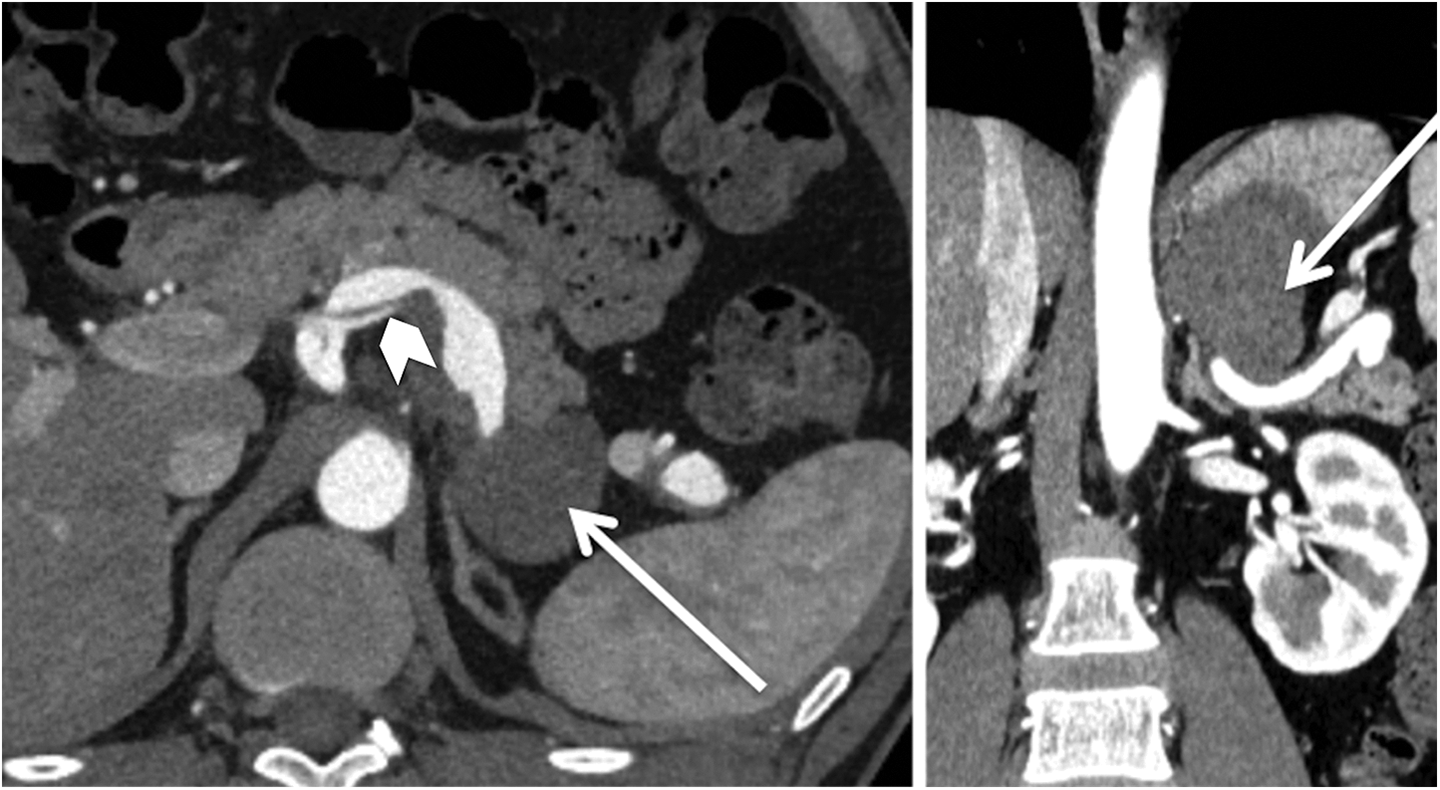
Contrast-enhanced computed tomography (CT; axial image on the left, coronal image on the right) shows a splenic artery aneurysm projecting into the stomach (arrow) and a dissected splenic artery (arrowhead).
All endovascular procedures were performed via a 12F sheath (Ansel: Cook Inc, Bloomington, Indiana) placed in the right femoral artery under local anesthesia. A celiac arteriogram detailed the 2 SAAs described earlier (Figure 3). The proximal part of the splenic artery was 8 mm in diameter measured with the use of intravascular ultrasonography (Visions PV: Philips, Amsterdam, the Netherlands). After selecting the celiac artery with a 4F diagnostic catheter, a 0.035-in hydrophilic wire (Terumo, Tokyo, Japan) was advanced into the splenic artery. This wire was exchanged for a 0.035-in stiff wire (Amplatz: Cook Inc) after advancing the tip of the 4F catheter into the splenic hilum. Then, two 10 × 100 mm self-expanding stent grafts (Viabahn: W.L. Gore and Associates, Flagstaff, Arizona) were deployed such that they spanned the distance between the origin of the splenic artery and its distal portion. Gentle dilatation was done using an 8 × 20 mm balloon catheter (Mustang: Boston Scientific, Marlborough, Massachusetts) to correct poor apposition at the proximal end. Postprocedural angiography confirmed the successful exclusion of the proximal aneurysm with free flow through the stent graft (Figure 4). After the artificial sheath was removed, the puncture site in the right common femoral artery was closed using a vascular closure device (Prostar XL: Abbot Vascular, Santa Clara, California). No complications occurred during the procedure.
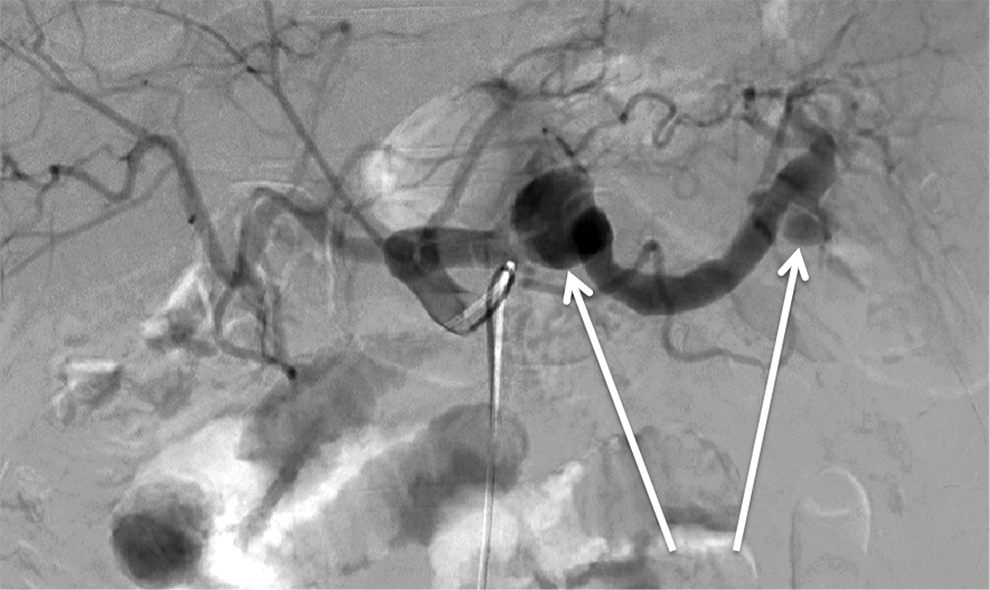
Celiac arteriogram shows 2 splenic artery aneurysms (SAAs; arrows).

Postprocedure angiography shows successful exclusion of the proximal aneurysm with free flow through the stent graft.
A contrast-enhanced CT obtained 3 days after the procedure showed that the SAA was completely excluded, but a small air bubble was visible inside the aneurysm sac (Figure 5). An upper gastrointestinal endoscopic examination showed a discharge of purulent matter from the SAA. Therefore, a drainage tube was inserted into the aneurysm sac through the gastric wall during endoscopy, and antibiotic therapy was started immediately. Although Peptoniphilus asaccharolyticus was detected in the pus, the patient was afebrile and stable. On the 19th day after the intervention, surgical debridement and omental implantation were performed to avoid stent graft infection. No complications occurred during the perioperative period. The patient was discharged on the ninth day after the open surgery. A follow-up contrast-enhanced CT performed at 6 months showed shrinkage of the residual aneurysm without any evidence of infection. And the residual aneurysm almost disappeared 1 year after the intervention. The patency of the stent graft and the perfect perfusion of the spleen without any infarcts were also confirmed. The patient is currently being followed up as an outpatient and has been prescribed oral antibiotics.
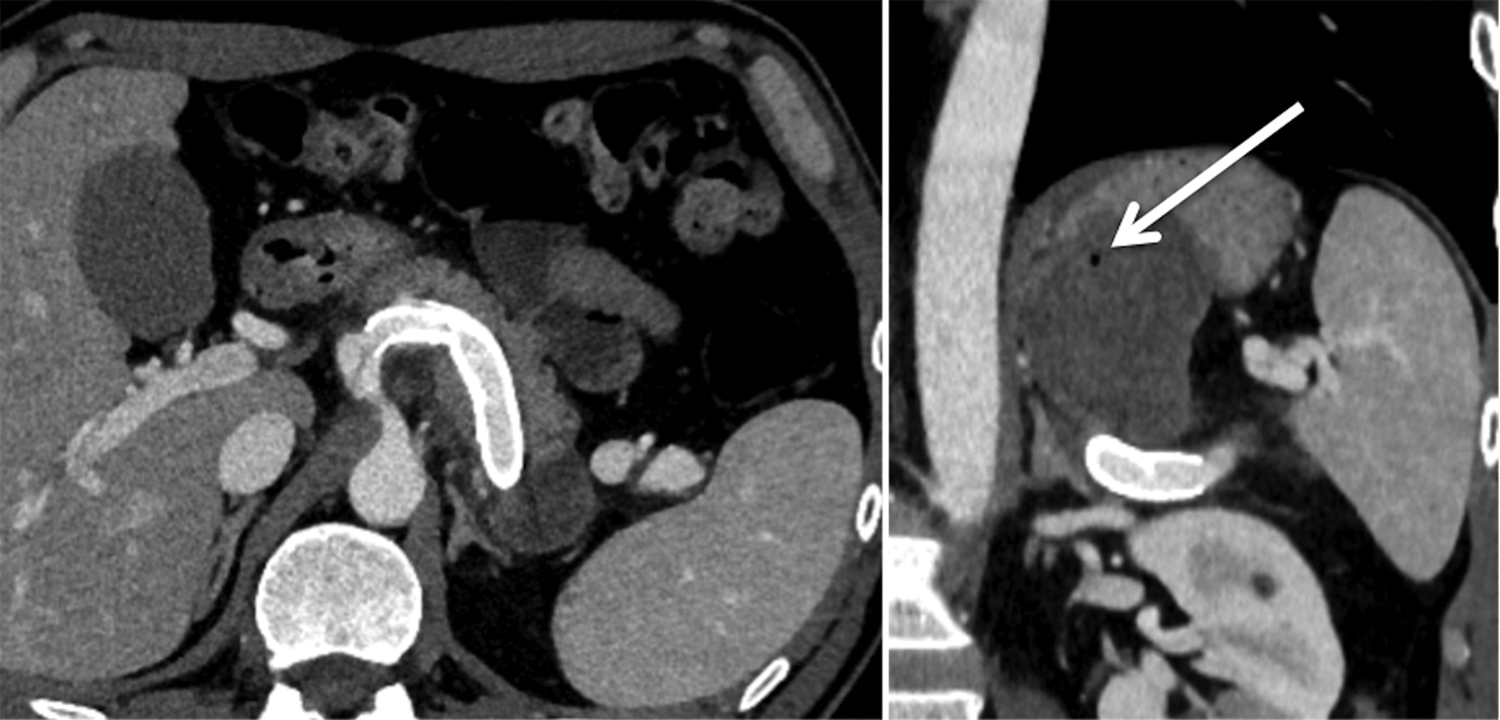
Contrast-enhanced computed tomography (CT) performed 3 days after the intervention (axial image on the left, coronal image on the right) shows a complete exclusion of the splenic artery aneurysm (SAA) and patency of the stent graft. However, a tiny air bubble can be seen in the aneurysm sac (arrow), indicating an infection.
Discussion
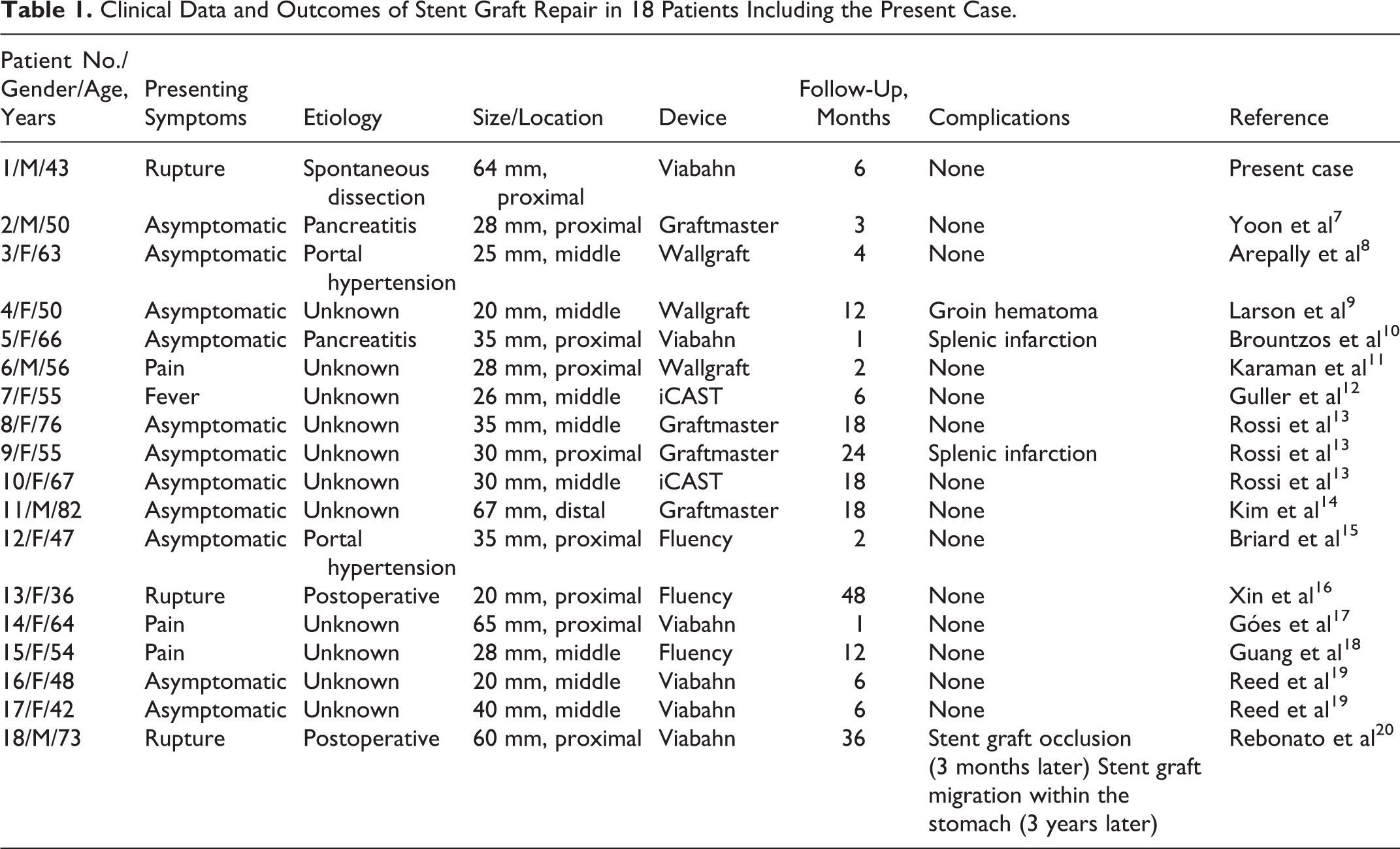
A literature search returned 27 cases of SAAs that had been treated using stent grafts. Among them, 10 cases were excluded from the present analysis because of incomplete data on age, gender, aneurysm diameter, or follow-up details. We reviewed the remaining 17 cases, for which all relevant details and follow-up data were available, along with the present case (Table 1). 7 -20 Of these 18 cases, 13 (72%) were female; the median age was 55 years (interquartile range [IQR]: 47.8-66.3 years). The median aneurysm diameter was 30 mm (IQR: 25.8-45.0 mm) in all cases and 30 mm (IQR: 26.0-35.0 mm) in nonruptured cases. The aneurysm was located in the proximal third of the splenic artery in 9 (50%) cases, in the middle third in 8 (44%), and in the distal third in 1 (6%). The etiology was unknown in 11 cases and was ascribed to pancreatitis in 2, portal hypertension in 2, postoperative pseudoaneurysm in 2, and spontaneous dissection in 1. Although 11 cases were asymptomatic, 3 had ruptured, 3 had abdominal pain, and 1 had fever. The stent grafts used include the Viabahn (n = 6), Graftmaster (n = 4; Abbott Vascular, Santa Clara, California), Fluency (n = 3; BARD Peripheral Vascular, Inc, Tempe, Arizona), Wallgraft (n = 3; Boston Scientific), and iCAST (n = 2; Atrium, Hudson, New Hampshire). Technical success was achieved in all cases. There were no procedure-related deaths or major complications, but splenic infarction was reported in 2 (11%) cases. 10,13 The median follow-up period was 6 months (IQR: 2.8-18.0 months). Complete exclusion of the aneurysm was confirmed in all cases, no significant increase in aneurysm diameter was noted, and no patient required reintervention. One instance of stent graft thrombosis occurred 3 months after the placement of a Viabahn stent graft. 20 However, the patient was stable, and the spleen remained perfused by collaterals, but the stent graft had migrated into the stomach 3 years after the intervention. The patient was palliatively managed because of the presence of a progressive malignant tumor.
Clinical Data and Outcomes of Stent Graft Repair in 18 Patients Including the Present Case.
The etiology was unknown in most cases reviewed here (61%), and it is reasonable to presume atherosclerosis as the main cause. Taking into consideration that dissection can be easily diagnosed by various imaging modalities, spontaneous dissection such as that observed in our case should be a relatively rare etiology. In the case described here, the splenic artery was so badly damaged by the dissection that it had lost the intimal flap in the middle part of the splenic artery, which may have led to the development of a large SAA that protruded and ruptured into the stomach.
Previous reports state that nearly 10% of patients with SAA presented with an acute rupture, which manifests as a sudden onset of sharp abdominal pain in the left upper quadrant and hypotension. 21 However, a recent study reports that this frequency has decreased to approximately 3% because of the widespread availability of modern imaging systems. 21 Splenic artery aneurysms can rupture not only into the surrounding space but also into adjacent organs such as into the digestive tract, 22 as in our case, and into the pancreatic duct. 23 Ruptured SAAs were observed in 3 (17%) of the 18 patients reviewed, and this high prevalence of rupture may be related to the urgent need to immediately treat the aneurysm using a stent graft.
Ruptured SAAs should be treated as a matter of urgency. However, the indication for intervention to asymptomatic SAAs has not been determined yet because the natural course of this disease is not well known. It is generally accepted that incidental asymptomatic aneurysms detected during or before planned pregnancy and asymptomatic aneurysms >20 mm should be treated. 21 The median aneurysm diameter of nonruptured cases was 30 mm in the present review series. Therefore, it is speculated that treatment is being carried out on the similar criteria regarding the size in many institutions.
Treatment options for SAAs include open surgery, coil embolization, and stent graft implantation. Although conventional open surgery was the mainstay of therapy until the last decade, its invasiveness is sometimes enormous because it may require resection of the spleen, pancreas, or other neighboring organs. 24 Thus, endovascular therapy is gaining favor because it is less invasive. Coil embolization is currently the first treatment option for SAAs. In the case of a giant aneurysm, its isolation by embolization of the afferent and the efferent splenic artery is considered to be the best option. However, splenic infarction occurs in up to 40% of the patients treated with this technique. 25,26 Large painful infarcts may necessitate prolonged hospitalization for pain control. In addition, splenectomy or percutaneous drainage may be required for the treatment of abscesses or refractory pain. Stent graft implantation can preserve splenic artery flow and minimize the potential risk of splenic infarction. Of the cases reviewed here, there were only 2 (11%) cases of splenic infarction.
Another concern with coil embolization for a ruptured SAA is recanalization that may lead to rebleeding, and this has been reported to develop in up to 12% of all cases. 19,26,27 When the procedure ends up in embolization of the afferent artery alone due to tortuosity of the splenic artery, rebleeding can still occur due to collateral vessel flow. 28 Rebleeding may also develop even if a stent graft is used instead of coil embolization because the risk of potential leaks remain even with this device. However, it is important to note that there have been no such reports, at least in the present review series.
As with coil embolization, difficulties may be encountered on delivering a stent graft through the tortuous splenic artery due to the relatively large-bore delivery system and its stiffness. Indeed, we were forced to use a stiff wire to deliver the stent grafts in the present case as with most previous cases. In addition to the difficulties in delivery, endovascular repair using a stent graft has several other drawbacks compared to coil embolization. First, it requires both proximal and distal necks with sufficient length to obtain good sealing. Therefore, cases such as the SAAs are located in the distal part of the splenic arteries are often not amenable to stent graft repair. In support of this assumption, we found only one case of an SAA at the distal splenic artery being repaired by stent grafting in the present series. Second, if the SAA is a true aneurysm and has vessels branching from it, a low pressure leak that is similar to type II endoleak of stent grafting for aortic aneurysm may develop. Therefore, close preprocedural evaluation of the aneurysm is mandatory to avoid this complication. When vessels branching from the aneurysm are confirmed, embolization of these vessels may also be required before the placement of a stent graft.
The important point in our case is that the infection was suspected. Some claim that stent graft repair cannot be an effective treatment in such a situation. However, large series reported by Sörelius et al concluded that endovascular treatment of mycotic aneurysm was a durable treatment option. 29 Furthermore, favorable results with combination therapy of endovascular stent graft treatment and abscess drainage are reported recently. 30 In our case, stent graft repair combined with drainage and surgical debridement contributed to the preservation of both spleen and pancreas without deterioration in infection. No signs of infection were confirmed at 1 year follow-up.
Strengths and Limitations
There are few reports of combination with stent graft implantation and surgical debridement for SAA ruptured into digestive tract. This report showed the feasibility of endovascular treatment of infected visceral artery aneurysm. This review of literature has certain limitations. First, there may be cases that were not included because they were not available in the PubMed database or did not return as a result when searched using the key words “splenic artery aneurysm” and “stent graft.” In addition, several reports were excluded from the present series because they lacked some essential case information. It is, therefore, possible that the outcomes reported here might be different from that experienced in clinical practice. Second, the characteristics of the SAAs and the procedural details, including stent grafts used, were so diverse that it may be difficult to derive any definitive conclusions.
Conclusions
A review of previously reported cases, together with that of the present case, indicated preferable outcomes for stent graft repair in the treatment of SAAs. Compared to coil embolization, endovascular therapy using a stent graft has the advantage of preserving blood flow to the spleen and avoiding ischemia. Even in cases with infected aneurysms, it may contribute to minimizing overall invasiveness.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.