
Abstract

A 67-year-old gentleman with end-stage renal failure on hemodialysis using right arteriovenous fistula presented with recurrent symptomatic thoracic central vein obstruction (TCVO). He initially presented 3 years ago with total occlusion of the superior vena cava (SVC; Figure 1), which was recanalized using balloon angioplasty and a 16 × 60 mm open-cell venous stent (Zilver Vena; Cook Medical, Bloomington, Indiana) was implanted. His symptoms recurred 2 years later, and repeat angiography showed distal stent deformation and in-stent restenosis. A second 16 × 60 mm self-expanding, closed cell venous stents (Vici; Boston Scientific, Marlborough, Massachusetts) were deployed overlapping with the previous stent extending with distal-end landing distal to the right subclavian (SCV) and internal jugular vein junction.
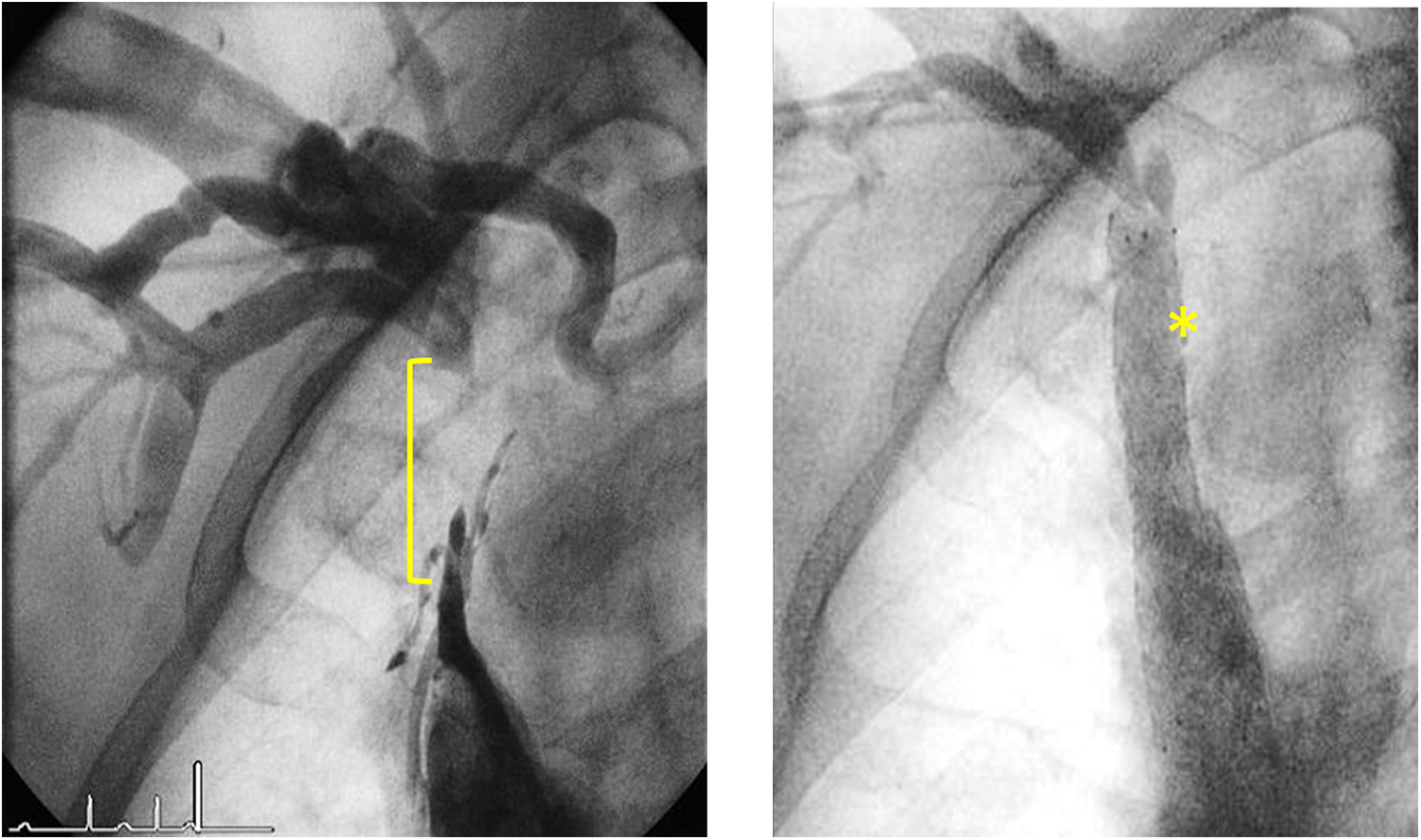
Initial venogram 3 years ago showed total occlusion of superior vena cava (yellow bracket). It was recanalized with balloon angioplasty and a 16 × 60 mm Zilver Vena stent was deployed. Symptoms recurred 2 years later and a second Vici stent (yellow asterisk) were deployed overlapping with the previous Zilver Vena stent.
One year after the second venoplasty, he presented again for recurrent TCVO symptoms. Repeat venography showed distal stent occlusion of the second stent (Figure 2). The occlusion was crossed, and positions of wires were secured in both the SCV and a large subclavian collateral vein (SCoV). Both SCV and SCoV were dilated with 8 mm noncompliant balloons but with suboptimal result. Bailout stenting was performed using a 7 × 40 mm interwoven self-expanding stent (Supera; Abbott Vascular, Illinois, USA) deployed at the SCV and a second 7 × 60 mm Supera stent deployed at the SCoV (Figure 3). Both Supera stents landed into the distal end of the Vici stent in a double-chimney fashion. Final venography showed brisk venous flow into SVC from both SCV and SCoV (Figure 4). The patient’s symptoms resolved after the venoplasty, and he remained asymptomatic up to 12 months follow-up.

Venography during this presentation showed distal stent edge total occlusion (yellow arrow).
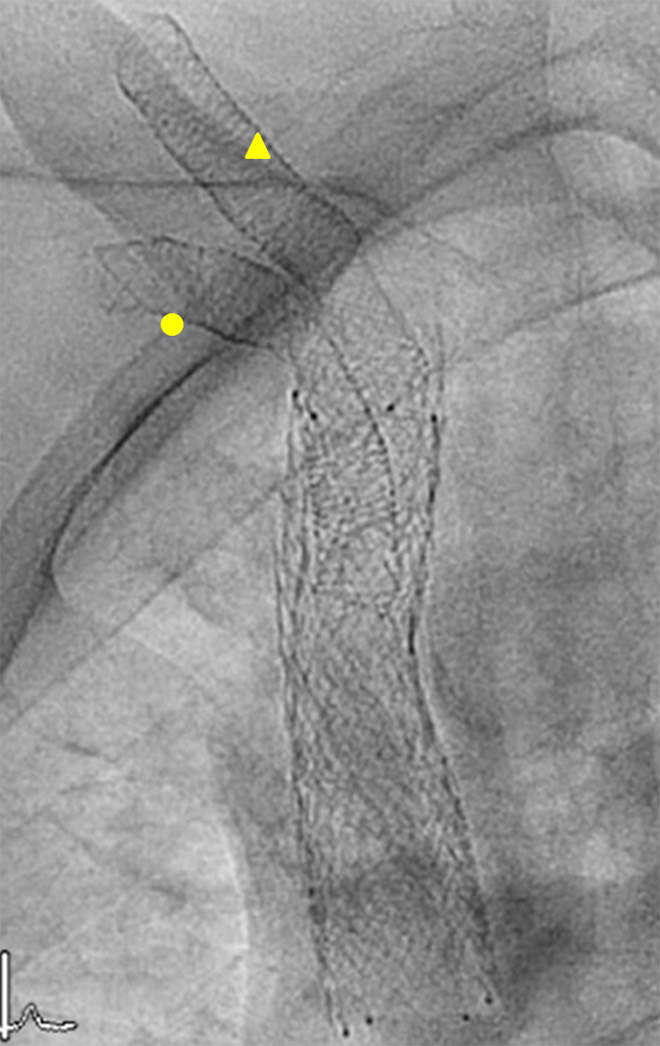
Double chimney style stenting was performed with a 7 × 40 mm Supera stent (yellow circle) deployed from the right SCV through the Vici strut into the SVC. A second 7 × 60 mm Supera stent was implanted from SVC into the SCoV (yellow triangle). SCV indicates subclavian vein; SCoV, large subclavian artery; SVC, superior vena cava.
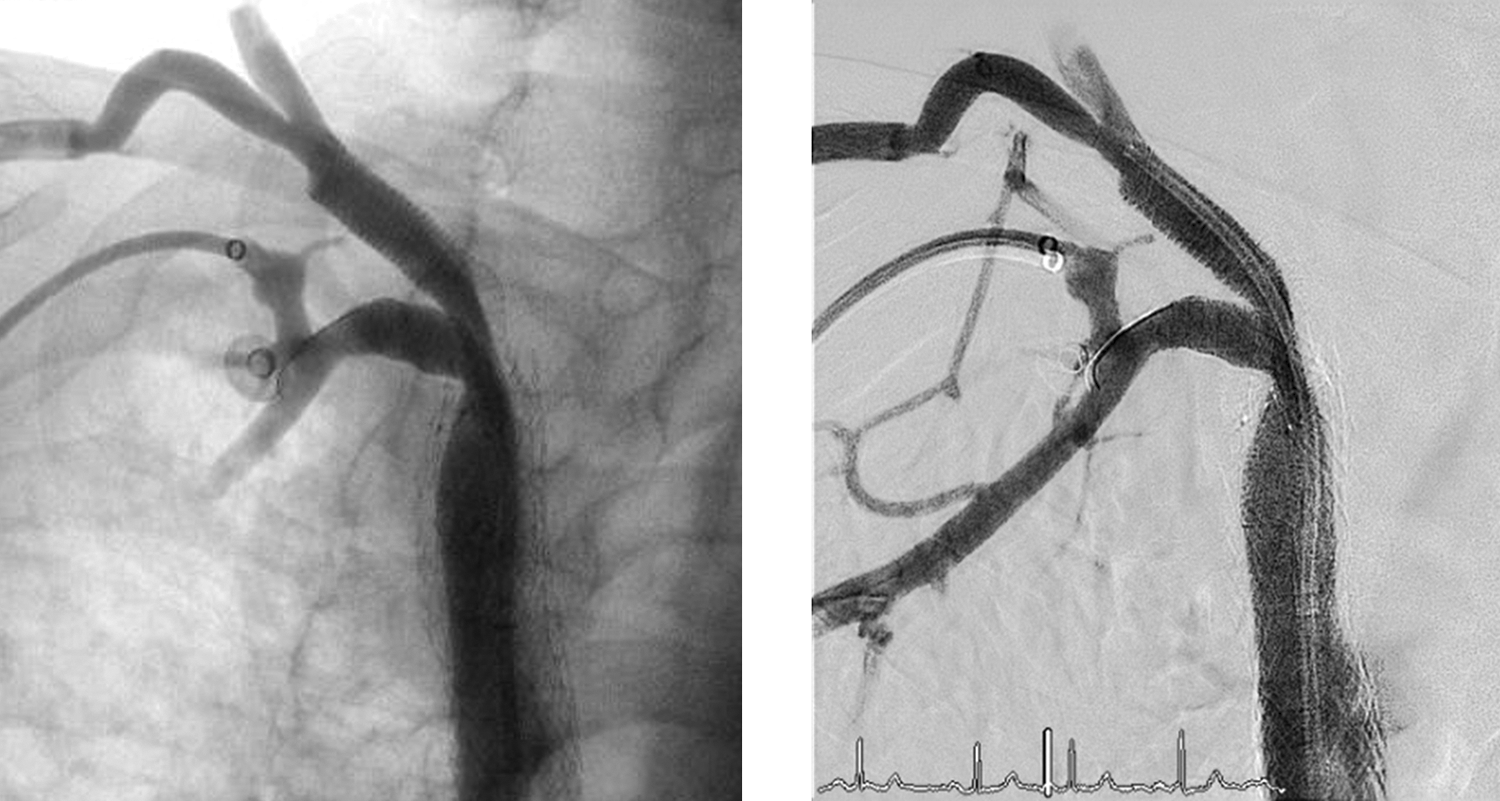
Final venogram showed brisk venous flow into SVC from both SCV and SCoV. SCV indicates subclavian vein; SCoV, large subclavian artery; SVC, superior vena cava.
Almost 50% of hemodialysis patients develop stenosis and occlusion of the thoracic central veins as a result of inflammation and fibrosis from previous central venous catheter placement. 1 Endovascular intervention with balloon angioplasty with or without stenting has been shown to be a viable treatment option for symptomatic TCVO but is limited by high rates of restenosis. 2,3 This case demonstrates the off-label use of interwoven stents in the treatment of complex TCVO restenosis. The properties of high radial strength and kink resistance of the interwoven stent make it ideal for implantation in a tortuous venous anatomy and across joints. However, the utility of the interwoven stent in venoplasty is mainly limited by the lack of a comprehensive range of size and the difficulty in stent deployment. It is unusual to deploy stent across a collateral vein. However, the SCoV in our case had a comparable size as the SCV, and we felt that maintaining its patency would provide a better relief for the patient’s symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.