
Abstract
We report a simple endovascular repair for symptomatic aberrant right subclavian artery (ARSA) in an 11-year-old girl. She had undergone tracheostomy due to hypoxic encephalopathy after cardiac surgery and suffered from dyspnea. Computed tomography revealed tracheal stenosis caused by a vascular ring made with an ARSA and the right common carotid artery. Transcatheter ARSA embolization using an Amplatzer vascular plug and coils was performed. Symptoms improved within a few days after this intervention and no complications such as upper extremity ischemia were encountered. Computed tomography showed the ARSA around the trachea had reduced in size and tracheal stenosis was improved.
Introduction
An aberrant right subclavian artery (ARSA) is a major arch vessel abnormality with a reported frequency of 0.16% to 0.44%. 1 Aberrant right subclavian artery is usually asymptomatic but rarely causes upper tracheal stenosis and compression of the esophagus. 2 We report a rare symptomatic case with tracheostomy treated by simple endovascular repair rather than an open surgical procedure. The patient and her family consented to publication.
Case
The patient was an 11-year-old girl diagnosed with pulmonary atresia, ventricular septal defect, major aortopulmonary collateral arteries, and an ARSA. She had undergone palliative right ventricular outlet tract reconstruction at 9 years old, and hypoxic encephalopathy developed postoperatively. Tracheotomy was performed 1 month after that surgery, and respiratory care by mechanical ventilation had been continued. The patient was given enteral nutrition from gastrostomy. Two years after the tracheotomy, she developed dyspnea, and stridor was heard. Because of frequent severe reductions in tidal volume, she needed manual, forced ventilation each time to restore respiratory status. Flexible bronchoscopy revealed stenosis of the midportion of the trachea, due to posterior compression by a discrete and pulsatile projecting shelf. Computed tomography showed compression and narrowing of the trachea by a vascular ring comprising the ARSA and the right common carotid artery (Figure 1). The tip of the tracheal tube touched the ARSA, and a risk of future progression to ARSA-tracheal fistula was considered present.
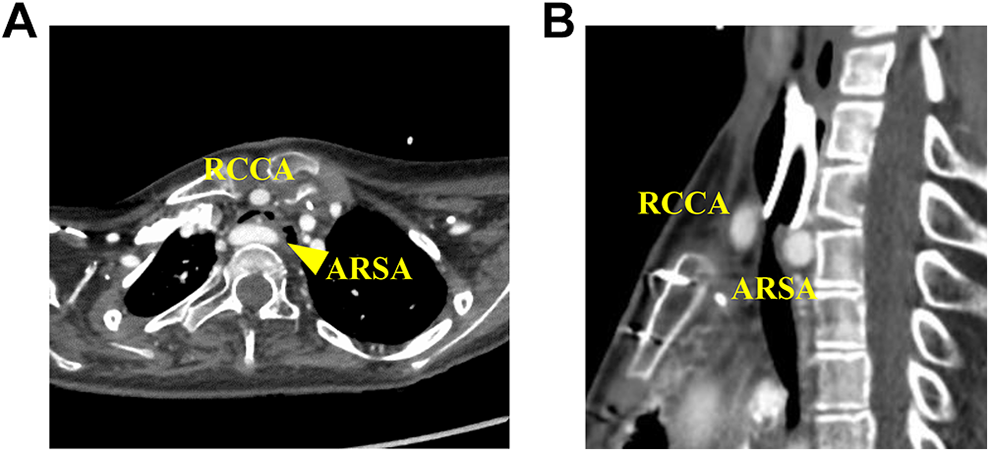
Computed tomography before endovascular repair. The trachea is compressed and narrowed by the aberrant right subclavian artery (ARSA) and right common carotid artery (RCCA). The tip of the tracheal tube touches the prominent ARSA. A, Axial view. B, Sagittal view.
To treat the tracheal stenosis and prevent ARSA-tracheal fistula, we decided to perform catheter intervention instead of open surgery because the patient was debilitated and had a history of several median sternotomies and thoracotomies, and a surgical approach was thus expected to be difficult due to severe adhesions.
A 6F guiding sheath was inserted through the right common femoral artery to the ARSA. A 10-mm Amplatzer vascular plug (St Jude Medical, Minneapolis, Minnesota) was deployed in the ARSA just proximal to the right internal thoracic artery (RITA). Before deploying another Amplatzer at the level of the ARSA orifice, branching arteries from the ARSA were occluded using coils; otherwise, the ARSA would not be thrombosed reliably due to the retrograde blood flow of the branches, and the Amplatzer deployed at the orifice of the ARSA would migrate distally due to the aortic blood pressure. We also occluded the right vertebral artery because computed tomography revealed left vertebral artery was dominant, and there was posterior communicating artery as usual. Finally, a 16-mm Amplatzer vascular plug was deployed just distal to the orifice of the ARSA. Aortography showed that the Amplatzer vascular plug had not migrated at all and the ARSA was successfully occluded. The artery distal to the plug was perfused via retrograde flow from RITA. The whole schema for this endovascular repair is shown in Figure 2.
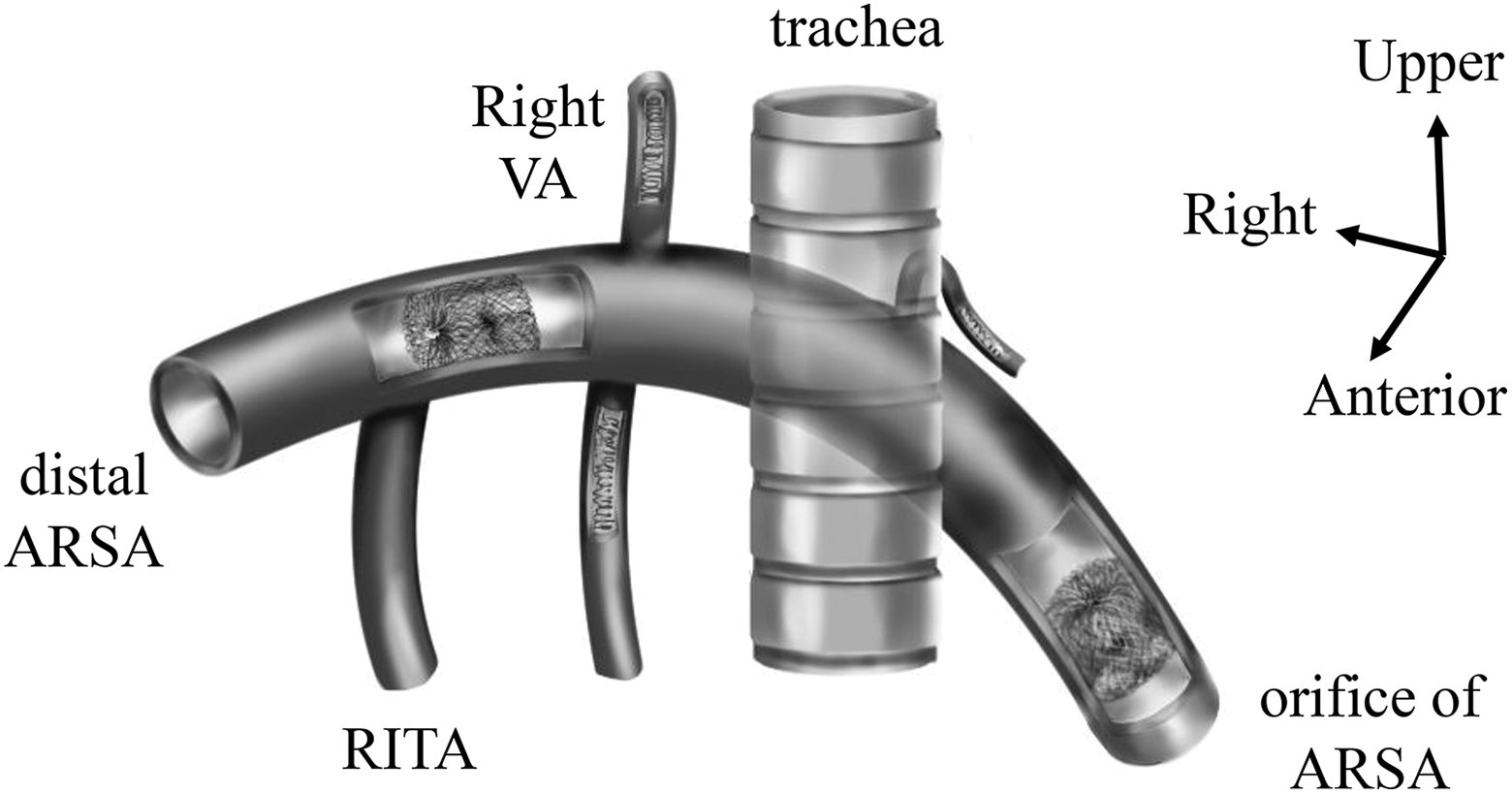
Schema for this procedure. Two Amplatzer vascular plugs are deployed, distal and proximal to the trachea. Before deploying the proximal Amplatzer, branching arteries are occluded by coils to prevent migration of proximal Amplatzer. ARSA indicates aberrant right subclavian artery; RITA, right internal thoracic artery; VA, vertebral artery.
Symptoms of tracheal stenosis gradually improved, and respiratory status became stable without manual ventilation within a few weeks. Computed tomography showed that tracheal stenosis had improved due to a reduction in size of the ARSA (Figure 3), and the tip of the tracheal tube was no longer touching the ARSA. Six months after this intervention, the patient was successfully taken off daytime ventilation.
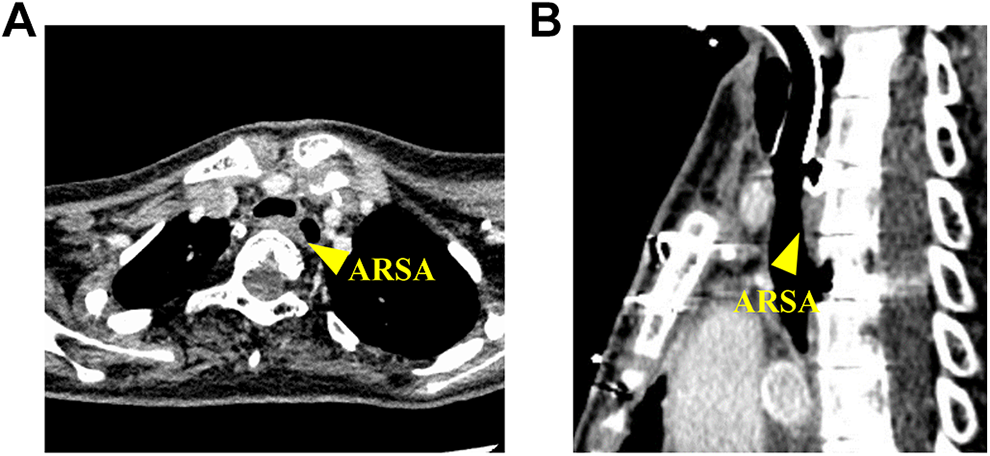
Computed tomography after endovascular repair. The aberrant right subclavian artery (ARSA) has reduced in size and tracheal stenosis has improved. A, Axial view. B, Sagittal view.
Discussion
This transcatheter ARSA embolization method was effective in 2 different ways: improvement of tracheal stenosis and prevention of ARSA-tracheal fistula. Aberrant right subclavian artery is usually asymptomatic but can cause symptoms of the trachea or esophagus is compressed between the ARSA posteriorly and truncus bicaroticus anteriorly. 2,3 Cases of tracheal stenosis with dyspnea due to ARSA as in the present case are very rare. In this patient, thoracic deformity prompted the symptom, although there were no obvious causes of tracheal compression such as Kommerell diverticulum. In addition, enteral nutrition was given from gastrostomy that was because the ARSA caused dyspnea without dysphasia, which was atypical symptom for patients with vascular ring. For symptomatic cases, surgical intervention of some kind is warranted because of the high frequency of complications associated with conservative treatment. On the other hand, tracheal-arterial fistula is known as a long-term complication of tracheotomy. 4 The mechanism involves inflammation of trachea caused by long-term stimulation from the tracheal tube cuff and tip, with the inflammation extending anteriorly to the brachiocephalic artery and then forming a fistula. In this case, the ARSA-tracheal fistula might have developed if treatment had not been provided because the tip of the tracheal tube was in direct contact with the ARSA.
The basic surgical procedure for symptomatic ARSA is ligation of the ARSA and restoration of blood flow to the right arm by anastomosing the ARSA to either the right common carotid artery or another vessel with or without interposition graft. Several operative approaches have been described, including right and left thoracotomies. Less invasive hybrid procedures such as ARSA embolization with carotid-to-subclavian artery bypass have also been reported. 5 Anastomosing the ARSA to another artery can prevent right arm ischemia and subclavian steal syndrome. In this case, we performed simple catheter embolization using Amplatzer vascular plugs without specific restoration of blood flow to the right arm. The ARSA does not make a true vascular ring around the trachea, but compression by the ARSA causes tracheal stenosis, so embolization of the ARSA is sufficient to improve tracheal stenosis. Although the risk of right arm ischemia was considered, the activity level of our patient was relatively low because of hypoxic encephalopathy, and no complications were seen after embolization. If patients complain arm pain, additional procedures such as ARSA-right common carotid artery bypass through a transverse cervical approach can be done in standard manner. 6 In the case of hypoplastic posterior communicating artery, right vertebral artery should not be occluded. In such a situation, deploying Amplatzer in the proximal part of the vertebral artery is one option, whereas we adopted presented method to reduce the volume of ARSA behind trachea as much as possible to improve tracheal stenosis.
The concept of this treatment has also been reported in other fields, such as endovascular repair for duodenal obstruction by the superior mesenteric artery and abdominal aortic aneurysm (AAA). 7 According to that report, symptoms improved relatively quickly after endovascular repair for the AAA. Reducing not only the size but also the pressure from the aorta allowed symptoms to resolve rapidly. Symptoms in our case likewise improved soon after the intervention, probably due to the same mechanisms.
We successfully improved tracheal stenosis caused by ARSA using a simple, minimally invasive transcatheter ARSA embolization method, achieving a symptom-free state for the patient. This method can also be expected to prevent tracheal-arterial fistula in patients with long-term tracheostomy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.