
Abstract
A 57-year-old male presented with intermittent gastrointestinal bleeding (GIB) 1 year after a successful simultaneous pancreas and kidney transplant. No source could be found after 5 tagged red blood cell studies, 3 computed tomographies (CTs), 7 endoscopies, and 4 catheter angiograms. Review of CTs showed pathologically enlarged superior mesenteric vein branches near a jejunal segment near pancreas graft. Transhepatic superior mesenteric venogram showed varicosities near jejunum, which were obliterated with ethylene vinyl alcohol (Onyx). Follow-up CTs confirmed complete obliteration, but he had more GIBs and eventually underwent native jejunal and donor duodenal resection. He has remained GIB-free for 12 months.
Introduction
Ectopic varices, defined as varices arising from locations other than esophagus or stomach, account for 1% to 5% of variceal bleeding. 1 Jejunal varices account for approximately 6% of ectopic varices 2 and are primarily associated with portal hypertension 3 or rare situations such as pancreaticobiliary surgery. Bleeding after pancreas transplant from arterial complications 4,5 has been reported, but we present recurrent gastrointestinal bleeding (GIB) from intestinal ectopic varices.
Case Report
Individual case reports are exempt from review by institutional review board. Informed consent has been obtained from the patient for publication of the case report and accompanying images. A 57-year-old African male with end-stage renal disease and coronary artery disease underwent simultaneous kidney and pancreas transplant. Pancreas transplant was performed to the right iliac vessels with systemic venous drainage and enteric exocrine drainage. Posttransplant course was only remarkable for a peripancreatic abscess due to extended spectrum β-lactamase Escherichia coli which resolved with percutaneous drainage and antibiotics. At 1 year posttransplant, he presented with intermittent GIB with hemodynamic instability and hemoglobin drops requiring multiple blood transfusions. His liver function tests were all within normal limits.
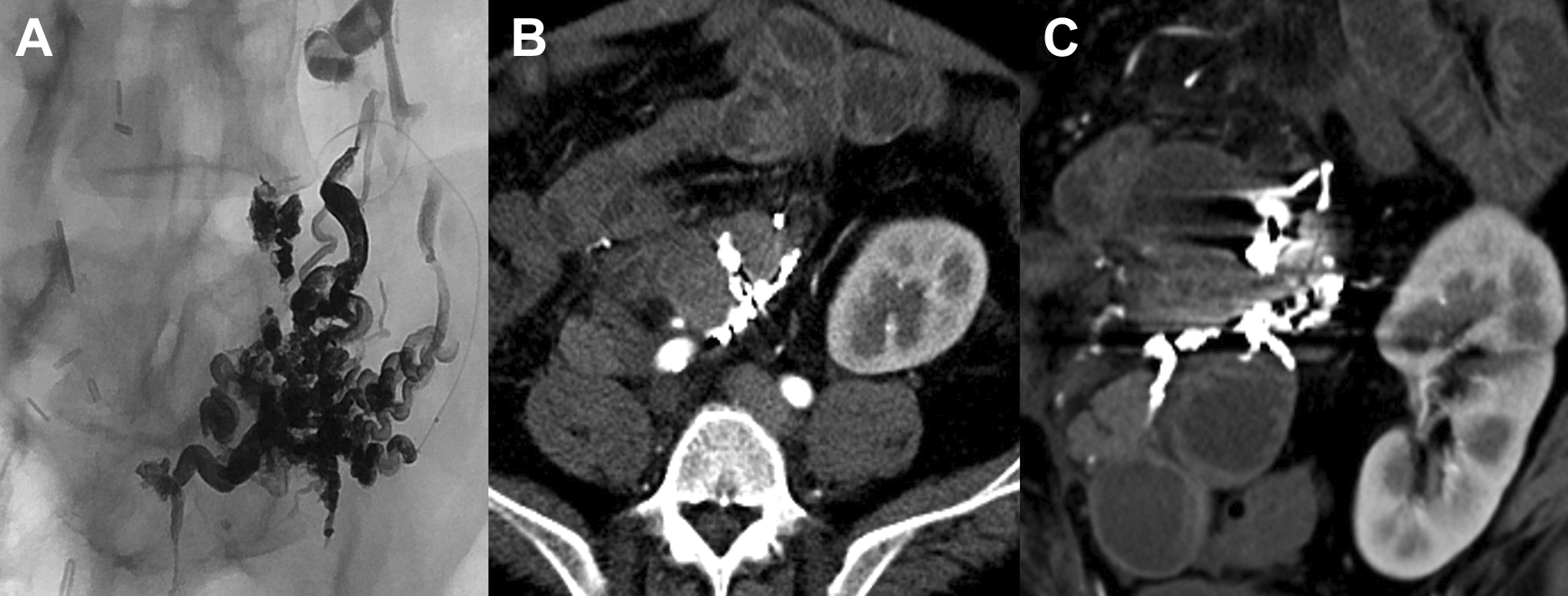
He had 5 admissions at 12, 14, 16, 17, and 18 months posttransplant. Duplex ultrasound of the pancreas allograft did not reveal any abnormalities in the vasculature of the graft. Five tagged RBC nuclear medicine scans were performed, 2 of them were positive for GIB from unclear location in the small bowel. Seven upper and lower endoscopies were performed, including push enteroscopies and double balloon endoscopies, which were unable to show the source of GIB. Push endoscopy was difficult for visualization of duodenal cuff of pancreas transplant since it was not reachable with a single balloon. A capsule endoscopy identified an area of erythematous jejunal mucosa and an arteriovenous malformation was suggested (Figure 1). Four catheter angiograms in the superior mesenteric artery territory and pancreas allograft Y-graft were all normal. In 2 of these catheter angiograms, provocative measures (300 µg nitroglycerin, up to 4 mg tissue plasminogen activator intra-arterially, 500 units of heparin intravenously) and cone beam CT were also used. Prolonged digital angiography runs only showed some engorged veins in the superior mesenteric vein (SMV) distribution (Figure 2C). Three CT angiograms were performed with no active extravasation. But review of all consecutive CT angiograms showed a segment of jejunum which was persistently hyperemic with adjacent engorged veins (Figure 2A-B) in SMV distribution with no portal thrombosis or abnormal mass effects on the portal vein. Liver morphology was normal.
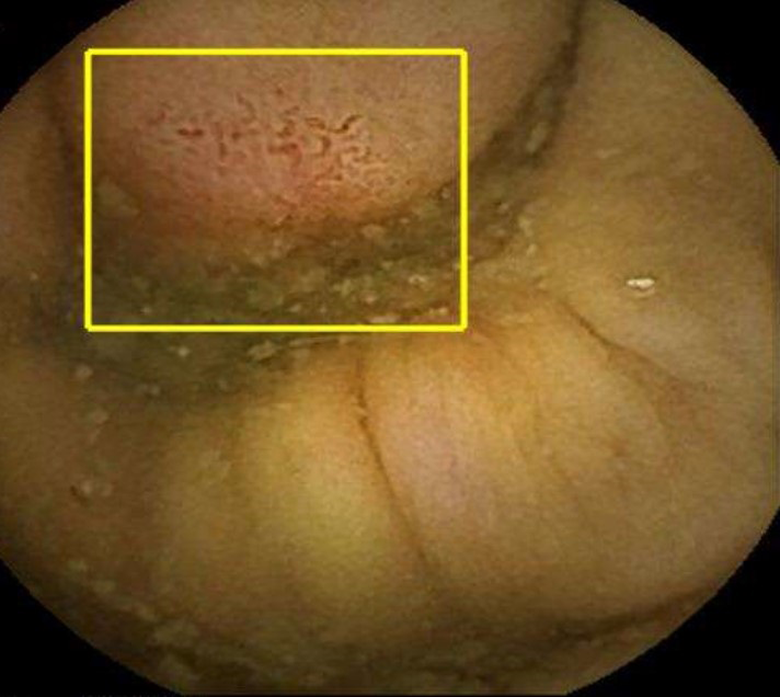
Capsule endoscopy demonstrated nonspecific engorged vessels in the wall of jejunum which were deacribed as possible arteriovenous malformation. This was only seen on capsule endoscopy and colonoscopy and upper gastrointestinal endoscopies did not show any abnormal findings.
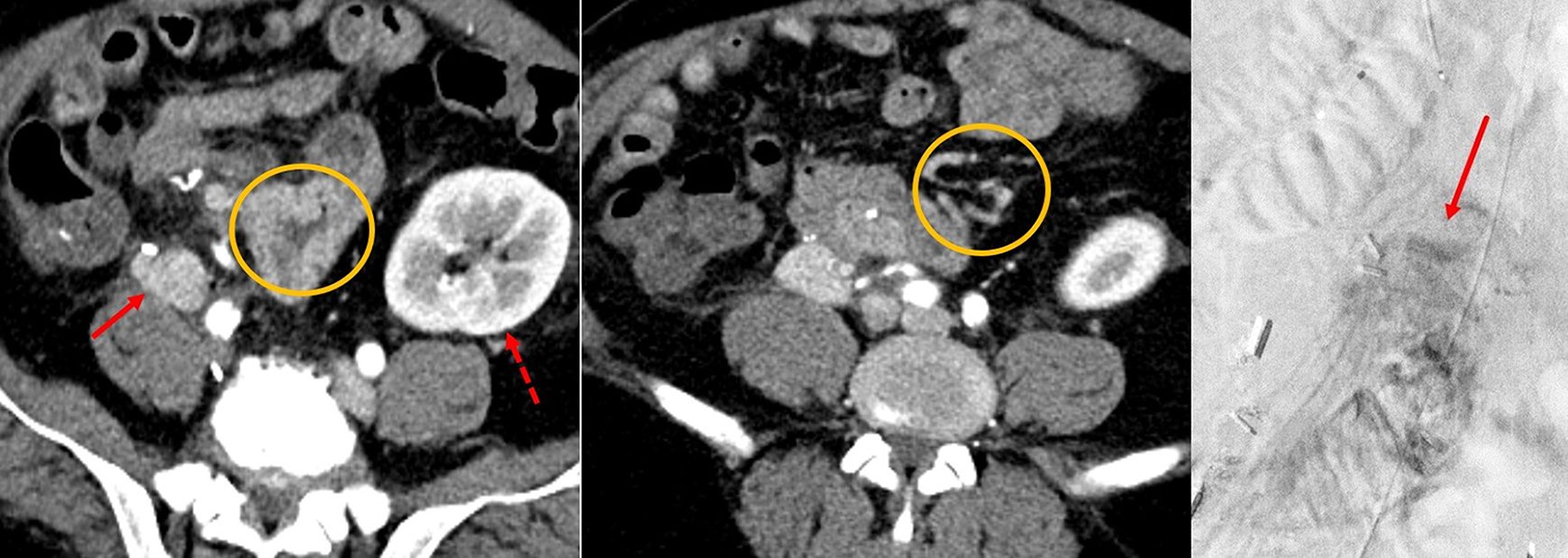
A, Computed tomography scan with contrast showing a hyperemic native jejunal segment (circle) adjacent to the pancreas graft (arrow). Dashed arrow shows kidney transplant. B, At 15 months posttransplant, the veins in the superior mesenteric vein (SMV) distribution are prominent and engorged. C, A prolonged SMA angiogram vaguely shows an engorged vein in the SMV distribution (arrow).
Procedural Details
The SMV venogram via percutaneous transhepatic portal access was performed which showed a large vascular network in peripheral SMV distribution. On prolonged venograms, the iliac vein outflow of the pancreas graft and eventually the inferior vena cava were visualized (Figure 3). Transjugular access to the pancreas graft’s portal vein anastomosis with native iliac vein confirmed communication and a pattern like portosystemic veno-venous fistula creating a network of ectopic varicose veins. Balloon occlusion catheters (5F Python catheter; Applied Medical, Rancho Santa Margarita, CA, USA) were placed via transjugular and transhepatic accesses and 3% sodium tetradecyl sulfate (Sotradecol; AngioDynamics, Latham, New York) injection was performed from the transhepatic access into the varicosity (Figure 4). The foaming characteristics of Sotradecol felt to be optimal for use in this situation given success in similar conditions such as gastric varices. 6
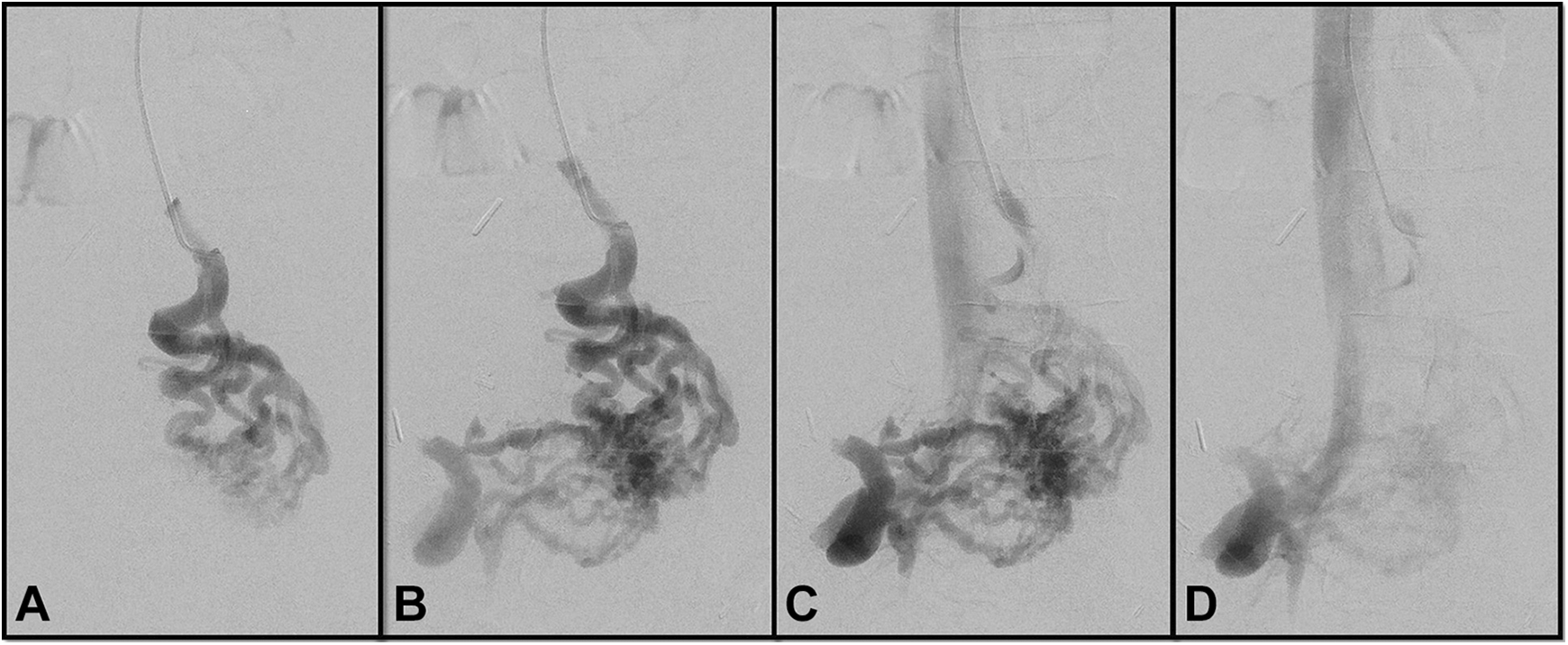
Transhepatic portal venous access and superior mesenteric vein (SMV) venogram shows a very large veno-venous fistulous communication consisting of jejunal varicose veins communicating the SMV branches into the nidus of the ectopic varices and then to the venous outflow of the pancreas graft through the donor iliac vein into the inferior vena cava. (A-D) are sequential phases of contrast injection.
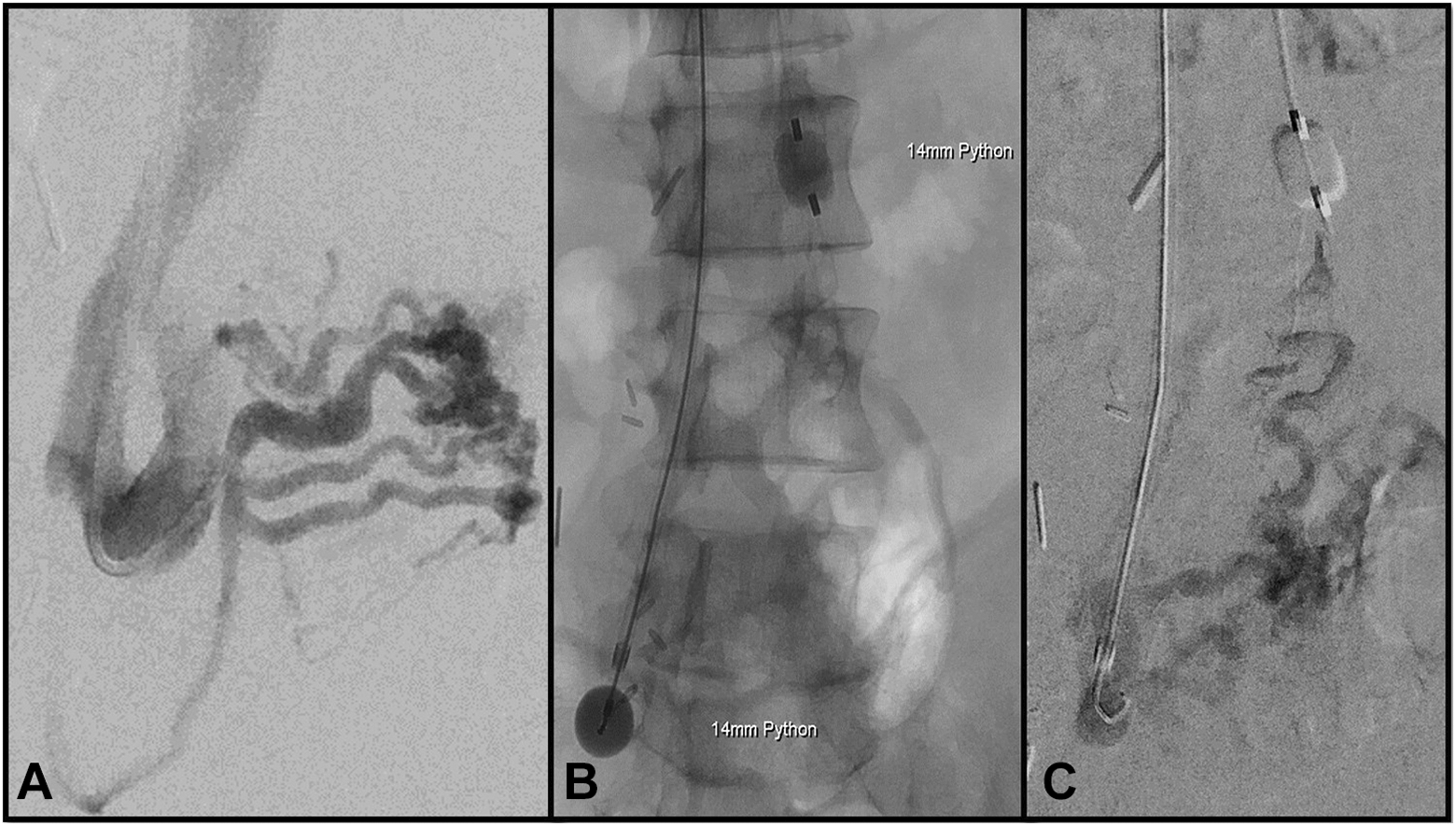
Stage 1 embolization of the ectopic varicose veins. A, Venogram from right internal jugular access with the catheter tip in the iliac vein of the allograft. Contrast fills retrogradely into the ectopic varices consisting of network of varicose veins in superior mesenteric vein (SMV) distribution communicating with the venous drainage of the graft and then into inferior vena cava. B and C, Attempted sclerotherapy of varicose veins to obliterate the nidus using Python Occlusion catheters in the systemic and portal systems and filling the network of the veins with Sotradecol.
Patient presented after 3 weeks with another GIB episode. A repeat transhepatic percutaneous portal venous access showed no apparent treatment effect from prior sclerotherapy. Onyx compatible balloon occlusion microcatheter (Scepter XC balloon microcatheter X-tra compliant; Microvention Terumo) was used and ethylene vinyl alcohol (Onyx 18; EV3-Covidien, Minneapolis, MN, USA) mixed with dimethyl sulfoxide was injected into these veins (Figure 5). Attempts were made to avoid embolization of veins at immediate vicinity of bowel to prevent ischemia. Completion venograms showed obliterated nidus of the ectopic varices.
Stage 2 embolization using Onyx in the nidus of the ectopic varices. A, Digital angiographic view of embolization shows complete obliteration of flow toward the pancreas graft venous outflow. B and C, Axial and coronal reconstruction computed tomography scan views 1 month after the procedure showing embolization of the superior mesenteric vein branches adjacent to wall of the native jejunum.
Approximately 3 weeks after Onyx embolization of jejunal varicosis, the patient presented with another GIB. Computed tomography angiogram showed no active extravasation, but some mesenteric veins in the vicinity of donor duodenum. There was nonocclusive thrombus in the native right portal vein, but otherwise no liver injury or signs of bowel ischemia. This episode also spontaneously resolved, but he presented 6 weeks later with another GIB and finally underwent resection of involved native jejunal segment and donor distal duodenum (D3 segment) while preserving the pancreas graft. There were multiple engorged veins anterior to donor duodenum which bled briskly during adhesiolysis and no other GIB sources identified. Exocrine drainage of pancreas transplant was revised and a pancreaticoduodenal-jejunostomy using D2 duodenal segment and uninvolved jejunum was created. Pathology confirmed varicose veins in the mesentery adjacent to wall of the jejunum (Figure 6). Clinical follow-up for 12 months after surgical resection has been negative for GIB.
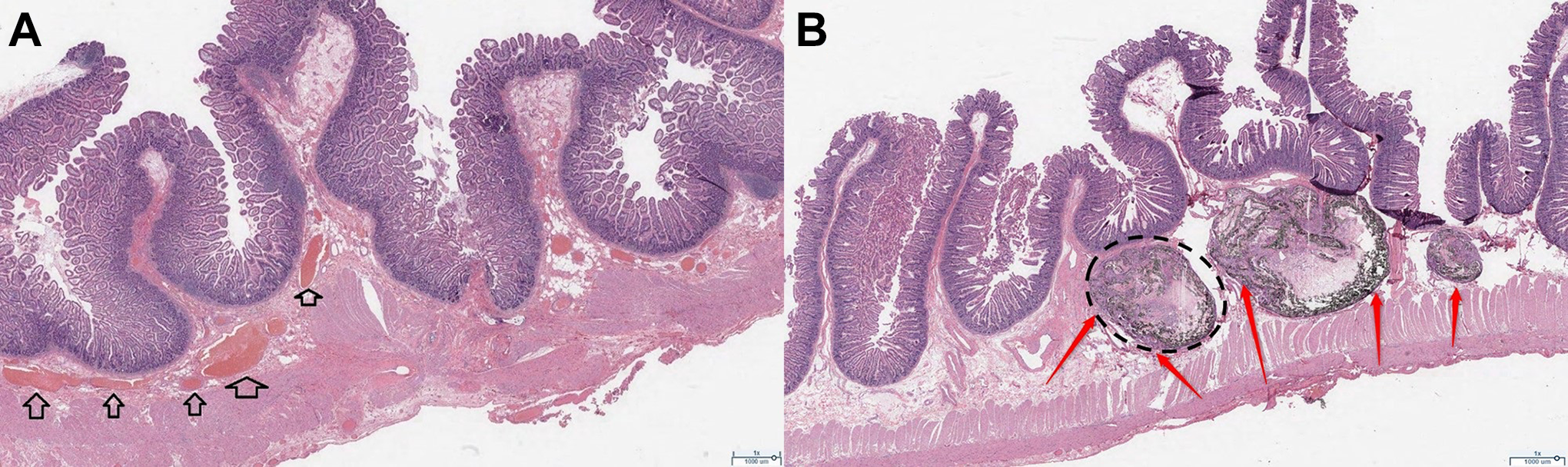
Surgical pathology specimens (H&E ×10). A, Severely dilated venules in the wall of donor duodenum (black arrows). B, The jejunal segment with areas of giant cell foreign body reaction and thrombosed veins (dotted circle) with tattoo deposits (red arrows) from embolization.
Discussion
Ectopic variceal bleed is seen in 1% to 5% in cirrhosis, 7 27% to 40% in extrahepatic portal hypertension, and up to 64% in coexisting portal venous occlusion and hepatobiliary surgery. 8 Bass et al 9 reported jejunal variceal bleed in pediatric cases after liver transplant with portal thrombosis. Hyun et al 10 reported delayed jejunal variceal bleed at hepaticojejunostomy or choledochojejunostomy anastomosis in the setting of portal venous occlusion. “Transcapsular hepatic collaterals” are described 8 in portal venous occlusion after liver transplantation, pancreatoduodenectomy, 11 or hepaticojejunostomy likely due to inflammatory adhesions. Although portal venous pressures were not directly measured in this case, lack of liver or portal venous disease argues against portal hypertension. The trauma of surgery and possibly infection around the pancreatic graft were likely the inciting factors. Alternatively, poor venous drainage of the donor duodenum might have been a contributing factor. Even though we saw widely patent venous drainage to the iliac vein during venograms, smaller veins might have been compromised. Finally, an episode of rejection could be a theoretical plausible trigger, but no rejection episodes occurred during this case and pancreas graft function remained within normal limits.
Unlike esophageal or gastric varices, the diagnosis and treatment of jejunal varices are challenging. Anecdotal reports are available for endovascular treatment of ectopic varices. Wang et al 12 presented 2 cases of portal hypertension–related parastomal variceal bleeding treated with Onyx and coil embolization. Similar varicose veins are described in a donor duodenum in a patient after kidney–pancreas transplant, 13 but in the setting of portal hypertension, who was treated successfully with coil embolization and subsequently underwent liver transplant. Surgical resection of the varicose veins in the small intestine has been reported, 14 but in our patient, this was kept as last resort, given surgical morbidity and potential need to explant a functioning pancreas allograft. The main consideration for our endovascular approach was risk of bowel ischemia.
There was a possibility that the obliteration of the varicose veins from transhepatic approach was incomplete. This can be suggested by the difference between extent of varices on Figure 4A and the spread of Onyx on Figure 5A, which shows that perhaps a more diffuse spread of Onyx could have resulted in further obliteration of the duodenal side of varices. The lack of complete clinical response to jejunal varicosis obliteration could therefore be linked to residual varicose veins in the donor duodenum not accessible via transhepatic portal access.
In conclusion, this is a report of ectopic varices after pancreas transplant in a noncirrhotic patient. The management of GIB in patients with pancreas transplant mandates exploration for the ectopic varices if no other source identified.
Footnotes
Authors’ Note
Nassir Rostambeigi contributed to study design, data collection, manuscript writing, and revisions. Prashant Shrestha contributed to study design, manuscript writing, and revisions. Ty B. Dunn contributed to study design, manuscript writing and revisions, and surgical interventions. Jafar Golzarian contributed to study design, manuscript writing, and revisions. Pooria Khoshnoodi contributed to manuscript writing and revisions and pathological evaluation. Michael Rosenberg contributed to study design, manuscript writing, and revisions. Reza Talaie contributed to study design, manuscript writing, and revisions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.