
Abstract
Endovascular treatment of chronic mesenteric ischemia is currently the treatment of choice, regardless of the number of involved vessels. Unlike other anatomic areas, the hyperperfusion produced by revascularization and the consecutive reperfusion syndrome is only described in cases of acute bowel ischemia, which is usually resolved with traditional surgery. We present a case of severe hyperperfusion syndrome secondary to endovascular correction with stents of a critical ischemia affecting the celiac trunk and superior mesenteric artery.
Introduction
Chronic mesenteric ischemia (CMI) is a rare but catastrophic disease. The typical symptoms are postprandial central abdominal pain, food phobia, and significant weight loss. The diagnosis is often difficult because these symptoms are nonspecific and they are present in many digestive pathologies. In addition, most of the patients are elderly and present with atherosclerosis in the visceral vessels. Consequently, there is a delay in the diagnosis and treatment in many cases of CMI. In a small percentage of cases, this delay may lead to the development of ischemic colitis (IC), which causes tissue changes in the colon secondary to decreased blood flow. These findings are confirmed by colonoscopy and histopathology. 1,2
Chronic forms represent 10% to 25% of the cases and present as segmental IC or colonic stenosis. 3 Only 10% of cases involve the right colon in isolation as in the case we are presenting.
Most of these patients present with occlusion or critical stenosis of the superior mesenteric artery (SMA) and at least one other mesenteric vessel, usually the celiac trunk (CT). If the mesenteric ischemia is not resolved, it usually progresses to cachexia and ischemic damage in the bowel, which may lead to death. 4 -6
Currently, endovascular therapy is the first-line treatment for these patients when the anatomy of the injuries allows for it, regardless of the surgical risk classification of the patient. These procedures present with low rates of morbidity, mortality, and complications. Among them, the most often-described complications are related to vascular access, renal failure, acute bowel ischemia secondary to distal embolism, cardiac events, and respiratory complications. 6 -10 In rare cases, secondary damage due to reperfusion occurs with hemorrhagic manifestations that occur less commonly in the bowel than in other areas.
However, inflammatory manifestations secondary to the ischemia–reperfusion (IR) phenomenon have been predominantly linked to acute ischemic processes. 11 We present a case in which multiple revascularization of the mesenteric circulation caused a situation of hyperperfusion with typical manifestations of IR damage in a patient with chronic IC.
Case Presentation
The patient is a 68-year-old woman who had severe abdominal pain related to ingestion in the setting of CMI. Her past medical history included arterial hypertension and dyslipidemia as well as ischemic heart disease treated with a drug-eluting stent 6 years ago, which had remained stable since then.
The patient presented with postprandial pain and progressive weight loss for the past 4 years. She had been evaluated by Digestive and was diagnosed with segmental IC, which exclusively affected the right colon. At the vascular level, a critical stenosis of the SMA and the CT had been diagnosed through computed tomography angiogram (CTA), while the lower mesenteric artery remained patent.
At that time, she had been treated by the Radiology Department, where they placed a 5 × 17-mm balloon-expandable stent (Visi-Pro; Medtronic, Madrid, Spain) in the SMA. The stenosis of the CT was caused by a preocclusive plaque that affected the ostium of the artery and technically was not covered in that procedure.
The improvement in the patient after the procedure was only partial. As a result of the IC, she developed colonic fibrous stenosis at the hepatic angle level, which required periodic endoscopic dilatations.
In the last year, the situation had substantially worsened, reaching severe levels of decreased body weight, weakness, and undernourishment. When the patient was seen again by Digestive, the occlusion of the mesenteric stent was confirmed by CTA, and the patient was referred to our angiology and vascular surgery department. We studied the case and recommended multivessel endovascular treatment.
Using a retrograde femoral approach, we performed an aortography in the lateral view with a full deployment of the visceral arteries outlet. We confirmed the stent occlusion of the SMA as well as the presence of a preocclusive short stenosis in the proximal CT (Figure 1A). An intravenous heparin (5000 UI) bolus was administered. We started by placing an Aptus TorGuide 7F introducer (Medtronic) into the visceral aorta. This introducer significantly facilitated the recanalization of these injuries because it allows us to start with the distal end and place it on the anterior aortic wall in the arterial ostium; this provides a high degree of stability, even when the disease is so severe that we cannot identify the arterial ostium with certainty. Thus, we first recanalize the preocclusive stenosis of the CT (Figure 1B).
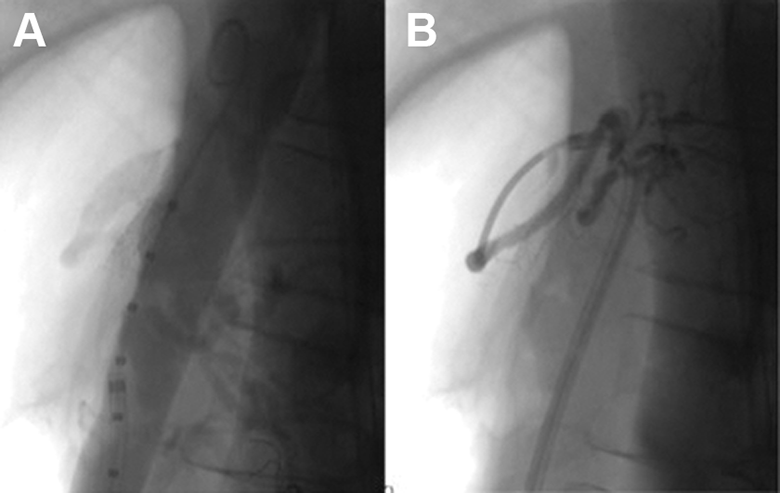
Aortography in lateral view, where the preocclusive stenosis of the CT and the occlusion of the stent of the SMA is shown (A). Recanalization of the CT (B). CT indicates celiac trunk; SMA superior mesenteric artery.
We progressively predilate the injury, maintaining a residual critical stenosis. We complete the treatment by placing an 8 × 37-mm balloon-expandable stent (Visi-Pro, Medtronic), which overcomes the stenosis resistance with a good angiographic result (Figure 2).
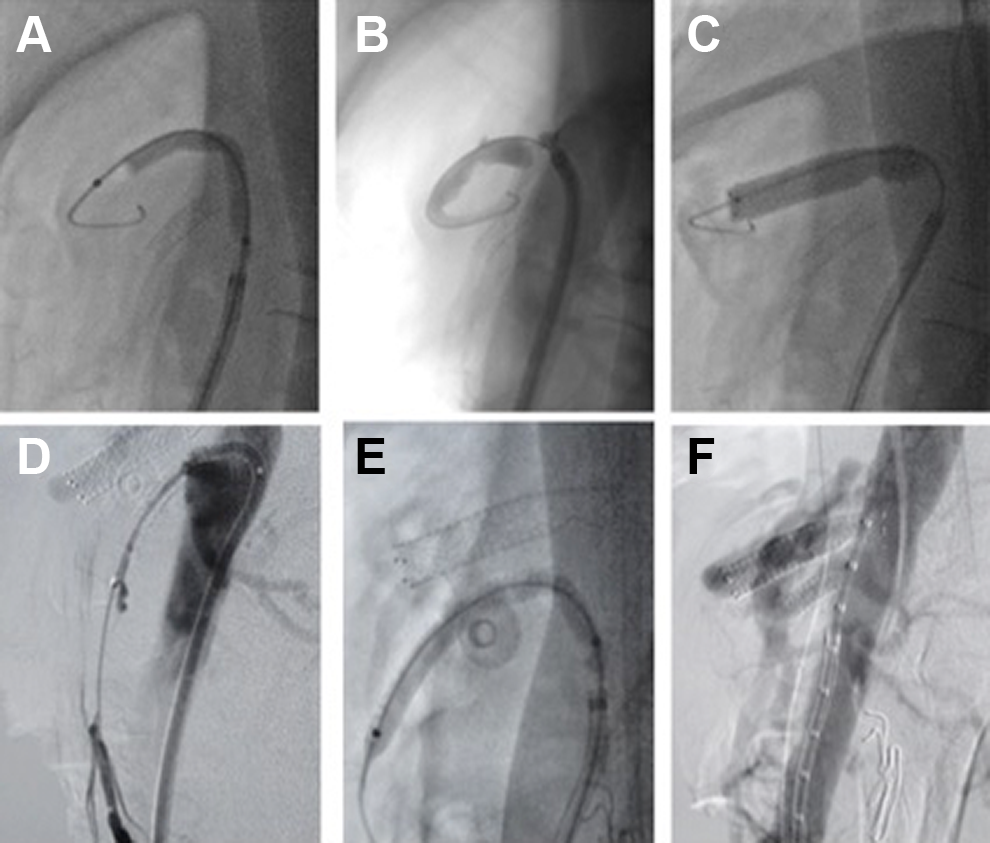
Angioplasty of the stenosis of the CT (A). Residual critical stenosis at the arterial ostium level (B). Balloon expandable stent placement (C). Recanalization of the occluded stent by means of a microcatheter (TrailBlazer, Medtronic) and working guide of low profile (Command, Abbott, Madrid, Spain) (D). Angioplasty with drug-eluting balloon (E). Final aortography with a good angiographic result (F). CT indicates celiac trunk.
Next, we recanalize the occluded stent of the SMA by using a low-profile material (Figure 3A), and we perform an angioplasty with a 5 × 40-mm drug-eluting balloon (Admiral In-Pact; Medtronic), recovering the occluded stent (Figure 3B). After the complete revascularization of both arteries

Highlighted and thickening of the gastric mucosa (A) as well as marked dilation of the bowel loops with edema and diffuse significance of all the intestinal mucosa (B and C).
During the postoperative period, a progressively painful abdomen, distension, and bloating developed within the first 48 hours. The kidney function deteriorated, presenting as oliguria, and respiratory distress developed as well, presenting as dyspnea.
An urgent CTA was performed, which proved that both stents remained patent, but there was a prominent significance that was highlighted in the gastric mucosa and the bowel loops in a diffuse way (Figure 4), along with the presence of abdominal free fluid in the peritoneal cavity (Figure 5). In the chest, there was a bilateral pleural effusion (Figure 6). The condition corresponded to IR syndrome secondary to hyperperfusion after the visceral revascularization that was performed in the previous days.

Ascites, presence of abdominal free fluid.
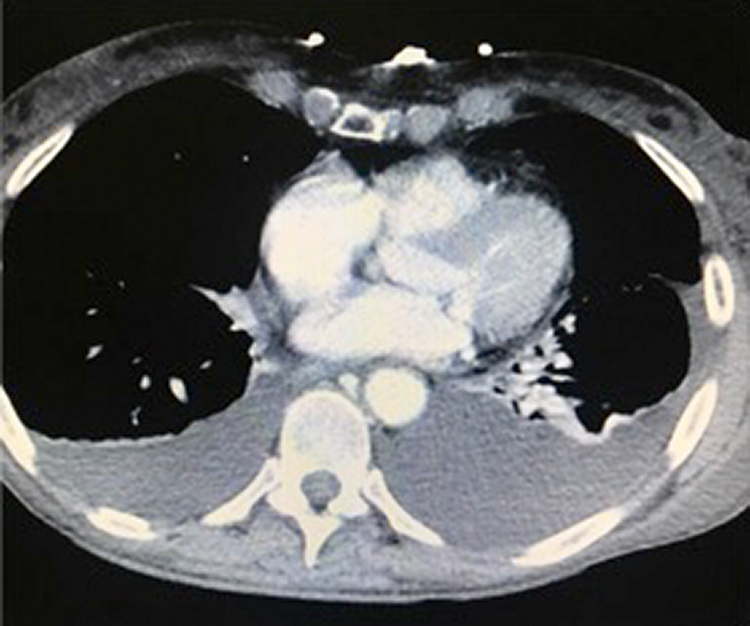
Bilateral pleural effusion.
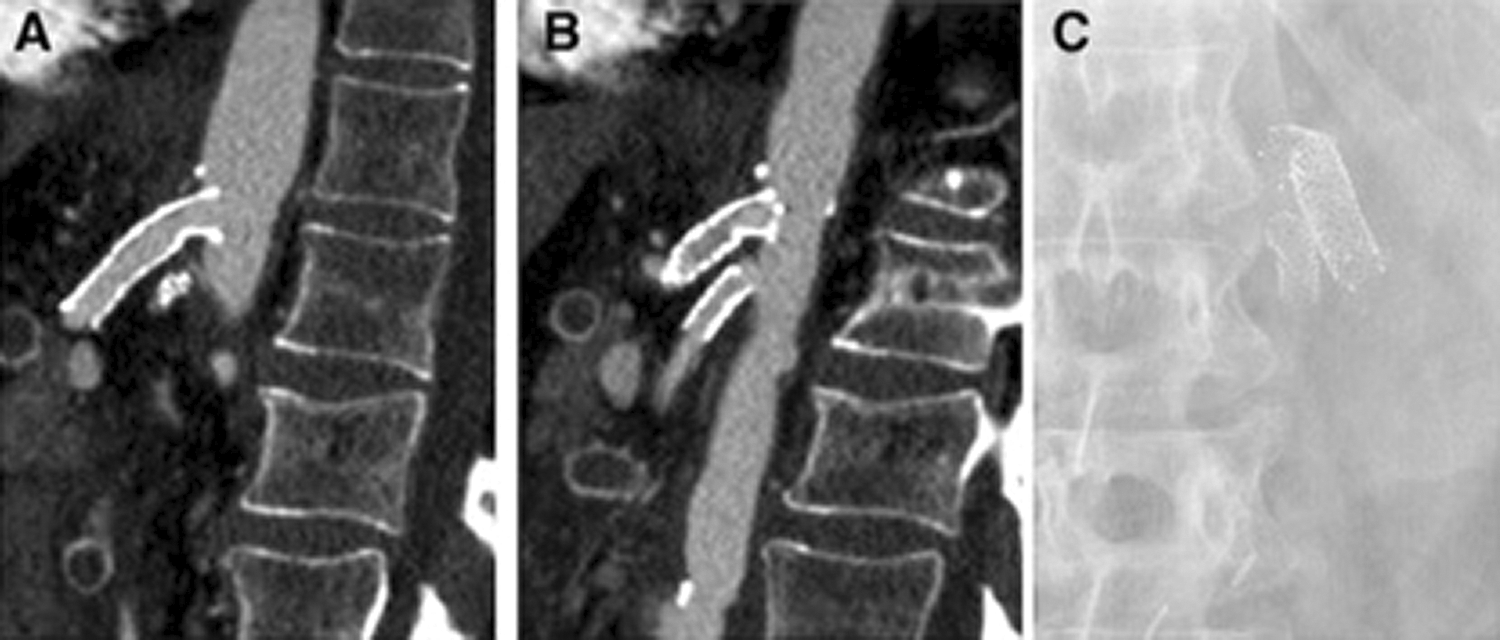
Stent patency in CT (A) and in SMA (B). Three-dimensional reconstruction of the stents (C). CT indicates celiac trunk; SMA superior mesenteric artery.
The patient was admitted to the intensive care unit, where her clinical situation was optimized with conservative measures. After 72 hours of digestive rest, parenteral nutrition, and depletive treatment, she showed significant clinical improvement.
One year later, the patient w feeling well, has gained weight, and the intense abdominal pain that she presented with after meals has disappeared. A follow-up was performed with Doppler ultrasound, which showed that both stents remained patent.
Discussion
The IR phenomenon is a complex pathologic process that is produced at the cellular and extracellular levels and involves both metabolic and inflammatory changes. In recent years, the experimental models have allowed for a deeper knowledge about its pathophysiology in the bowel. 12 -14
The bowel is one of the organs that is the most sensitive to IR. It is made up of labile cells that have high levels of metabolic damage in ischemic situations. The restoration of an appropriate blood flow to these ischemic tissues may lead to a cascade of events that cause increased cellular damage following reperfusion.
In this process, a series of mediators have been described as being involved, such as polymorphonuclear white cells, nitric oxide, oxygen free radicals, pro-inflammatory proteins, “heat shock” proteins (of intracellular stress), endothelins, complement, heme oxygenases, and iron. The damage is also related to an increase in the proinflammatory cytokine circulation, such as interleukin 6 and the tumor necrosis factor alpha which are released by the bowel itself. This fact means that distant organs, such as the lungs, liver, or kidneys, might cause a systemic inflammatory response syndrome or multiorgan failure.
The IR syndrome is accompanied by a decrease in the contraction of the bowel, an increase in vascular patency, bacterial overgrowth, and mucosal barrier dysfunction. 12,14 -17
The severity of this phenomenon continues to be a very controversial subject. This is partly due to the fact that the reperfusion injury rate seems to depend on the type of ischemia (complete or partial vascular occlusion), the length of time ischemia has been present, and which segment of the bowel is affected.
In previously published studies, this process has been primarily described as being the result of an abrupt discontinuation of the blood flow as would occur during an embolism or mesenteric acute thrombosis, an aortic aneurysm surgery, septic or hypovolemic shock, and other circumstances. 12 -17
In our case, the severity of this phenomenon as a response to the reperfusion was remarkable, especially in the setting of a CMI, in a patient with advanced IC and where a certain degree of ischemic preconditioning exists. 18
In conclusion, the development of experimental models in recent years has enabled a better understanding of the mediators that participate in the phenomenon of IR in the bowel.
It has been seen that the pathophysiological response to reperfusion in mesenteric ischemia varies considerably based on multiple factors, such as the duration of the ischemia, its severity, the bowel sector involved, and the possibilities of compensation by means of replacement mechanisms that exist in the visceral vascular anatomy.
However, the knowledge about the impact of these factors continues to be modest, and many questions still exist and must answered in order to better understand these mechanisms and how multiple revascularizations can affect the severity of this phenomenon. Future studies must address the implementation of this knowledge about intestinal IR, with the aim of improving the screening processes, prevention, and treatment.
Footnotes
Authors’ Note
Informed consent has been obtained from the patient for publication of the case report and accompanying images.
Declaration of Conflicting Interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.