
Abstract
The association between pancreaticoduodenal artery aneurysm (PDAA) and local hemodynamic changes in pancreaticoduodenal arcades is well established. However, there are few case reports of PDAA associated with acute aortic dissection. In this article, we outline and discuss the case of a 61-year-old man diagnosed with a type A acute aortic dissection who underwent emergency surgery and developed sudden-onset severe abdominal pain and shock 10 days later. Contrast-enhanced computed tomography showed a ruptured PDAA with feeding vessels from the gastroduodenal and superior mesenteric arteries, with evidence that the celiac artery was diverged from a false lumen. Transarterial embolization via the superior mesenteric artery alone was not expected to achieve hemostasis, so we performed a hybrid procedure involving transarterial embolization cannulated from superior mesenteric artery with complementary surgical ligation of the gastroduodenal artery. The postoperative course was uneventful, and follow-up contrast-enhanced computed tomography showed no persistence of the aneurysm 8 days after the second operation. This case proposed that visceral arterial malperfusion due to acute aortic dissection can cause PDAA in the early postoperative period. Although previous reports suggest that endovascular treatment is preferable, it may not always be feasible. Since ruptured PDAAs are often not detected during surgery, surgical treatment can be overly invasive. Whereas, transarterial embolization with complementary clamping or ligation of the gastroduodenal artery for ruptured PDAA is less invasive and can control hemorrhage, especially when cannulation to the celiac artery is impossible. Notably, the technique did not cause organ ischemia, presumably because the small collateral vessels of the pancreaticoduodenal arcades permitted sufficient blood flow. If endovascular treatment is unable to achieve rapid hemostasis, this technique may be a useful option for ruptured PDAA.
Keywords
Introduction
The pancreaticoduodenal arcade is an arterial network that encircles the pancreatic head, connecting the celiac artery (CA) and superior mesenteric artery (SMA). 1 It is thought that increased blood flow to the small and fragile vessels of the arcade cause pancreaticoduodenal artery aneurysms (PDAAs) through local arterial hypertension and weakening of vessel walls. 2,3 This theory has been supported by flow-sensitive 4-dimensional magnetic resonance imaging. 1,4 Recently, an association has also been shown between PDAA and CA lesions, and there are a few case reports of PDAA being associated with acute aortic dissection (AAD). 5,6
Pancreaticoduodenal artery aneurysms are clinically important because most are found after ruptured, leading to fatal hemorrhage and high mortality rate. 7 The superiority of endovascular treatment over open surgery for PDAAs has been reported. 8 However, this approach may not always be feasible. There are few reports of treatment options in such situations, especially for less invasive approaches.
In this case report, we describe successful treatment by transarterial embolization (TAE) of the inferior pancreaticoduodenal artery (IPDA) with complementary surgical ligation of the gastroduodenal artery (GDA) in a patient with PDAA rupture.
Case Report
A 61-year-old man with an otherwise unremarkable medical history was referred for assessment of neck and shoulder pain. He did not present any risk factors for cardiovascular diseases, such as hypertension. Contrast-enhanced computed tomography (CT) showed a Stanford A type AAD (Figure 1A), but no visceral artery aneurysms (VAAs), including PDAA, were observed (Figure 1B). He was transported to our hospital where he underwent emergency replacement of the ascending aorta. Postoperatively, his blood pressure was within the normal limit, and laboratory data did not show abnormalities. On day 10 after surgery, he developed sudden-onset, severe abdominal pain and his systolic blood pressure fell to 60 mm Hg that recovered to 100 mm Hg with fluid resuscitation. Contrast-enhanced CT showed a PDAA with a massive retroperitoneal fluid collection (Figure 2). Inflow vessels to the PDAA were seen to originate from both the GDA and the SMA, and the AAD was noted to have reached the aortic bifurcation (Figure 3). Preoperative diagnosis was of PDAA rupture with hemorrhage shock. The diagnosis of postoperative pancreatitis was not considered because the patient’s pancreatic enzyme level was within the normal limit on performing blood examination during the postoperative course. The patient responded transiently to fluid resuscitation with crystalloids and a blood transfusion.
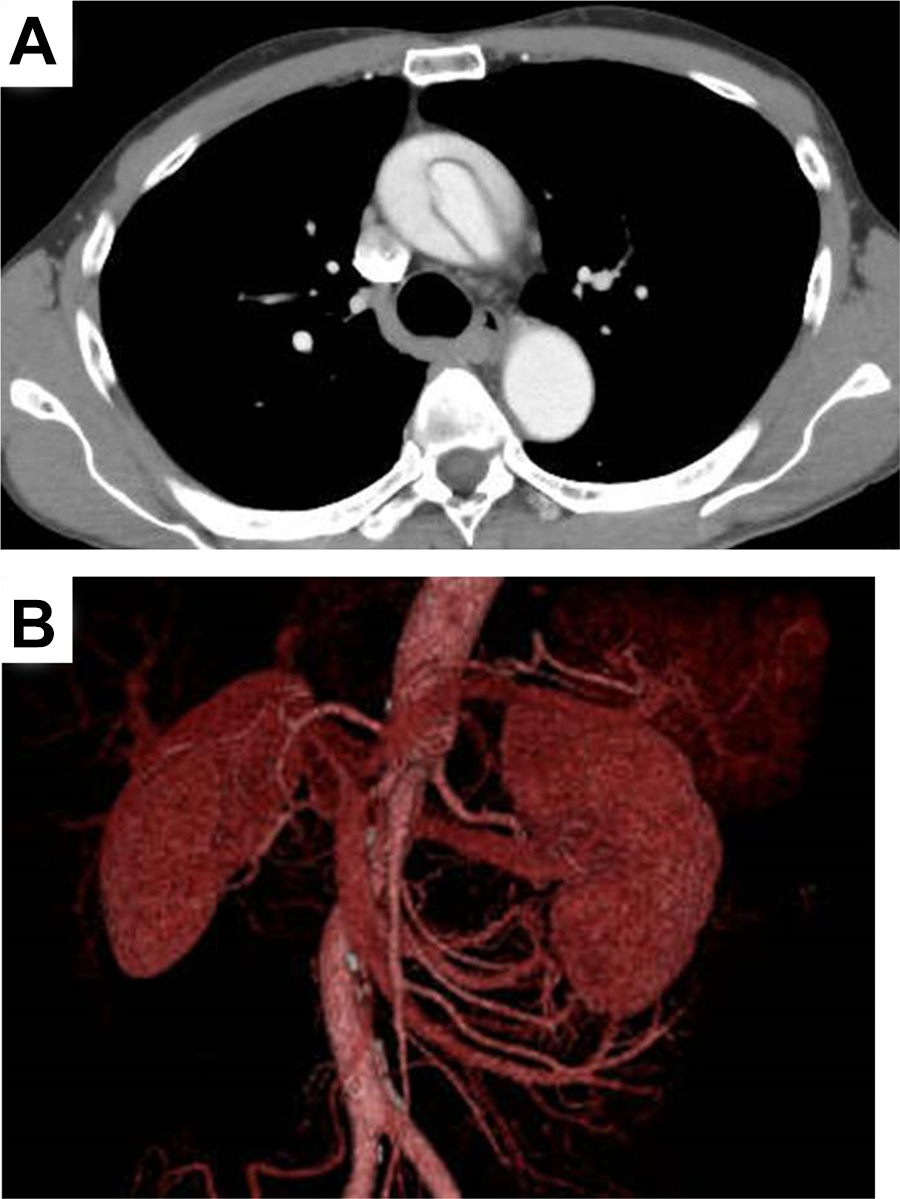
Initial contrast-enhanced CT findings. A, Results showed type A AAD. No aortic dissection was observed in the descending aorta. B, Pancreaticoduodenal artery aneurysm was not detected in 3-dimensional image reconstruction. AAD indicates acute aortic dissection; CT, computed tomography.
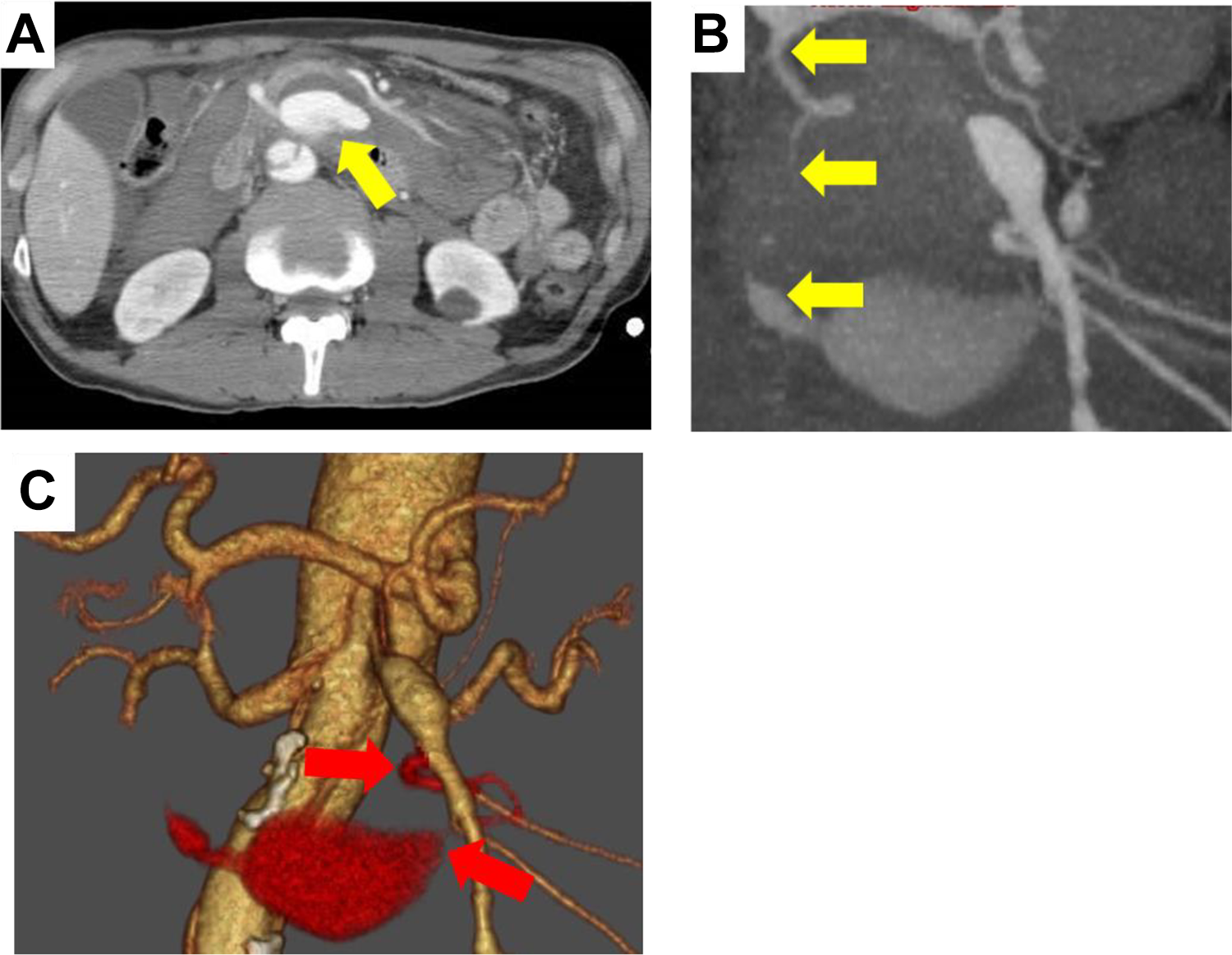
Preoperative contrast-enhanced CT findings. (A) A ruptured PDAA (yellow arrow) with massive retroperitoneal fluid collection was detected. (B) Feeding vessel connected to GDA (yellow arrows) is shown. (C) Feeding vessel originating from SMA (red arrows) is shown. CT indicates computed tomography; GDA, gastroduodenal artery; PDAA, pancreaticoduodenal artery aneurysm; SMA, superior mesenteric artery.
Contrast-enhanced CT revealed AAD reaching the aortic bifurcation. The diameter of the false lumen was larger than that of the true lumen. CA had diverged from the false lumen (A), whereas SMA had diverged from the true lumen (B). AAD indicates acute aortic dissection; CA, celiac artery; CT, computed tomography; SMA, superior mesenteric artery.
Endovascular treatment was initially considered for the PDAA rupture. However, cardiologists observed that an intravascular approach from the CA would be difficult because it diverged from the false lumen and that embolization of feeding vessels from the GDA was unlikely given the known difficulties passing a catheter through a ruptured aneurysm. Despite this, it was noted that embolization of the feeding vessels from the SMA was possible. Surgeons therefore recommended clamping the GDA to reduce blood flow of the pancreaticoduodenal arcade and asked cardiovascular surgeon to prepare for revascularization, if necessary. After obtaining informed consent, the patient underwent the proposed hybrid surgery as an emergency.
Under general anesthesia, the GDA was accessed via an upper median incision. The PDAA rupture did not affect the GDA, but a hematoma was noted to markedly affect the aneurysm, making a direct surgical approach to the PDAA difficult. Surgeons therefore clamped the GDA with Bulldog forceps, as planned, before asking the cardiologists to perform endovascular treatment. The right femoral artery was cannulated using a 6F gage sheath catheter and SMA angiography showed the ruptured PDAA and the associated inflow and outflow vessels (Figure 4A). The outflow vessel was connected to the clamped GDA-like preoperative CT finding (Figure 4B). Under selective angiography, catheter could not cannulate the outflow vessel. Therefore, TAE of the inflow vessel was performed with coil. After TAE, surgeons confirmed that there was no ischemic response to the GDA clamping and ligated the GDA to reduce blood flow into the aneurysm. Superior mesenteric artery angiography was repeated and revealed that another branch flowed into the aneurysm (Figure 4C). This branch flowed to the initially imaged outflow vessel connecting to the GDA. Cardiologist repeated the coil-based TAE, and complete embolization of PDAA was achieved (Figure 4D). We did not perform revascularization because there was no ischemic response. The procedure lasted 260 minutes, and the patient’s hemodynamic state remained stable throughout.
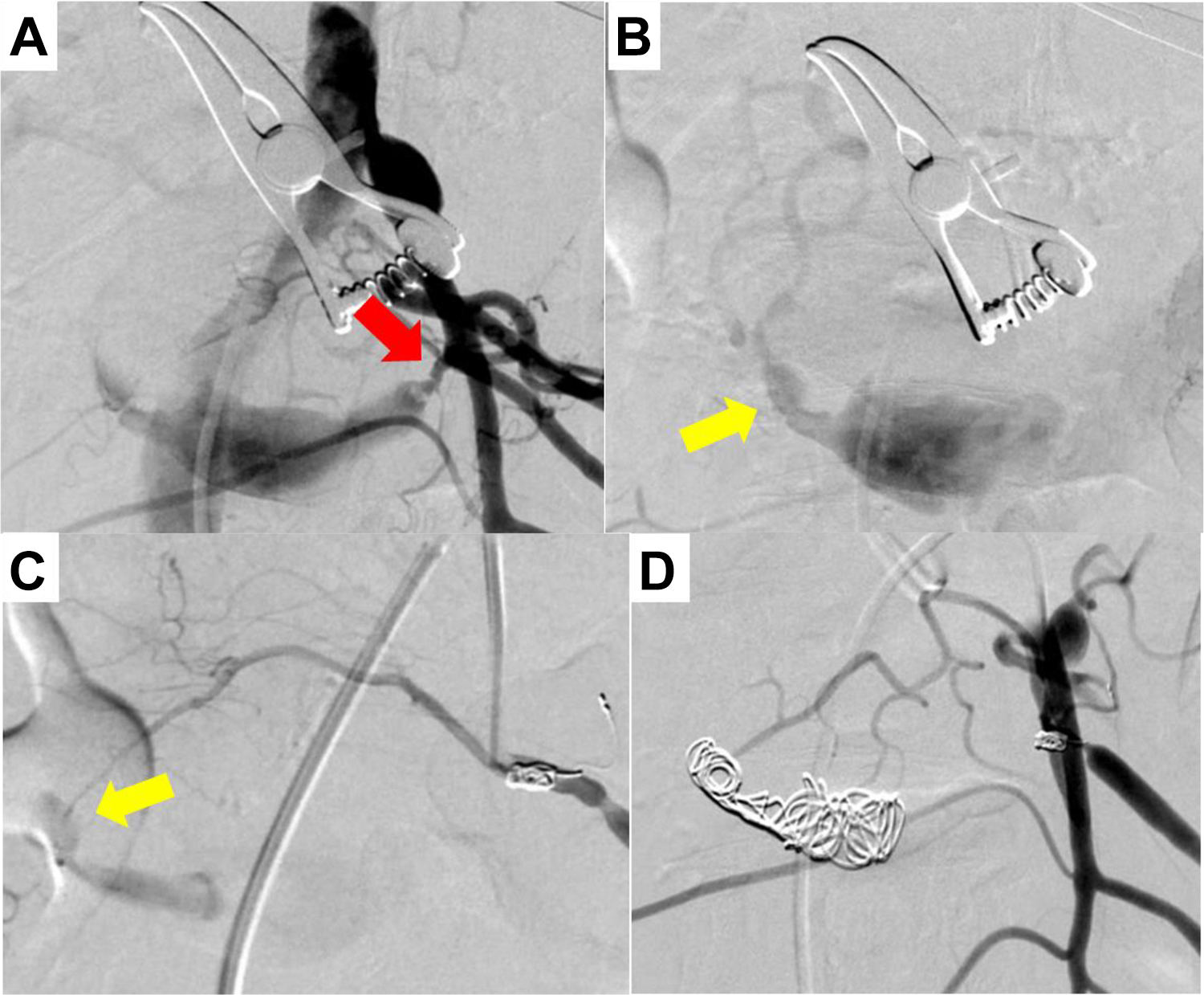
A, SMA angiography revealed the ruptured PDAA and inflow vessel (red arrow). B, The outflow vessels (yellow arrow) were connected to GDA clamped with Bulldog forceps. C, Repeated angiography revealed another branch to the aneurysm. This branch flowed to the initially imaged outflow vessel (yellow arrow). D, Final angiography revealed that both inflow and outflow vessels were embolized with coil. GDA indicates gastroduodenal artery; PDAA, pancreaticoduodenal artery aneurysm; SMA, superior mesenteric artery.
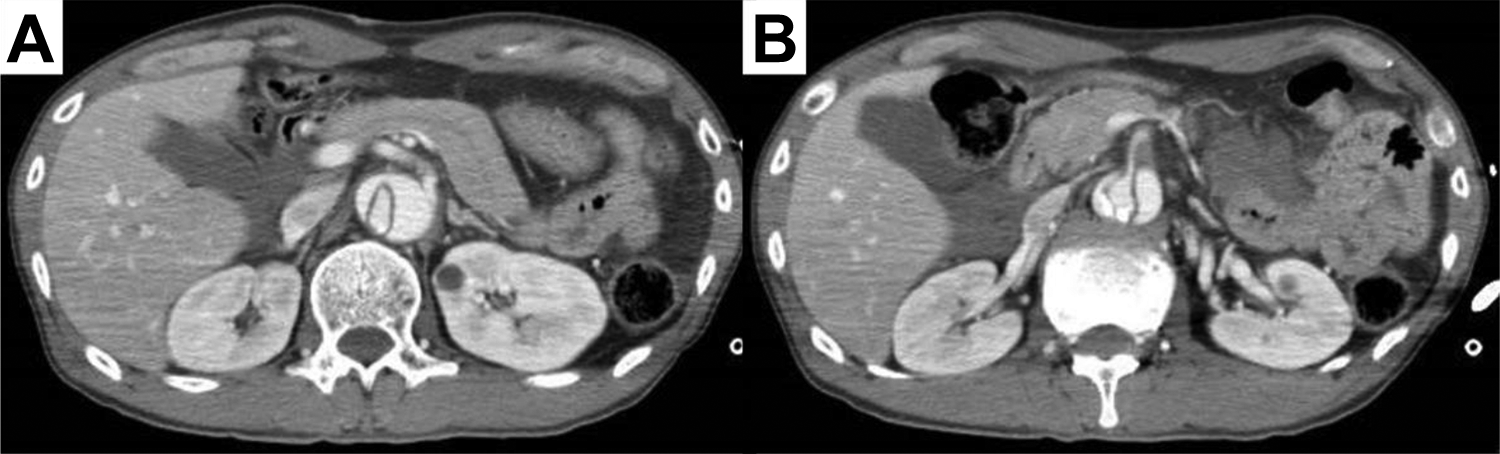
A follow-up CT 8 days after the second operation confirmed that there was no persistence of the aneurysm. The contrast effect of the dominant area of the pancreaticoduodenal arcade was enough to prevent ischemic changes. He then underwent rehabilitation and was discharged 23 days after the second operation. Follow-up CT 1 month after the second surgery revealed no new aneurysm or ischemic response. We plan to perform further outpatient follow-up every 6 months.
Discussion
The number of VAAs found incidentally has increased, since the use of diagnostic imaging has become more widespread. 9,10 Pancreaticoduodenal artery aneurysms account for 2% of all VAAs, 6,11 but unlike other VAAs, PDAAs have not shown a clear correlation between size and propensity to rupture. 3 In a review of 88 PDAAs, 53 (60%) ruptured, of which 26 (49.1%) were fatal. 6 Pancreaticoduodenal artery aneurysms usually rupture into the retroperitoneal space, causing hypotension or shock, 12 and treatment is associated with high mortality and technical difficulty. 10 In emergencies, prompt and appropriate management is typically required, necessitating that we share our treatment experiences to establish a set of viable options for use in different settings.
Mesenteric malperfusion caused by AAD occurred as a complication in 3.8%, 13 and its mechanisms have been reported by Orihashi. 14 In our patient’s initial CT image, the AAD did not reach the abdominal aorta and there was no PDAA, indicating that the AAD progressed to the aortic bifurcation by the time of the repeat imaging. Therefore, AAD was considered to have progressed distally during the transportation or replacement or following the replacement of the ascending aorta. True PDAAs have been linked to hemodynamic alternations in the involved visceral branches. 10 We hypothesize that the hemodynamics of the CA and SMA were altered when the AAD reached the bifurcation, changing the hemodynamics of the pancreaticoduodenal arterial arcade and causing the PDAA. The patient recovered normally after the first emergency surgery for AAD until he suddenly developed severe abdominal pain on postoperative day 10. Other than visceral arterial malperfusion, pathological conditions causing aneurysm, such as postoperative pancreatitis, were not observed. We therefore suggest that visceral arterial malperfusion due to AAD can cause PDAA in the early postoperative period.
Transarterial embolization of both the inflow and the outflow arteries of an aneurysm is the most common treatment of VAAs. 9 However, TAE is not always technically feasible because of difficulties in selective cannulation of the feeding vessels of the aneurysm. 15,16 Surgical treatment for PDAA varies from ligation or resection of an aneurysm to pancreatectomy. Pancreaticoduodenal artery aneurysms are often located behind or within the parenchyma of the pancreas and may not be detected at surgery in about 70% of cases. 15,17 In another report, 3 of 6 patients with PDAA rupture had to undergo emergency pancreatoduodenectomies because visualization was not possible due to the presence of massive retroperitoneal hematomas. 15 Ushijima et al reported a case of PDAA requiring distal pancreatectomy to complete the aneurysm resection. 7 Therefore, ruptured PDAAs may require invasive surgical treatment. 7 We considered pancreatoduodenectomy to be overly invasive for our patient and that it would have resulted in avoidable morbidity or mortality. It seems necessary to establish minimally invasive surgical techniques.
In this case, contrast-enhanced CT showed inflow of contrast agent from both the GDA and SMA. Cardiologists considered that cannulating the CA or passing through the ruptured aneurysm was not possible, predicting that hemostasis could not be achieved with TAE alone. On the other hand, direct surgical approach to the ruptured PDAA was also expected to be difficult as well as previous report. As an alternative procedure, surgical clamp of GDA was proposed for temporary control of bleeding.
In a previous report, concerns were noted about the risk of aortic rupture in the subacute phase of aortic dissection around the orifices of the CA and SMA when using endovascular treatment. 5 However, our case experienced no such complications. The urgent endovascular repair of ruptured PDAAs was still associated with significant morbidity and mortality. 18 Recently, the immediate technical success rate for TAE with ruptured PDAAs was only 57%, 12 while in another, embolization via the SMA approach was only successful for PDAAs with CA lesions in 10% to 40% of cases. 9 In this case, his hemodynamics could be stabilized after clamping of GDA and initial TAE. We believe that GDA clamping permitted temporary control of the bleeding, which allowed us to stabilize the patient’s hemodynamics before complete embolization. Additional SMA angiography fortunately revealed the collateral vessel to the aneurysm, which was not initially shown. Gastroduodenal artery clamp increased blood flow from SMA to pancreaticoduodenal arcade, which may have facilitated the detection of small collateral vessel pathway to aneurysm. Repeated TAE achieved embolization of aneurysm. Surgical clamp of GDA can be expected to markedly reduce blood flow into an aneurysm, resulting in hemostasis due to tamponade in the retroperitoneal cavity, especially in cases that cannulation to the CA is impossible. Suzuki et al reported that significant reduction in the flow to the aneurysm may be predictive of future thrombosis. 19 Consistent with our approach, Ricci et al reported that temporary control of bleeding lowered the morbidity and mortality rates. 12 For lethal hemorrhagic lesions, minimally invasive temporary control is important. From our experience, If TAE alone cannot achieve hemostasis, complementary GDA clamping or ligation may help to suppress bleeding and detection of small collateral vessels.
We are not aware of any other case reports of PDAA rupture showing the advantage of GDA clamping or ligation to control bleeding. This technique seems to be an option when cannulation to the CA is not possible. However, when using this technique, there is a valid concern about the potential for organ ischemia, although a trial can confirm the need for revascularization. 15 Otsuka et al reported no cases of foregut ischemia after embolization without revascularization. 2 We also found that GDA clamping did not cause ischemia during endovascular treatment, with the patients having an uneventful postoperative course without organ ischemia by postoperative day 8. This can be explained by the presence of small collateral vessels around the pancreatic head. These include the pancreaticoduodenal arcade and other collaterals between the celiac axis and the SMA, such as the arc of Buhler (an inconstant direct connection between the CA and the SMA), the dorsal pancreatic artery, and the arcs of Barlow (a collateral pathway within the omentum, between the epiploic arteries of the splenic artery and the SMA). 20 Small collateral vessels may prevent organ ischemia after ligation of the GDA and TAE of the IPDA. However, the existence of such collateral vessels remains a risk factor for new aneurysm formation, necessitating careful radiological follow-up at 6 months, and possibly yearly thereafter. 10
We only described our experiences in one patient, which is the main limitation of this case report. Therefore, our technique needs to be trialed in other situations. Also, notable disadvantages of the GDA clamping technique are that the hemodynamics may not be stabilized and that it may cause organ ischemia. Thus, it is necessary to prepare for such eventualities. We hypothesize that intravascular treatment from GDA cannulation could also have been possible, allowing for more selective embolization of the PDAA; to date, however, there have been no reports of endovascular treatment for PDAAs using such an approach. If organ ischemia occurs following this procedure, revascularization is required to secure the blood flow to CA or its branch. For example, SMA to common hepatic artery bypass surgery using saphenous vein graft can be proposed.
In conclusion, TAE with complementary surgical ligation of the GDA was successfully employed to treat PDAA rupture associated with hemorrhage shock. The etiology of PDAA formation was presumed to be AAD progression to the abdominal aorta, altering the hemodynamics of the pancreaticoduodenal arterial arcade. If TAE is unable to achieve rapid hemostasis, a complementary GDA clamping may be a useful option for control of hemorrhage and detection of small collateral vessels. In our experience, TAE of the PDAA with surgical ligation of the GDA is safe and does not cause organ ischemia.
Footnotes
Authors’ Note
T.I., T.H., R.M., and S.T. performed surgical treatment. A.T. and M.A. performed endovascular treatment. N.K. prepared for revascularization T.I. drafted the manuscript. S.T. and H.K participated in the correction of the manuscript. All authors approved the final manuscript. This study was approved by the ethics committee in Nagoya Tokushukai General Hospital (Institutional Review Board approval 2019-03-001). Written informed consent was obtained from patient for publication of this case report.
Acknowledgments
The authors would like to thank Enago (www.enago.jp) for the English language review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.