
Abstract
Common iliac artery (CIA) aneurysms present across a spectrum of anatomic variants that can pose unique operative challenges. A wide variety of procedural approaches have been described in the literature with current therapeutic options including both open and endovascular repair. These techniques may involve either ligation or embolization of the internal iliac artery (IIA) with reliance on collateralized blood flow to the pelvis to mitigate postoperative complications. However, preservation of the IIA is often preferred. This case report describes a hybrid surgical approach for treating CIA aneurysms while preserving IIA perfusion. Our technique mitigates the risks of hypogastric artery dissection (including hypogastric vein injury) in the presence of a large CIA aneurysm.
Keywords
Introduction
First reported by Valentine Mott in 1827, common iliac artery (CIA) aneurysms are described as a dilatation or an abnormal widening of the vessel with any segment reaching a maximal diameter greater than 1.5 cm 1 ; 20% to 40% of these aneurysms are associated with a concurrent abdominal aortic aneurysm. 2,3 Isolated aneurysms of the CIA are much less common having a reported prevalence of approximately 0.4% to 1.9% of all aneurysmal disease. 4
The primary objective in the repair of a CIA aneurysm is twofold. (1) To isolate the aneurysm from the arterial circulation, eliminating arterial wall pressure and (2) to prevent further aneurysmal degeneration and rupture while maintaining lower extremity tissue perfusion. Current guidelines recommend that CIA aneurysms measuring 3.5 cm and greater undergo elective repair in patients with acceptable surgical risk. 5
Two treatment classes have been described for elective CIA aneurysm treatment: open and endovascular. While minimally invasive endovascular repair (ER) is a widely accepted approach for CIA aneurysm treatment, open repair (OR) remains the approach of choice for patients who are anatomically unsuitable for ER and physiologically fit with acceptable life expectancy. Successful OR may help to avoid the: (1) long-term aggregate effects of patient radiation exposure associated with requisite surveillance protocols and (2) potential endograft related complications such as an endoleak. Herein, we report a case of an isolated 48 mm CIA aneurysm treated with a hybrid open/endovascular approach.
Case Presentation
A 63-year-old male presented to an outpatient clinic with an incidental finding of left sided iliac and popliteal artery aneurysms. He was a current smoker with history of hypertension and hypercholesterolemia. His computerize tomography (CT) imaging from an outside hospital demonstrated a left popliteal aneurysm measuring 33 mm as well as a left common iliac aneurysm of 48 mm that extended distally to include the left CIA bifurcation (Figure 1). His left internal iliac artery (IIA) was widely patent and nonaneurysmal.
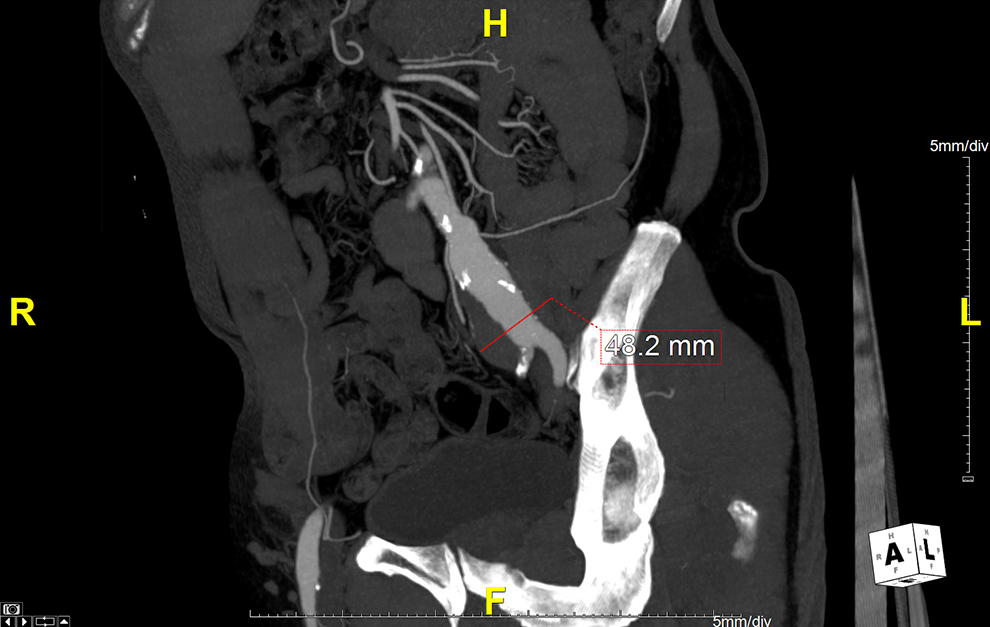
Preoperative CT angiographic image of the common iliac artery aneurysm. CT indicates computerize tomography.
Initial recommendations at outside facilities recommended treatment with an iliac branch endoprosthesis. He was referred to our institution for a third opinion. We opted for an OR with a staged intervention, whereby the popliteal aneurysm was treated first due to its associated pain, size, and risk for distal thromboembolization. After appropriate postoperative recovery from this repair, he returned for the second planned intervention for his left CIA aneurysm. Given his young age, lack of significant comorbidities, anatomic constraints, and desire to minimize the consequences of pelvic ischemia secondary to IIA ligation, the decision was made to pursue open surgical repair with IIA preservation. Informed consent for the publication of this case report as well as the accompanying images was obtained from the patient.
After the induction of general anesthesia, the patient was positioned with his left hip elevated 45 degrees in right lateral decubitus position. He was then prepped and draped in a standardized fashion from the xiphoid process to the knees. With ultrasound guidance, the right common femoral artery was percutaneously accessed utilizing a 4F micropuncture system, and subsequently exchanged to a 7F Flexor Check-Flo (Cook Medical, Bloomington, Indiana). The aortic bifurcation was crossed over and the tip of the sheath was placed into the left CIA. Next, the left IIA was selected using a 0.035 angled Glidewire (Terumo, Somerset, New Jersey) and a 5F Impress Modified Hook catheter (Merit Medical, South Jordan, Utah) and an angiogram was performed. A suitable distal landing zone was identified just proximal to the second order hypogastric branches that provided 2 cm of contiguous seal. Then a 7 mm × 75 mm Viabahn (W. L. Gore & Associates, Flagstaff, Arizona) stent graft was deployed, sized 10% larger than the sealing zone of the distal IIA and post dilated to 7 mm (Figure 2A). A completion angiogram was then performed, confirming intact runoff without evidence of an endoleak.
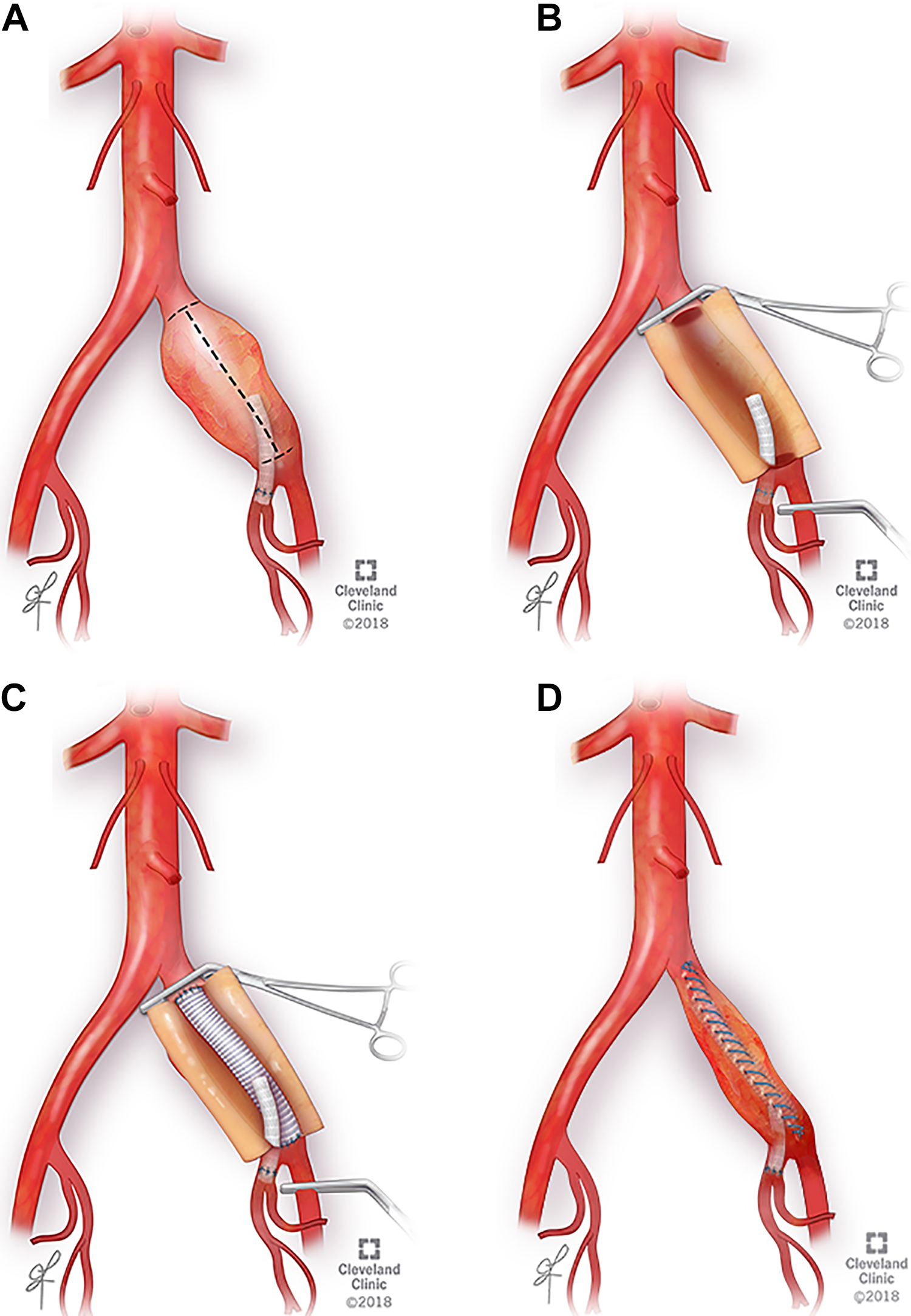
A, Viabahn (W. L. Gore & Associates, Flagstaff, Arizona) covered stent deployed distally within the hypogastric artery and proximally within the common iliac artery aneurysm sac. B, Longitudinal arteriotomy of the left common iliac artery (CIA) aneurysm. C, Illustration of the end-to-end interposition bypass constructed from the left CIA proximally to the left EIA using a 12 mm beveled Dacron tube graft. D. Completed hybrid reconstruction and repair with closure of the aneurysm sac over graft. EIA indicates external iliac artery.
Next, a 10 cm oblique incision was made in the left flank lateral to the rectus sheath. Retroperitoneal space was developed and intra-abdominal organs, left kidney, and the left ureter were retracted cephalomedially with an Omni-Tract (Integra LifeSciences Corporation, Cincinnati, Ohio) self-retaining retractor system to maintain a widely exposed operative field. The patient was then heparinized utilizing an initial 100 units of heparin per kilogram and optimally titrated throughout the case based on the Activated Clotting Time. We then identified and gained control of the left common and left external iliac arteries. A longitudinal arteriotomy was made in the left CIA (Figure 2B). Then, the proximal end of the previously placed hypogastric Viabahn stent graft was identified and easily clamped giving us control of the left hypogastric vessel. We then performed an end-to-end interposition bypass from the left CIA proximally to the left external iliac artery (EIA) using a 12 mm beveled Dacron tube graft (Figure 2C). After reperfusion of the left lower extremity, a side biting clamp was placed on the medial edge of the Dacron graft. The proximal edge of the Viabahn stent graft was then implanted in an end-to-side fashion using a running 6-0 prolene suture without pledgets in order to reconstruct the iliac bifurcation (Figure 3). Several anchor stitches were placed between the stent graft and the proximal native IIA to reinforce the seal zone. Blood flow was then restored to all vessels and hemostasis was confirmed. The aneurysm sac was closed over the graft using a running absorbable suture (Figure 2D). Estimated blood loss was 150 cc. The patient recovered from the procedure without complication and was discharged home on postoperative day 4 on daily Aspirin 81 mg with scheduled outpatient surveillance. Follow up imaging included an arterial duplex and pulse volume recordings at 2 weeks and 12 months which were unremarkable. A CT angiogram was also obtained at 12 months which demonstrated a widely patent CIA graft and IIA stent without evidence of endoleak (Figure 4). Throughout this time the patient remained without complaint of abdominal pain, hip/buttock claudication, or impotence.
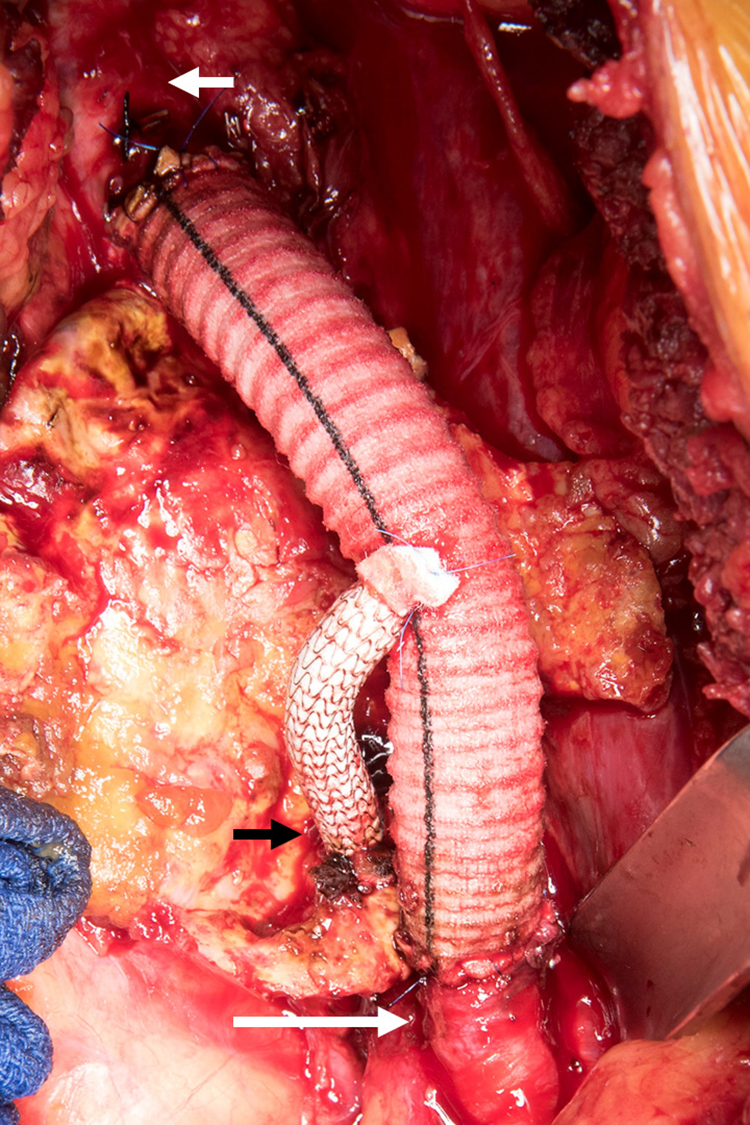
Intraoperative photograph showing graft configuration after reconstruction. Short white arrow: Aorta, Short black arrow: Viabahn graft, Long white arrow: External iliac artery.
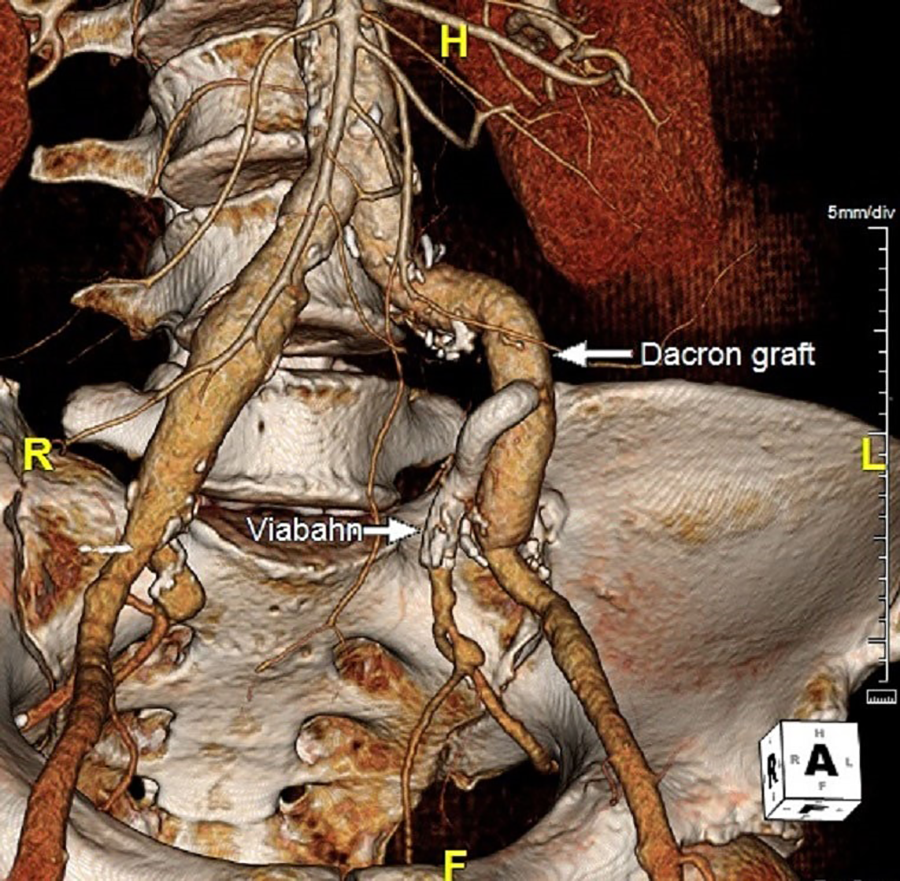
One year follow-up reconstruction CT angiogram imaging demonstrating patency through the CIA graft and IIA covered stent without evidence of endoleak. CIA indicates common iliac artery; CT computerize tomography; IIA, internal iliac artery.
Discussion
Iliac artery aneurysms are commonly asymptomatic and discovered as incidental findings on abdominal and pelvic imaging typically acquired for workup of other pathologies. In describing the management of CIA aneurysms, Sandhu and Pipinos reported that once ruptured, CIA aneurysms have a very poor prognosis with a rate of 28% mortality for emergent repair. However, they found this rate to be significantly reduced to 5% in those patients who underwent elective operative treatment prior to rupture. 6
Common iliac artery aneurysms that extend to or beyond the iliac bifurcation can be particularly challenging to address if pelvic perfusion via the IIA is to be preserved. There are a number of published strategies that can be utilized in this situation, each with its own operative challenges and benefits for patients. The authors identified one other case report describing a similar hybrid repair technique that utilized an endovascular stent graft in the iliac system to repair aneurysmal disease. The technique utilized in those procedures differed with repair through a midline laparotomy incision and the use of bifurcated Dacron grafts to address concomitant aortic as well as CIA and IIA aneurysms, which our patient did not present with. 7
Commonly used ER strategies include coil embolization of the IIA with extension of the endograft into the EIA. While this strategy can effectively exclude a CIA aneurysm, the resultant occlusion of the origin of the IIA can result in a range of complications such as pelvic hypo-perfusion and/or type 2 endoleak. Pelvic hypo-perfusion may clinically present as hip/buttock claudication, colorectal ischemia, sexual dysfunction, and spinal cord ischemia, each greatly impacting the patient’s quality of life. Clinical studies have reported a wide range in the incidence of pelvic ischemia following hypogastric artery embolization from 28% to 55%. 8 However, no highly reliable factors are available to predict those patients who will develop ischemic symptoms. This hypoperfusion can be further exacerbated if the patient requires future aortoiliac intervention that may compromise the contralateral IIA. Therefore, strategies to preserve pelvic blood flow during reconstruction are preferred. More recently, with the advancement of endovascular devices and technologies, CIA aneurysms have been treated with various endovascular approaches such as parallel grafts and reversed flared iliac limbs. 9 There is also increasing use of specialty iliac branched devices (IBD) on the market that obviate the need for hypogastric occlusion.
These devices can be utilized in high operative risk patients who may not be able to tolerate conventional OR. However, endovascular approaches themselves also present challenges such as increased complexity, as well as the risk of late endograft related complications, for example, limb migration, type I and II endoleaks, and graft occlusion. Jongsma et al reported a case series of 140 aneurysms treated with IBD in which more than 10% of CIA aneurysms treated required secondary interventions during follow-up. 10 Cost also continues to be a significant concern. Device pricing may minimize procedural profitability while at the same time introduce higher rates of reintervention. With current ER options on the market, an endovascular approach for the treatment of our patient’s aneurysm would have required treatment of his normal 30 mm aorta as well.
Open repair has long been the standard of care in the treatment of CIA aneurysms. In contrast to endovascular treatment, open approaches have higher rates of in-hospital mortality, perioperative complications, and a longer postoperative hospital length of stay. 11 However, OR demonstrated comparable 1- and 5-year overall mortality with significantly higher freedom from reintervention than ER. 12 However, it may be possible that decreasing exposure to open aortoiliac surgery both in training and in practice may have an impact on a vascular surgeon’s willingness to offer OR when ER options exist. 13
Thus, healthy patients with longer life expectancy would benefit from OR, free from an intensive lifelong surveillance program. The downside of OR includes the relatively difficult exposure of the IIA, especially when situated in the narrow male pelvis. In addition, exposure of the IIA is made more difficult in the presence of a large CIA aneurysm that extends to the CIA bifurcation and obscures visibility of the hypogastric venous complex. This can make conventional open surgical repair technically challenging especially while gaining hypogastric artery exposure and distal arterial control during open reconstruction. Our hybrid approach facilitates IIA control and anastomosis through endovascular placement of a stent while mitigating potential complications from pelvic dissection, but maintaining the advantages of an open surgical repair.
Conclusion
Open surgical repair of CIA aneurysms is technically challenging, especially in patients where maintaining IIA perfusion is preferred. This challenge can be augmented in patients with a narrow pelvis when the origin of the IIA is located in the deep pelvis. Our approach outlines the successful use of a hybrid repair technique in order to preserve hypogastric blood flow in the treatment of a CIA aneurysm. Endovascular placement of a covered stent in the IIA can facilitate safe and effective open CIA aneurysm repair.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.