
Abstract
Nutcracker syndrome is a rare entity in which compression of the left renal vein (LRV), usually by the overlying superior mesenteric artery (SMA), results in renal venous congestion and reflux in the left ovarian vein (LOV). Patients may present with hematuria, left flank pain, dyspareunia, and vaginal or abdominal wall varicose veins. We report a patient with nutcracker syndrome who presented atypically with left flank pain that was exacerbated in the postprandial state. We hypothesize that the physiologic dilation of the SMA after oral intake caused increased LRV compression at that site and augmented lateral LRV distention. The patient had no evidence of SMA syndrome or chronic mesenteric insufficiency. Her symptoms resolved after we performed an LOV to inferior vena cava transposition.
Case Report
A 50-year-old white female who was otherwise healthy was referred by the gastroenterology service and presented with a 4-month history of intermittent left flank pain exacerbated by eating. She reported a 5-pound weight loss during this time, which was attributed to fear of eating. She noted that the postprandial pain was partially relieved by lying in the left lateral decubitus position. The patient denied any history of hematuria, dyspareunia, or abdominal wall or pelvic varicose veins.
Abdominal magnetic resonance imaging showed compression of the left renal vein (LRV) between the superior mesenteric artery (SMA) and aorta as well as a dilated left ovarian vein (LOV) but without SMA compression of the duodenum (Figure 1). An abdominal duplex ultrasound in our accredited noninvasive vascular laboratory confirmed these findings and showed the LRV measured 1.7 mm in diameter between the SMA and aorta and 12 mm laterally (Figure 2). The LOV measured 10 mm in diameter. There was no duodenal compression by the SMA, which was widely patent. Upper endoscopy and upper gastrointestinal series were normal and also confirmed there was no compression of the duodenum by the SMA.
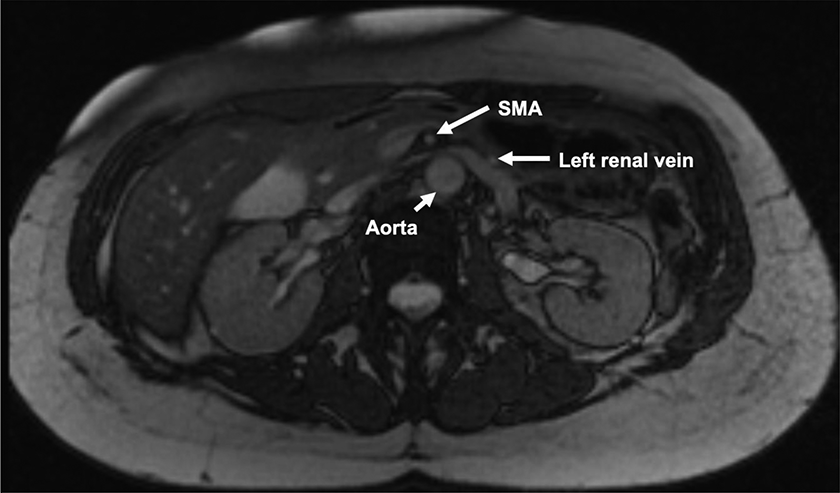
Magnetic resonance imaging showing compression of the LRV by the SMA.
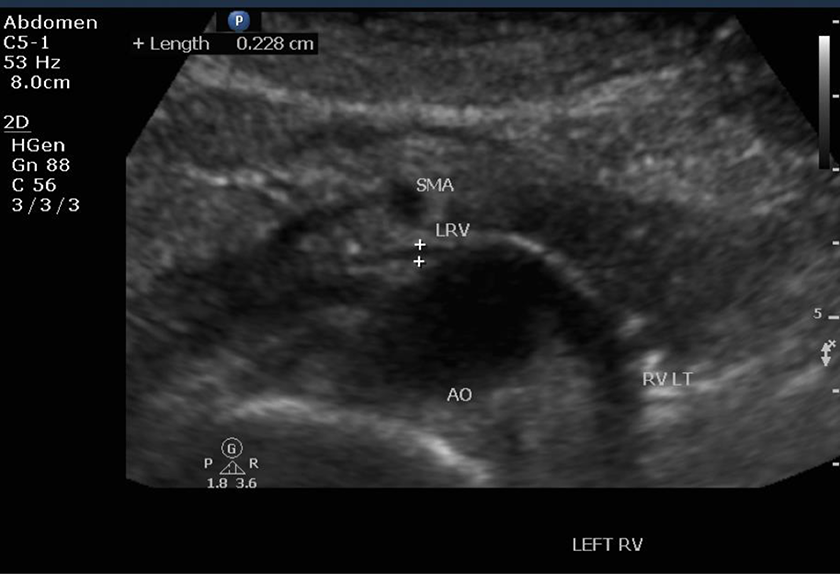
Duplex ultrasound showing compression of the left renal vein by the superior mesenteric artery.
The LOV transposition was recommended as treatment in preference to endovascular or other surgical options. A midline incision was made, the colon was retracted cephalad, and the small bowel was retracted to the right. The LOV was easily identified due to its large diameter and was in normal anatomic position lateral to the inferior mesenteric vein (IMV). The LOV was dissected from the pelvic brim to its confluence with the LRV (Figure 3). The inferior vena cava (IVC) was dissected circumferentially inferior to the renal veins.
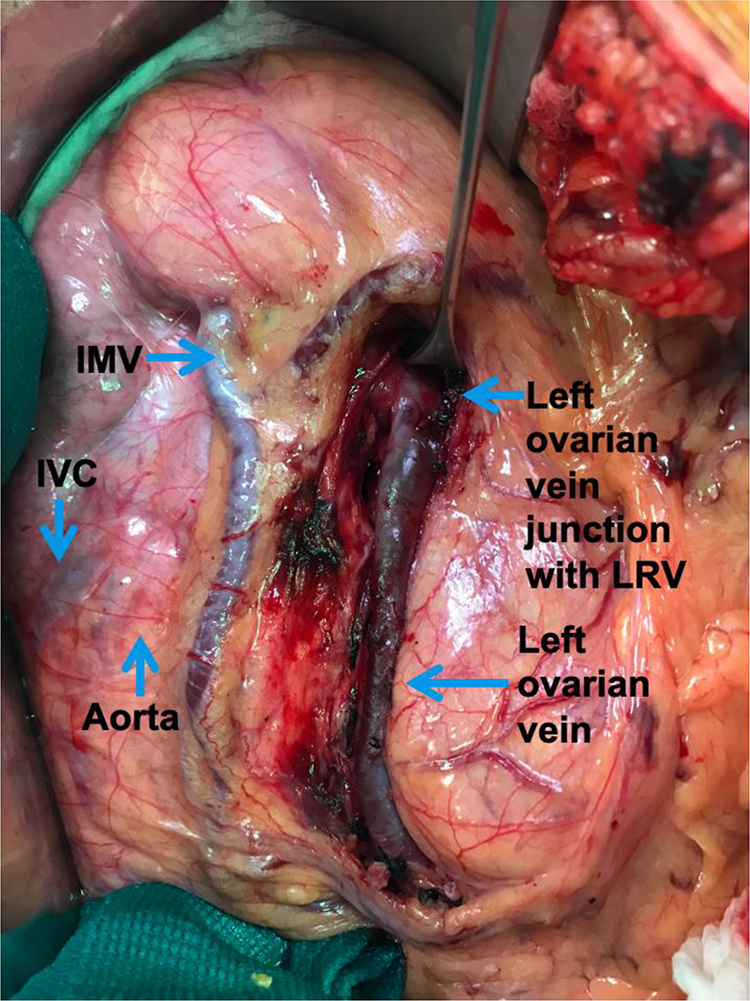
Intraoperative photograph showing the inferior vena cava, inferior mesenteric vein, and left ovarian vein.
The patient was systemically heparinized. The LOV was ligated near the pelvic brim after assuring that its length was adequate for transposition to the IVC. The divided LOV was tunneled posterior to the IMV. A side biting clamp was applied to the IVC. The spatulated end of the LOV was sutured to the IVC as an end-to-side 20-mm-long anastomosis using a running 5-0 Prolene suture (Figure 4). The retroperitoneum was closed over the LOV and the IVC.
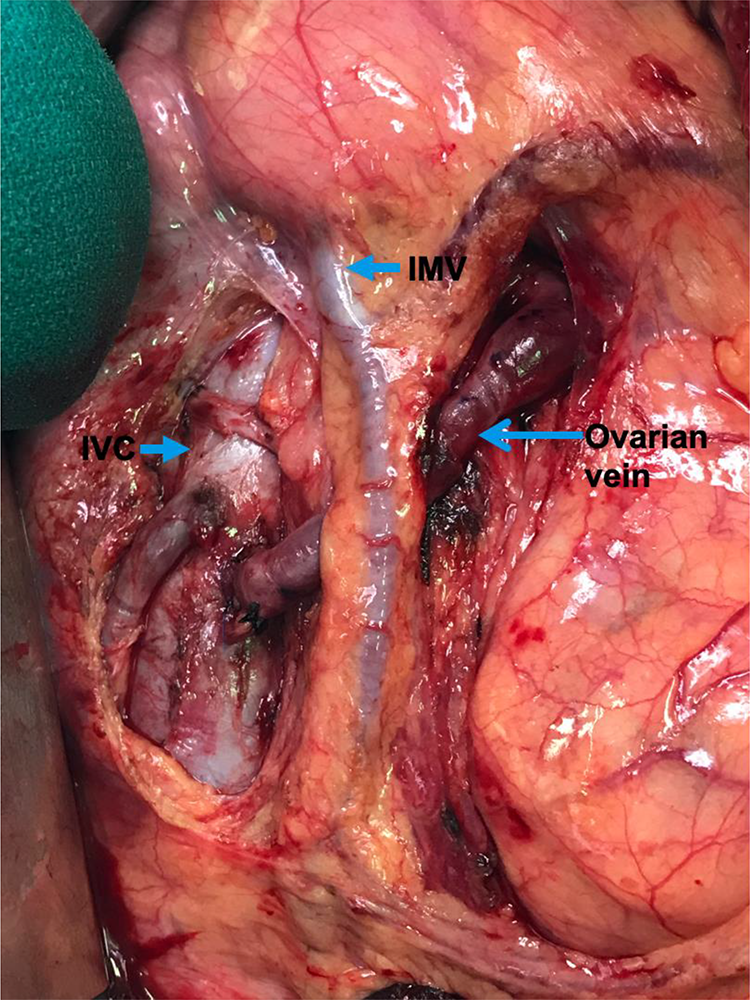
Intraoperative photograph showing the completed left ovarian vein transposition to the inferior vena cava.
The patient had an unremarkable postoperative course and was discharged on the fourth postoperative day. At a 2-week follow-up visit, the patient noted remission of the left flank and postprandial pain. Duplex scan documented flow from the LRV through a widely patent LOV transposition bypass into the IVC. She remained asymptomatic after 6 months of follow-up.
Discussion
Nutcracker syndrome, or compression of the LRV, was first described by Grant in 1937. 1 It is considered a rare diagnosis, although the exact prevalence is unknown. Nutcracker syndrome is differentiated from nutcracker phenomenon in that patients with the syndrome present with clinical symptoms due to compression of the LRV, typically left flank pain and hematuria, whereas nutcracker phenomenon is a radiographic finding in an asymptomatic patient. The most common anatomic conformation of nutcracker syndrome is termed an anterior nutcracker in which the LRV is compressed between the SMA and aorta. In contrast to this, a posterior nutcracker is caused by compression of a retroaortic or circumaortic renal vein between the aorta and vertebral body.
An anterior nutcracker syndrome can rarely occur concomitantly with SMA syndrome, in which the SMA compresses the duodenum causing postprandial pain, early satiety, nausea, vomiting, and weight loss. 2 -4 More commonly, patients with SMA syndrome may also have nutcracker phenomenon where the LRV is compressed but without symptoms. 5 -8
We suspect that physiologic dilation of the SMA after oral intake caused further compression of the LRV and hence a worsening of the patient’s left flank pain in the postprandial state. Her pain was improved by lying in the left lateral decubitus position, possibly increasing the angle between the SMA and the aorta and thereby decompressing the LRV. Resolution of symptoms after LOV transposition lends credence to this theory. To our knowledge, there are no similar case reports to date.
A variety of surgical approaches have been used to treat nutcracker syndrome. These include LRV bypass with PTFE, Dacron or saphenous vein graft, LRV transposition, medial nephropexy with excision of renal varicosities, SMA transposition, renal autotransplantation, gonadocaval bypass, nephrectomy, and wrapping the LRV with ringed PTFE. An endovascular surgical approach was not offered for concern of possible stent migration and/or in-stent stenosis requiring repeated intervention. 9 We chose LOV transposition to the IVC as our surgical approach because it is effective, durable, and simple in execution and has limited morbidity as compared to other treatment options. 10
Footnotes
Authors’ Note
Informed consent was not obtained for this case report as the patient information has been de-identified.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.