
Abstract
Background and Aims:
The management of persistent type II endoleaks (T2E) is often problematic for the endovascular specialist, with a lack of clear evidence for the best approach for embolization. The aim of this study was to evaluate the safety and efficacy of translumbar embolization (TLE) for T2E following endovascular aneurysm repair (EVAR).
Methods:
This retrospective review included 27 embolizations performed on 23 patients with a median age of 78 (range 67-94 years; male: female 15:9), during the period September 2006 to July 2018. Primary outcome was freedom from aneurysm sac growth defined as <2 mm sac diameter increase on subsequent computed tomography.
Results:
The initial technical success rate was 100%, with complete “on table” embolization of the T2E on fluoroscopy; however, 4 (15%) patients needed repeat TLE due to persistent endoleak identified on follow-up computed tomography or because of further sac expansion. Satisfactory stasis was achieved in these 4 cases following a second embolization. The mean volume of embolic injected was 7.4 mL per case. Feeding vessels were identified on angiography in all cases; the nidus was supplied by lumbar branches in 21 cases, by the inferior mesenteric artery in 1 case and by both in a further 5 cases. Freedom from aneurysm sac growth (defined as < 2 mm) following 1 or 2 separate TLE was achieved in 18 (78%) and 20 (86%) patients, respectively. The major complication rate was <5% with one case of psoas abscess presenting 7 months following embolization; there were 2 minor complications in the form of intraprocedural transient abdominal pain.
Conclusion:
The translumbar approach is a safe and effective technique to treat T2E, as evidenced by the low complication and reintervention rate.
Keywords
Introduction
A type II endoleak (T2E) is defined as persistent perfusion of an aneurysm sac following endovascular abdominal aortic aneurysm repair (EVAR), caused by retrograde flow via collateral arteries. The inferior mesenteric artery (IMA) and lumbar arteries are the most commonly implicated vessels. This can lead to continued pressurization and subsequent growth of the aneurysm sac, which carries a risk of rupture.
Type II endoleak represents the commonest complication of EVAR. The largest published series, from the EUROSTAR registry (European collaborators on stent/graft techniques for aortic aneurysm repair) reported T2E incidence at 9% at any point postoperatively. 1 Although the natural history of this process is not well understood, it has been demonstrated that more than 50% of T2E resolve spontaneously. 2,3 The clear majority of these can therefore be safely managed conservatively with serial imaging. Treatment should be reserved for persistent cases (>6 months) and patients with more than 5 mm of sac expansion, when compared to preprocedural computed tomography (CT) scan measurements. 4,5 Persistent T2E is associated with adverse outcomes such as significant sac size increase, subsequent conversion to open repair, reintervention, and rupture. 4,6
Much debate has focused on the optimal approach for embolization with transarterial, transcaval, translumbar, and more recently transabdominal techniques described. 7,8 There is a lack of clear evidence in favor of any of these techniques. Low numbers, reflective of the low incidence of these persistent leaks, has blighted these studies. Despite the relatively low incidence these cases can prove to be very challenging and often require multiple rounds of treatment.
The translumbar technique has been previously described, with some evidence to suggest better outcomes when compared to transarterial embolization (TAE) of feeding vessel. 9 The aim of this retrospective study was to assess the safety and efficacy of the percutaneous translumbar technique of embolizing T2E, with a focus on subsequent sac sizes and clinical outcomes at our regional vascular center; adding to the small body of existing evidence.
Method
Patients with previous EVAR, who were diagnosed with T2E, were identified from our local hospital database between 2006 and 2018. From this cohort, we were then able to identify patients who went on to have T2E treated. Transarterial embolization remained the first choice treatment for relevant T2E at our institutions. During the later years, we adopted obliteration of nidus rather than just the feeding vessel. After exclusion of patients with T2E treated with TAE, we identified patients who had translumbar embolization (TLE) of T2E. We collected relevant patient demographic, preprocedural, procedural, and postprocedural data using our hospital radiology information system. Data were collated and analyzed using Microsoft Office Excel 2016.
Follow-Up Protocol Following EVAR
Following standard EVAR, patients underwent CT angiography (CTA) and plain film at 1 month to identify potential technical issues followed by a further CT at 3 months to assess sac size. If there were no adverse findings, the patient would go on to have routine annual plain film and duplex follow-up. All cases of demonstrated T2E were discussed at our vascular multidisciplinary meeting and a decision made regarding the merits of further interval imaging or treatment. Embolization was considered in patients with persistent T2E (>6 months) and significant sac growth (>5 mm). Multiplanar reconstructions was used to assess the most appropriate approach for embolization, favoring a transfemoral approach initially if technically possible. In the absence of favorable anatomy, or where a transfemoral approach had failed, a TLE was performed.
Procedure
Given that these procedures were performed over a period of 12 years the technique had evolved somewhat and some of the equipment substituted, although the principles described have not changed. The most current protocol is described herein. All TLE were performed under a general anesthetic in the prone position. All patients were given intravenous Co-amoxiclav and Gentamycin antibiotic prophylaxis on induction. XperCT technology (Phillips Medical, Amsterdam, the Netherlands) was used for needle tracking and placement. A left (occasionally right) paraspinal entry point was chosen and a predetermined radiopaque reference point (such as a bony landmark, sac calcification, or graft markers) was used to determine the target point in the endoleak cavity. An 18G-long needle was used to puncture the sac under XperGuide fluoroscopy (Figure 1). Pulsatile backflow was watched for, on removal of the needle inner stylet confirming correct needle placement within the endoleak nidus. An 8F hemostatic valve is fitted to the trocar needle and angiography was performed, detailing the endoleak cavity and feeding/draining vessels. A 4F dilator was used to open the hemostatic valve and a Progreat co-axial microcatheter (Terumo, Tokyo, Japan) was passed via the dilator and puncture needle and used to direct embolization. If manageable in a timely manner, the feeding/draining vessels were cannulated and embolized with microcoils, this was not always possible largely due to the inability to use large directional catheters. The endoleak nidus was then embolized with Onyx 34L (Medtronic, Dublin, Ireland), often with reflux into feeding vessels. Static Onyx within the endoleak cavity (ideally with lumbar arterial reflux) was taken as an end point. A noncontrast CT was performed before discharge to exclude retroperitoneal hemorrhage, assess Onyx distribution, and document sac size. Further follow-up by means of CT angiography was performed at 3 and 6 months, if possible. Once sac stability was achieved, annual follow-up with plain film and duplex was resumed.
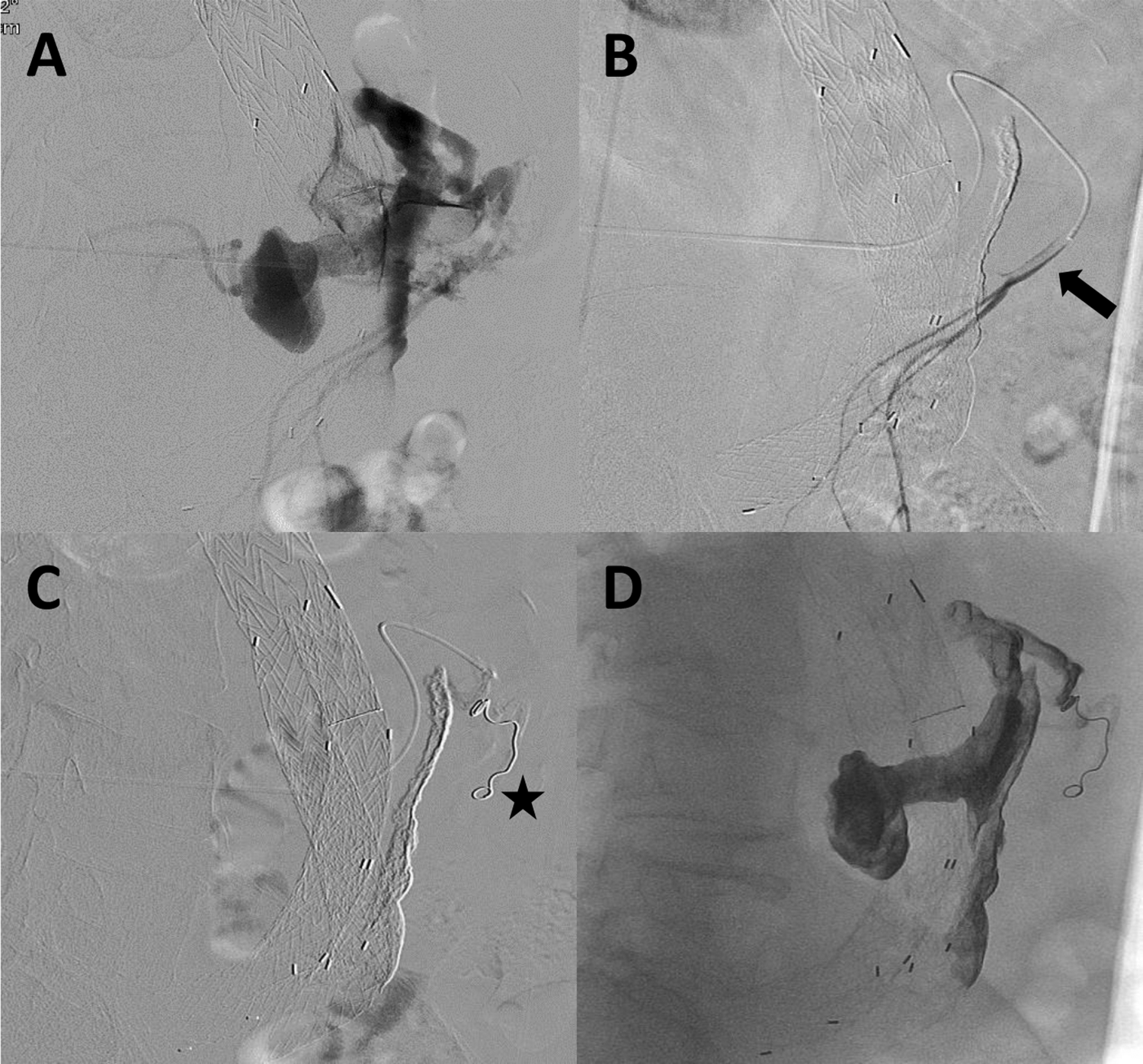
Image A represents a DSA image of an endoleak cavity performed via an 18-gauge trocar needle. Note the reflux into the IMA and lumbar vessels. Image B demonstrates a selective angiogram of the IMA (arrow) cannulated with a Progreat co-axial microcatheter. Image C demonstrates a coil within the IMA (star). Onyx is then injected into the IMA stump and the catheter withdrawn to fill the endoleak cavity/nidus until a typical end point is reached (see Image D). IMA indicates inferior mesenteric artery.
Results
Twenty-seven TLE were performed in 23 patients with a median age of 78 years (range 67-94 years; male: female 15:9) during the period September 2006 to July 2018. There were 17 GORE excluder grafts, 2 Anaconda grafts, 2 COOK Zenith grafts, and 2 “unknown” grafts placed out of region. All aneurysms were infrarenal in morphology, including 1 case, which had previously undergone exclusion of an iliac aneurysm prior to EVAR.
Median time to first endoleak diagnosis was 34.5 days (0-1827 days) following graft placement. These data were unavailable for 1 patient. Only 1 case had a demonstrable endoleak “on table” at time of initial procedure. Eleven (47%) patients had previously undergone an attempt at TAE, which was either abandoned due to vessel tortuosity or was not successful in abolishing the endoleak.
The initial technical success rate was 100%, with complete “on table” embolization of the endoleak on fluoroscopy; however, 4 (15%) patients needed repeat TLE due to persistent endoleak identified on follow-up CT or because of further sac expansion. Satisfactory stasis of sac growth was achieved in those 4 patients following a second embolization.
The choice of embolic material is highlighted in Table 1. There was a trend toward Lipiodol/Histoacryl glue (Guerbet, Solihull, United Kingdom) use early in the series, followed by a more recent shift toward Onyx 34L (Medtronic). The mean volume of embolic injected was 7.4 mL per case. Feeding vessels were identified on angiography in all cases; the nidus was supplied by lumbar branches in 21 cases, by the IMA in 1 case and by both in a further 5 cases (Table 1).
Technical and Procedural Parameters.a
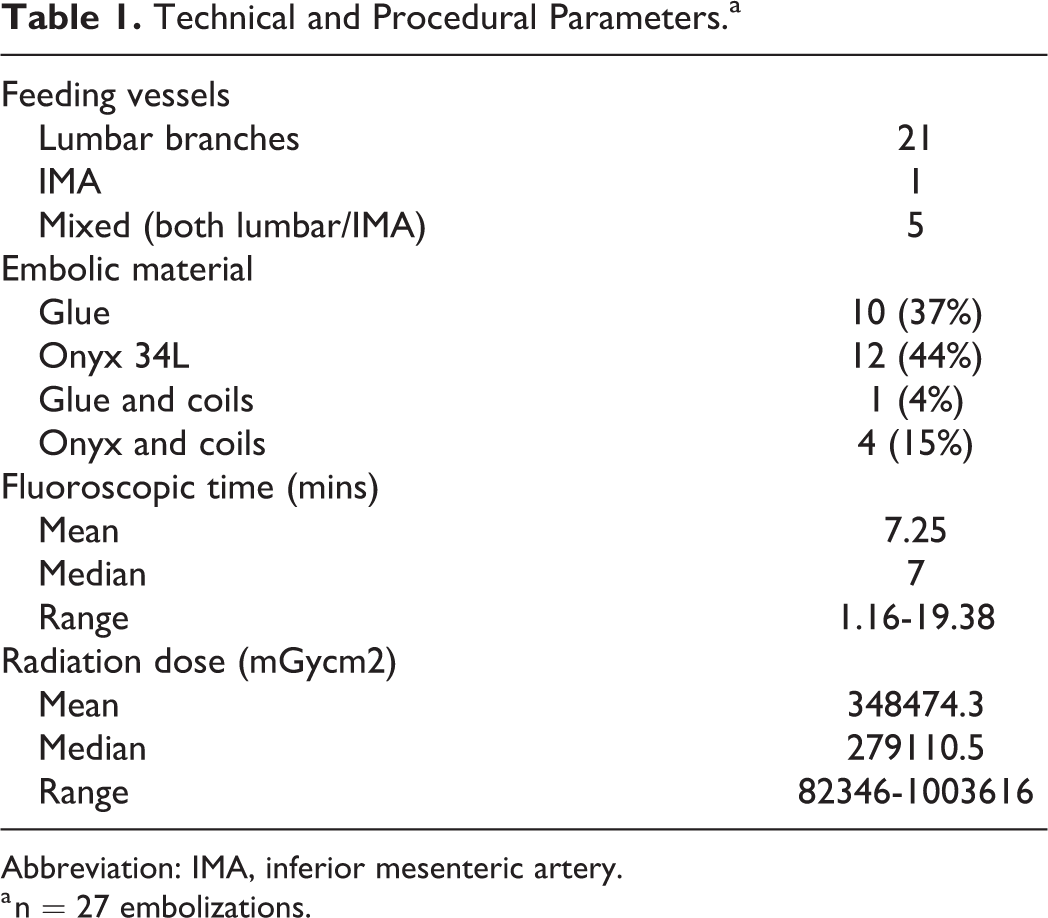
Abbreviation: IMA, inferior mesenteric artery.
a n = 27 embolizations.
There were no significant immediate complications. Two patients experienced intraprocedural transient abdominal pain, which was managed conservatively. There was 1 case of left psoas abscess and sac infection in a 90-year old detected 7 months after left translumbar Onyx embolization. The patient had not received prophylactic antibiotics. The patient was able to return home on long-term oral antibiotics, without requiring further intervention.
Freedom from aneurysm growth (defined as <2 mm sac size increase) following 1 or 2 separate TLE was achieved in 18 (78%) and 20 (86%) patients, respectively. All patients had <5 mm sac size increase following 1 or 2 separate embolizations. The median cross-sectional follow-up period was 220 days (31-960 days), with 83% of patients having had a minimum of 3 months of follow-up at time of writing (follow-up data highlighted in Table 2).
Patient Sac Size Changes and CT Follow-Up.a
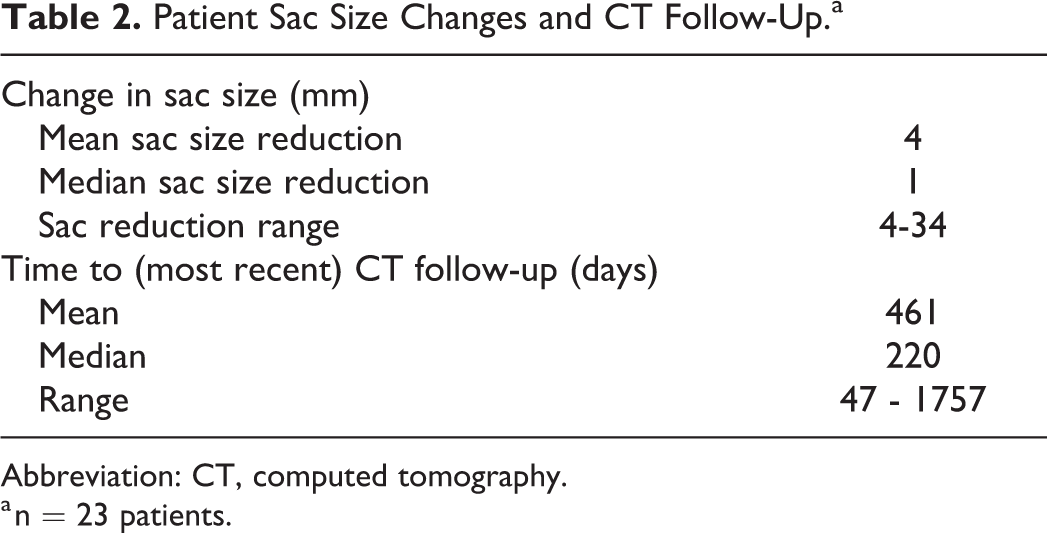
Abbreviation: CT, computed tomography.
a n = 23 patients.
One patient treated with EVAR in October 2013 underwent TLE at 3 and 6 months before achieving freedom from further sac growth. There was good proximal seal on pretreatment CTA, with a visible T2E. He represented with symptoms 9 months following initial treatment and was found to have developed a large type 1A endoleak. The patient declined further treatment and died the following day.
A second patient was treated with TLE using histoacryl glue, 19 months following initial EVAR. The patient represented with a large left sided type 1B endoleak, 13 months following embolization. The type 1B endoleak was successfully treated with limb extension of the stent graft. Ten months later, the patient presented again with a right type 3 endoleak due to limb dislocation (rather than fabric tear, which is a recognized complication of direct sac puncture). The limb was relined, and the aneurysm restabilized. There were no suspicions of occult type 1 endoleaks in the aforementioned cases on high-quality CTA, it is however possible that sac expansion as a result of T2E led to the development of type 1 leaks.
Discussion
In our experience, the translumbar approach is a safe means of treating T2E; with only 2 cases of transient abdominal pain and one case of psoas abscess and sac infection during the study period. Following the psoas abscess complication, a review of antibiotic prophylaxis was conducted, and a new protocol was devised. Significant complications have been encountered employing the translumbar technique in other studies. In the largest published series (n = 62), Stavropoulos et al described an IMA branch nontarget embolization requiring a partial colectomy as well as a retroperitoneal hemorrhage requiring transfusion. Other complications described include graft fabric puncture and pulmonary embolism. 10,11
The mean fluoroscopic time of 7 minutes achieved in this study is short and the associated fluoroscopic doses low; an important factor in the management of patients requiring long-term follow-up and accumulating large lifetime cumulative doses.
There were no technical “on table” failures in this series, with complete on table embolization achieved in all cases. Freedom from aneurysm growth, defined as a static sac (<2 mm), was achieved following 1 or 2 separate TLE in 18 (78%) and 20 (86%) patients, respectively. These results are promising in comparison to other published series reporting primary success rates of 50% to 92%, 9 -12 especially in light of some studies accepting ≤5 mm sac increase on follow-up, with other studies not providing clear definitions of sac size increase. The rigorous measuring criteria utilized in this study was possible due to all follow-ups being reviewed by 2 vascular radiologists, thus minimizing interobserver error.
Three of the patients requiring a repeat TLE (4 in total) were initially treated early in the series. In fact, 2 of those represent the first and second TLE performed at our center. There are 2 possible explanations for this, the first being operator “learning curve.” The second possible explanation is recent shift to using Onyx as the liquid embolic of choice. We prefer Onyx to glue; in our experience, it facilitates better control of embolization and a more permanent outcome. We have experienced Lipiodol resorption and endoleak recurrence especially where low histoacryl:lipiodol ratios were used.
Our center employs a “transarterial first” approach to T2E management in anatomically favorable cases. Forty-seven percent of our cases had previously undergone an attempt at TAE. Direct comparison of the 2 techniques is therefore not possible. Attempts have been made to compare the 2 approaches; Stavropoulos et al compared a modified transarterial technique which also involved coil embolization of the nidus (n = 18) with the translumbar technique (n = 45) and failed to demonstrate a significant difference in clinical outcomes with an overall success rate of 78% and 72%, respectively. 11
The transcaval (TC) method of embolization has been well described. 8,13,14 Mansueto et al studied the efficacy of a TC approach performed via a transfemoral or transjugular approach, with a curved guiding cannula and a flexible puncture needle for access. 8 Embolization was performed using a combination of thrombin and coils. On table, success was achieved in 11 of 12 patients, with sac stasis achieved in 10 of 12 patients at 1 year. There was 1 case of common femoral vein thrombophlebitis treated medically. A larger series by Giles et al described 29 TC coil embolizations in 26 patients, with 47% having previously undergone other modes of embolization. Regression or stasis of sac measurements was achieved in 70% of patients with mean follow-up period of 16.5 months. No major complications were reported although the reintervention rate was high (5 of 26 patients). Interestingly, there were no cases of aortocaval fistulae reported in the literature; however, this is a theoretical risk of the TC technique. The author concluded that the TC approach is a useful alternative when anatomy makes other approaches difficult.
A recent retrospective study by Zener et al studied the efficacy of a transabdomial approach to T2E embolization. Thirty patients were treated with 33 direct sac punctures. Embolization methods included coils, glue, and Onyx. Technical success was quoted as 97% with freedom from sac growth in 85% after ≥1 embolizations (mean follow-up 15 months). There were 2 cases of rectus sheath hematoma and 1 case of self-limiting neuropraxia as a result of a psoas injury. Interestingly, the technical success rate was not quoted on an “Intention to Treat” basis with 13 patients excluded due to not having unobstructed access, with interposing bowel on preprocedure ultrasound. This transabdominal approach may prove to have an advantage for treating “anterior” endoleaks, where other access would be difficult.
Despite these promising results, we have maintained a “transarterial first” approach, particularly in the context of favorable anatomy. This is largely based on logistical factors, negating the need for patient admission and avoiding what would often be a high-risk general anesthetic. It is interesting to note that 11 patients underwent successful TLE, having previously failed a transarterial attempt. The cause of this may be multifactorial; however, our results support the theory that embolizing the endoleak nidus (with liquid embolics such as Onyx) has a treatment benefit. The hypothesis that T2E are morphologically similar to arteriovenous malformations has been previously suggested 9,11,15,16 ; nidus embolization interrupting flow to all aortic side branches seems more likely to abolish the leak than targeting individual feeding or draining vessels. Our results support this theory, which is likely to be relevant regardless of the approach for embolization. Careful patient selection is paramount when performing embolization of T2E, with treatment reserved for those with persistent leaks and significant sac increases.
Limitations
This study is limited by its retrospective nature and relatively long inclusion period. The number of patients included is small but larger than comparable published series. Aspects of the procedure have evolved over time, with improvements in equipment, technique, and protocol; however, the principles have remained the same.
Conclusion
The translumbar approach is a safe and effective technique for treating type 2 endoleaks, as evidenced by the low complication and reintervention rate. There is little evidence to support the superiority of a particular approach, each having its advantages and disadvantages; clinical decisions should be made on a case-by-case basis. With relatively small numbers of procedures performed, even in high volume centers, a multicenter prospective study may be necessary to conclusively determine the best method of embolization.
Footnotes
Authors’ Note
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. For this type of study (retrospective), formal consent is not required. The local Hospital Ethical committee was approached (Queen Elizabeth Hospital, Birmingham, United Kingdom) and ethical approval was waived due to the observational nature of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.