
Abstract
Objective:
The attempt to repair a ruptured abdominal aortic aneurysm carries a significant risk of perioperative mortality. The relationship between body mass index (BMI) and outcomes after repair of ruptured abdominal aortic aneurysms (AAAs) has not been well defined. We report the association of BMI with outcomes after ruptured AAA repair.
Methods:
Patients undergoing ruptured AAA repairs between 2008 and 2017 at 2 tertiary academic centers were included in this retrospective study. Demographics (including BMI), type of repair, length of stay, and admission mortality risk scores were gathered and analyzed using bivariate and multivariate logistic regressions. Adjusted odds ratio (AOR) was reported with 95% CIs and P values from the multivariate analysis. The primary outcome was 30-day mortality. Akaike information criterion (AIC) and c-statistics were used to assess the predictive power of models including physiologic score with or without BMI.
Results:
A total of 202 patients underwent repair of ruptured AAA. In bivariate relationship, increased BMI was significantly associated with 30-day mortality. With multivariate analysis, adjusting for demographics, type of procedure, and physiologic score, for each kg/m2 increase in BMI, an 8% increase in the likelihood of perioperative mortality (AOR = 1.08, 95% CI: 1.01-1.17; P = .04) was observed.
Conclusion:
When adjusted for admission risk score, type of procedure, and demographics, obesity was associated with increased 30-day mortality. With BMI as an additional data point, the c-statistics and AIC comparisons indicated that we would have a greater ability to preoperatively estimate mortality after ruptured AAA repair. Consideration could be made to include BMI in future mortality risk scoring systems for ruptured AAA.
Introduction
Despite the implementation of aggressive screening for at-risk patients, ruptured abdominal aortic aneurysms (rAAAs) are still very much a part of the vascular surgical practice. The decision to treat these patients is still associated with overwhelming risks, even with contemporary surgical treatments. Current Society for Vascular Surgery (SVS) guidelines indicate the need for further refining the perioperative mortality scoring systems and also to enhance their predicting ability. 1 Some previous publications have suggested the presence of an association of perioperative mortality and BMI in the setting of elective AAA repair. 2,3 However, this association, if present, has not been defined in the emergency repair of ruptured aortic aneurysms. It also remains to be studied if there are gender-based differences affecting the mortality in patients with similar body mass indices (BMIs).
There are many risk scoring systems that are available to assist in the prediction of perioperative mortality of rAAAs. These scoring systems may help with guiding decisions to operate, as well as perioperative management by identifying those at highest risk of morbidity and mortality. They include the Glasgow aneurysm, 4 Vascular Study Group of New England (VSGNE), 5 Hardman index, 6 Vancouver, 7 and Edinburgh ruptured aneurysm scores. 8 These risk scores, however, do not take into account BMI. Therefore, the objective of the present study is to identify the relationship, if any, between BMI and 30-day mortality after rAAA repair.
Methods
This was a retrospective study performed within the guidelines specified by the latest iteration of the Declaration of Helsinki after expedited review approval from Indiana University Institutional Review Board (IRB approval 1704207547). 9 All consecutive patients with rAAAs who underwent surgical repair from November 2009 to November 2017 at Indiana University Health Methodist Hospital in Indianapolis, Indiana, and from August 2008 to December 2015 at the University of Wisconsin Hospital at Madison, Wisconsin, were eligible for inclusion. Both hospitals are part of tertiary academic referral centers with high-volume complex vascular surgical caseloads. Additionally, both institutions have protocols in place for expediting the care of patients with rAAAs, for example, streamlined transportation and immediate access to the operating room with array of endovascular inventory for emergent repair of ruptured aortic aneurysms.
All patients had preoperative imaging either by computed tomography or by magnetic resonance. Those included in the study were found to have rAAAs either on preoperative imaging or confirmed intraoperatively. Excluded were patients whom we were unable to obtain all the relevant data points, those who presented to the hospital but died before undergoing definitive therapy, those who had prior aortic repair, and those who had aortic emergencies other than that due to aneurysm rupture.
Patient demographics, BMI, comorbidities, type of repair (endovascular or open), length of stay (LOS), total blood products transfused, variables needed for calculation of the Glasgow aneurysm and VSGNE score, and 30-day mortality were collected. The Glasgow aneurysm score variables are age, presence of shock, myocardial disease, cerebrovascular disease, and renal disease. 4 The VSGNE score variables are age greater than 76 years, presence of cardiac arrest, loss of consciousness, and need for suprarenal clamp. 5 Because the VSGNE study studied only open repairs and this study included endovascular repairs, the definition of “suprarenal clamp” in this study was broadened to include those that required balloon occlusion during endovascular repair.
For the statistical analysis, all categorical variables (gender, type of repair, and categorized BMI) were summarized into proportions, whereas continuous variables (age, total blood products transfused, Glasgow aneurysm, and VSGNE score) were summarized as means (with SD) or median (with interquartile range [IQR]). Body mass index categories were determined by standard definitions originated by the World Health Organization 10 : normal is defined as BMI between 18.5 and 25 kg/m2, overweight is between 25 and 30 kg/m2, and obese is greater than 30 kg/m2. Bivariate Pearson χ2 and Fisher exact tests, as appropriate, were used to examine the relationship between 30-day mortality and each of the categorical variables, while Student t tests for normally distributed variables and Wilcoxon rank sum tests for skewed variables were performed to examine the bivariate relationship between 30-day mortality and each of the continuous variables. Shapiro-Wilk test was conducted to assess normality of all continuous variables. Relationship of the mortality outcome with BMI, our main variable of interest, was analyzed treating BMI as a categorical as well as continuous variable. We used generalized linear model 11 (GENMOD) with logit link function to perform a multivariable logistic regression with 30-day mortality. Robust standard errors 12 were requested in GENMOD procedure by treating each observation to be independent and within its own cluster and by using INDEPENDENT correlation structure and REPEATED statement. All variables that were significant at .25 levels in bivariate analysis were included in the multivariable model. We also included age in the multivariable model as older age is a known confounder for mortality. Our final multivariable model included BMI, physiologic scores, age, gender, type of procedure (endo vs open), and health facility. In addition, we also tested for the presence of any multicollinearity in the model using tolerance and variance inflation factor. 13 We examined the model fit with or without BMI to predict mortality using Akaike information criterion (AIC) and c-statistics. Model with lower AIC and higher c-statistics was chosen as the favorable model, 14,15 with better predictive ability to preoperatively estimate mortality after rAAA repair. Adjusted odds ratio with 95% CIs and P values were reported for each predictor. Data analysis was performed using SAS 9.4.
Results
Within the prespecified study period, 202 patients underwent repair of their rAAAs at our institutions, 109 (54.8%) by open repair and 90 (45.2%) by endovascular repair. Three patients had endovascular converted to open repair (1.5%). Forty-seven patients (23.3%) died within 30 days of their intervention. On bivariate analysis, no significant differences in age (P = .47), gender (P = .13), type of procedure (P = .25), BMI as continuous variable (P = .06), and BMI as categories (P = .24) were found between those who survived and those who died. However, there were significant differences in hospital LOS (P < .01), total blood products (P < .01), and Glasgow aneurysm (P < .01) between those who survived and those who died. The Glasgow aneurysm 4 was calculated by previously published scoring systems. The median hospital LOS was significantly different (P < .01) between those who survived (8 days, IQR = 10 days) and those who died (1 day, IQR = 6 days). Those who died compared to those who survived had a median BMI of 32 and 29 kg/m2, respectively (P = .06). The Glasgow aneurysm score of those who survived was 83.0 compared to 93.8 in those who died (P < .01; Table 1).
Patient Characteristics with Ruptured Abdominal Aortic Aneurysm.
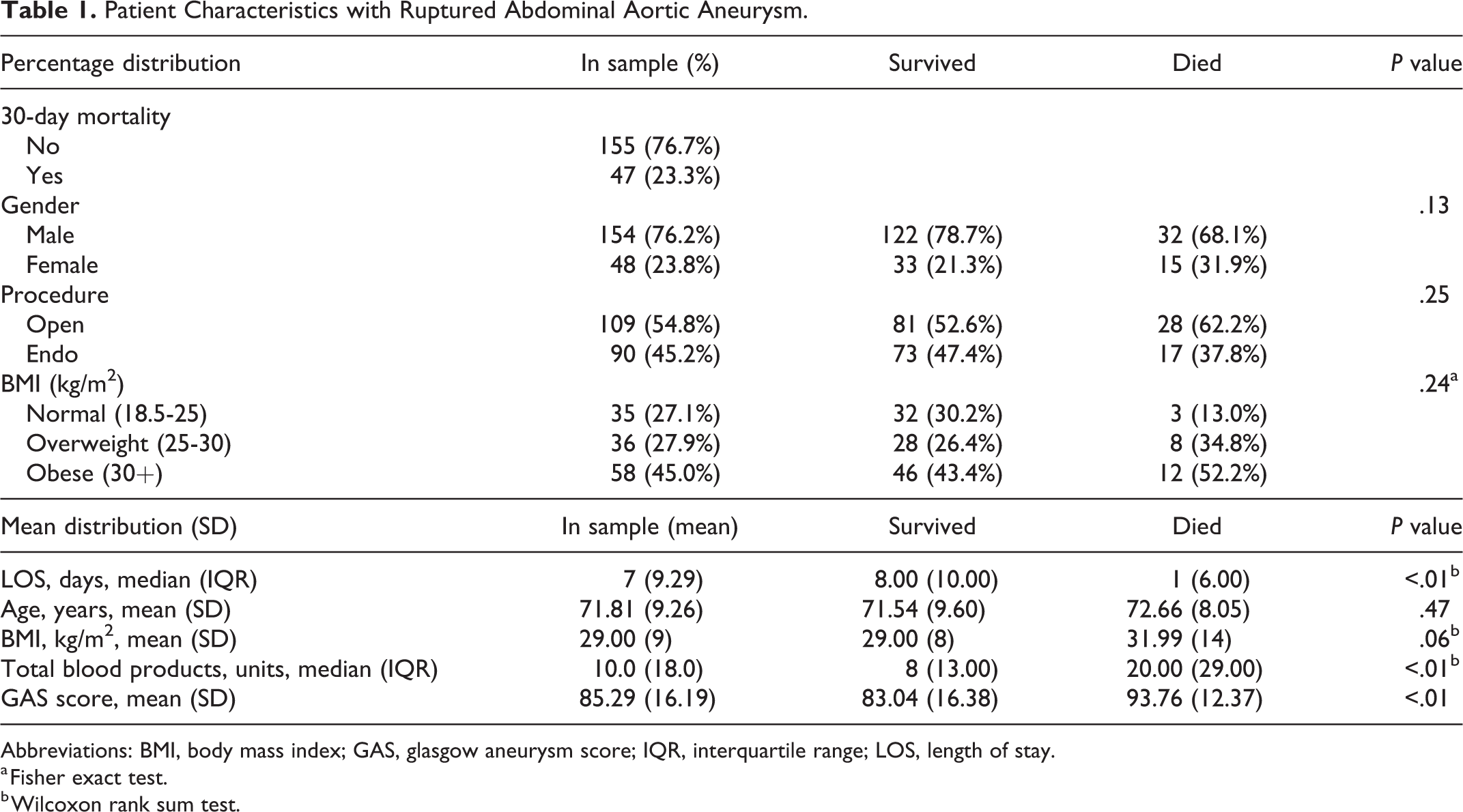
Abbreviations: BMI, body mass index; GAS, glasgow aneurysm score; IQR, interquartile range; LOS, length of stay.
a Fisher exact test.
b Wilcoxon rank sum test.
In multivariable analysis, the odds of 30-day mortality in patients undergoing repair of rAAA increased significantly by 1.08 for every 1 kg/m2 increase in BMI (95% CI, 1.01-1.17; P = .04). This translates to 2.16 higher odds of 30-day mortality for every 10 kg/m2 increase in BMI. In addition, odds of 30-day mortality significantly increased by 1.06 for every integer increase in Glasgow aneurysm score (95% CI, 1.02-1.10; P < .01). Age, type of repair, gender, and academic center did not significantly affect the odds of 30-day mortality (Figure 1). We also analyzed the prediction ability of models including physiologic scores with or without BMI. The c-statistics was higher and AIC was lower for the multivariable model, with BMI indicating greater ability to preoperatively estimate mortality after rAAA repair compared to the physiologic score without BMI in the model (Figure 2).
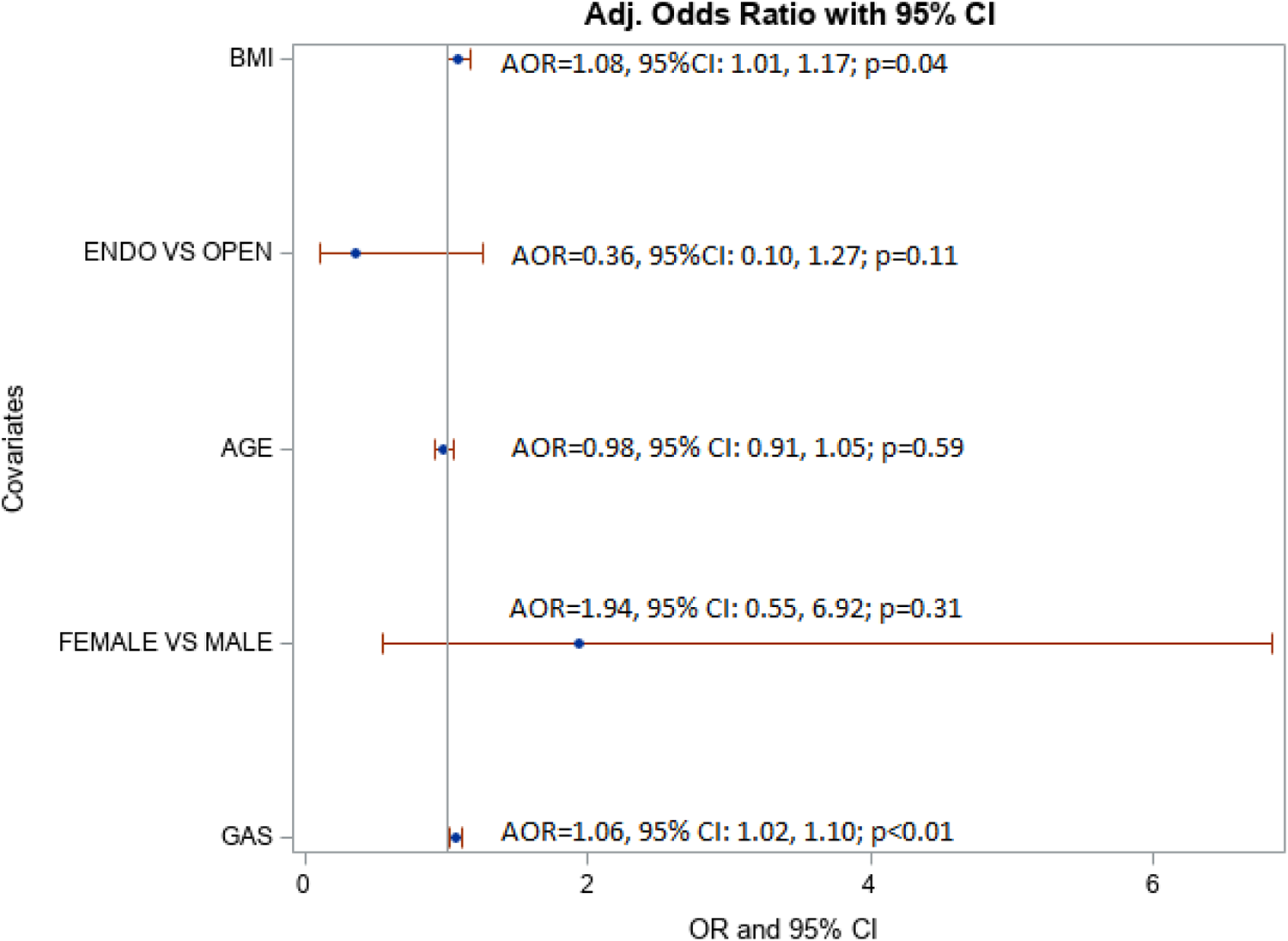
Multivariable model with variables predicting 30-day mortality in patients undergoing ruptured abdominal aortic aneurysm (rAAA) repair.
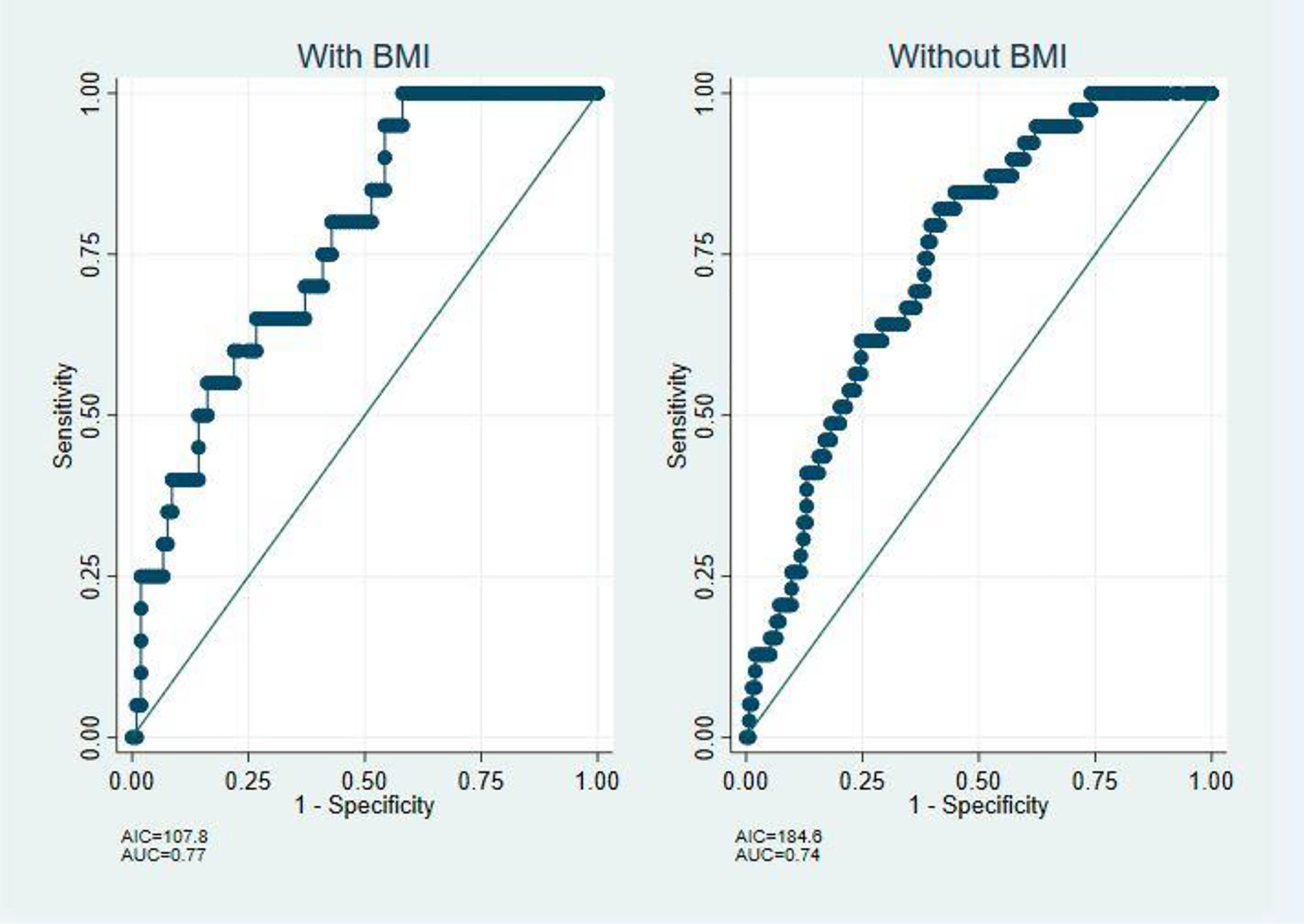
Model using body mass index (BMI) to predict mortality using Akaike information criterion (AIC) and c-statistics.
The BMI which was not significant in bivariate analysis turned out to be significant in the multivariable model and this could be because of controlling for confounders .The error variance from BMI was also removed making BMI a better predictor in the multivariable model. This can be observed by comparing the c-statistics and AIC with (0.77 and 107.8) and without BMI (0.74 and 184.6) in the model.
Discussion
Body mass index has been shown to affect screening of AAAs, operative decisions, surgical outcomes, postoperative complications, and mortality in various surgical procedures, including in elective AAA repairs, although this has not been consistent. Giles et al demonstrated a higher 30-day mortality in morbidly obese patients (BMI >40 kg/m2) undergoing elective AAA repair than obese or nonobese patients (4.3% vs 1.7%-3.7%, respectively). 16 However, while the study by Johnson et al 17 demonstrated increased incidence of certain postoperative complications (eg, wound, renal, and cardiac complications) in obese patients, there was no difference in 2-year mortality among different BMI groups. Studies of the relationship between BMI and other vascular procedures demonstrated, in general, highest mortality in underweight patients (BMI < 18 kg/m2), with lower mortality seen in overweight and obese patients. 18 -20
Body mass index has not been included in previously established risk scoring systems that predict mortality after the repair of rAAAs. 4 -8 However, there is definitely a signal between BMI and mortality in elective repairs of AAAs. 3,16 There continues to be ambiguity in this area as contradictory results have been reported demonstrating no significant difference in mortality based on BMI alone. 17,21 However, other investigations analyzing outcomes in vascular surgical procedures outside of AAA repair such as lower extremity revascularizations, cerebrovascular procedures, and amputations also show a significant relationship between BMI and mortality. 18 -20
This study represents a large cohort of patients with rAAA across 2 academic institutions demonstrating the potential predictive value of BMI on perioperative mortality. These 2 institutions have designated protocols in place for taking care of patients with ruptured aortic aneurysms with almost similar resources. From Indiana University Methodist Hospital, there were 124 number of patients, while the remaining 78 patients were from University of Wisconsin. There were no statistical differences in age (P = .2659), gender (P = .619), BMI (P = .4043), procedure type—endo vs open (P = .158), and Glasgow aneurysm score (P = .9572) between these 2 institutions, indicating no difference in the underlying patient characteristics across the centers. Our final multivariable model included BMI, physiologic scores, age, gender, type of procedure (endo vs open), and health facility. Our conclusions were based on the analysis of this combined cohort. Future derivations and validations of risk scoring systems for rAAAs should consider BMI as a variable as they continue to play an important part of vascular surgical practice. As Robinson et al pointed out, these scoring systems continue to help identify patients in which repair would be futile and assist with fair comparisons of surgical outcomes of rAAAs between individual surgeons and institutions by providing the appropriate patient risk adjustment. 5
Another consideration is the potential differential effects of BMI on open versus endovascular repair techniques. There is evidence that BMI (on both low and high extremes of the spectrum) is associated with frailty, 22 which is known to have an adverse effect on postoperative morbidity and mortality. Due to generally increased surgical stress during open compared to endovascular operative repairs, BMI and its associated frailty may have more effect on postoperative outcome of open repairs. We did not report the differences between the effects of BMI on open versus endovascular repairs because of small numbers within each cohort and no difference noted upon our initial analysis. Additionally, prior reports find that underweight patients undergoing various vascular procedures have the highest mortality. 18–20 However, there were no underweight patients in this cohort. We do not know the cause of this specific oddity, but perhaps a thin body habitus allows for easy physical diagnosis by palpation before growth to a size large enough to rupture consistently.
In addition, our results are similar to those presented by the randomized studies comparing the open versus the endovascular therapy for rAAA. A French randomized study, 23 examining 107 patients with rAAA, reported statistically nonsignificant 30-day mortality of 18% in the endovascular group and 24% in the open repair group. The Amsterdam Acute Aneurysm trial 24 with 116 patients reported a 30-day mortality of 21% for the endovascular and 26% for the open repair. In addition, in Endovascular versus Open Strategy for ruptured abdominal aortic aneurysms (IMPROVE Trial) 25 with 316 randomized patients, a strategy for endovascular repair was not associated with significant reduction in either 30-day mortality or cost. In the IMPROVE trial, 36.4% mortality was reported for the endovascular group and 40.6% for the open repair.
There are limitations to this study, including the inherent selection and survival bias of patients who are transferred to the 2 tertiary referral hospitals who are alive at the time of operation and were offered an intervention. Also, this was a retrospective study that allowed collection and analysis of only the data that were recorded in the patient charts, and there were no matched controls, introducing the possibility of confounding variables that may not have been eliminated by multivariable analysis. Authors acknowledge the potential for a type 2 error given the small number of patients. However, to mitigate this, we used a model with lower AIC and higher c-statistics as the favorable model with better predictive ability to preoperatively estimate mortality after rAAA repair. As indicated above with regard to the sample size, the only few randomized studies comparing the open versus endovascular repair for ruptured aneurysms have very similar number of patients. Longer follow-up may also yield differing mortality outcomes, but that data were not available to us readily. The strength of this study derives from the relatively large numbers for this pathology, ruptured aneurysms, and represents real-world data from 2 tertiary referral centers with rAAA protocols in place.
Conclusion
Patients with high BMI are at increased likelihood of perioperative mortality after repair of ruptured aortic aneurysms. Therefore, considering developing accurate risk scoring systems incorporating patient BMI may improve the predictive value of existing models as we demonstrated in this study. Further, modifications should be considered to existing aneurysm screening protocols for patients with higher BMI, given the higher likelihood of mortality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.