
Abstract
Objective:
Patients who present acutely with a femoral deep vein thrombosis (DVT) diagnosed by ultrasound are often treated with anticoagulation and instructed to follow-up electively. This study sought to assess whether obtaining axial imaging of the central venous system results in the identification of additional iliocaval pathology warranting treatment.
Methods:
This study was a retrospective review of a prospectively maintained registry from November 2014 through April 2017 with follow-up through March 2020. Consecutive patients with a diagnosis of femoral DVT diagnosed by ultrasound were evaluated; those who underwent axial imaging of the iliocaval system (Group A) were compared to those who did not undergo imaging of the central veins (Group B). The primary outcome was the performance of any percutaneous central venous intervention. Secondary outcomes included the extent of DVT identified on duplex and after axial imaging, follow-up duplex patency and persistence of severe symptoms.
Results:
Eighty patients presented with an ultrasound diagnosis of a femoral vein DVT. Mean follow-up was 551 ± 502 days. Group A comprised 24 patients (30%) and Group B comprised 56 patients (70%). Baseline demographics did not differ significantly between the 2 groups. After duplex imaging, Group A exhibited an increased prevalence of DVT in the common femoral vein. After central imaging, Group A exhibited an increased prevalence of DVT in the iliocaval veins. The number of patients who underwent invasive treatment differed significantly between the 2 groups, Group A 16/24 (67%) vs. Group B 9/56 (16%), P < 0.0001. The number of patients that demonstrated duplex patency and had persistent symptoms on follow-up did not differ significantly.
Conclusions:
Patients with an ultrasound diagnosis of femoral DVT may have additional iliocaval pathology warranting intervention. Well-selected imaging of the central veins may reveal a more complete picture, potentially altering management.
Introduction
The initial diagnosis of a lower extremity deep vein thrombosis (DVT) is typically based on a combination of clinical evaluation as well as venous duplex ultrasound. Clinical evaluation comprises a targeted history and physical examination with the purpose of improving the positive predictive value of subsequent testing, and this may involve the use of clinical tools such as the Wells Score. 1 The severity and the distribution of the presentation may also influence the kind of testing that is chosen, and this may range from laboratory testing, to a venous duplex, or to axial imaging of the abdomen and pelvis or of the chest.
Venous duplex ultrasound (VDU) remains the gold standard for the diagnosis of lower extremity deep vein thrombosis. It is highly sensitive and specific, and it provides information on the character, extent and distribution of disease, as well as the mobility and chronicity of the thrombus. 2 VDU is used most commonly to evaluate the venous system from the common femoral vein proximally to the tibial/muscular veins distally, and there are well-defined protocols for this. 3 Evaluation of the iliofemoral segment by VDU is less well codified, and evaluation of the more central iliocaval system remains the most challenging, least standardized, and is often limited by body habitus, bowel gas and operator experience. These adverse conditions may be exacerbated in the emergency setting. 4
Venous anatomy nomenclature has been evolved with possible consequences for delineating iliofemoral and iliocaval disease extension. 5 For example, the nomenclature “superficial femoral vein” has been replaced by “femoral vein,” and this can be a source of confusion for providers outside the vascular specialty. Evaluation of the profunda femoris vein is not performed routinely, and there is significant variability in anatomy. 6 The common femoral / external iliac vein boundary is often confounded, possibly resulting in greater variability in reporting. Lastly, there may be a subgroup of patients with acute femoropopliteal DVT superimposed on synchronous non-thrombotic or chronically diseased central veins (e.g. May-Thurner syndrome), and this may be missed by the venous duplex.
Therefore, there may be a group of patients with femoral or common femoral veins DVT diagnosed by VDU in whom synchronous iliofemoral or caval disease is missed, due to the aforementioned diagnostic limitations. These patients may warrant axial imaging of the abdomen and pelvis and/or venogram to interrogate the central veins. This may influence the decision for hospitalization and the consideration for interventional as compared to medical management. In patients with a common femoral or femoral DVT identified by VDU, this study sought to evaluate whether central venous imaging would identify additional iliofemoral or caval pathology warranting treatment.
Methods
This study was approved by the institutional review board of New York University Langone Medical Center, research number 14-01626. This study was a retrospective review of a prospectively maintained registry from November 2014 through August 2017 with clinical follow-up through March 2020. The registry is maintained by the Venous Thromboembolic Center (VTEC) at New York University Langone Health (NYULH). The function of the registry is to capture all patients presenting to NYULH with the diagnosis of DVT and who provide informed consent to have their information collected in a prospective manner. All qualifying patients are interviewed by the VTEC nursing staff, evaluated, and have their demographic variables collected prospectively.
Consecutive patients were evaluated who were diagnosed by VDU with any common femoral or femoral DVT. A common femoral DVT was defined as occurring below the inguinal ligament and above the common femoral vein bifurcation (i.e. above the division into the femoral and profunda femoris veins). Femoral DVTs were subclassified into proximal or distal in order to further stratify the potential for iliofemoral involvement. A proximal femoral DVT was defined as abutting, but not extending into, the common femoral vein and correspondingly located in the upper thigh. A distal femoral vein DVT was located in the mid or distal thigh. The patients underwent assessment by clinicians from a range of clinical specialties including vascular surgery, emergency medicine, cardiology, hematology and interventional radiology. The patients were divided into 2 categories. Group A included those patients who underwent additional central venous imaging at the time of diagnosis [computed tomography venography (CTV), magnetic resonance venography (MRV) or venogram with intravascular ultrasound (IVUS)]. Of note, patients who received DSA for central venous imaging underwent for diagnostic but not therapeutic purpose due to reasons such as contrast allergy resource limitation. Venogram performed during an interventions was not included. The decision for central imaging was multifactorial including: malignancy workup (6), previous IVC filter (5), duplex finding of iliocaval DVT (3), worsening symptoms (2), assessing for progression of a prior DVT (2), workup for May-Thurner syndrome (2), confirming findings of iliocaval DVT obtained at an outside institution (2), hydronephrosis (1), and prior ipsilateral arterial access for angiography (1). Group B included those patients who did not undergo central venous imaging.
Patient demographics including medical co-morbidities, surgical history, medications and physical findings were compared between the 2 cohorts. The primary outcome evaluated was the performance a percutaneous central venous intervention. Percutaneous interventions were performed using venogram and/or IVUS and included percutaneous thrombectomy, lytic-based techniques, angioplasty, stenting, and inferior vena cava (IVC) filter placement. The decision to treat, procedural characteristics, and peri-procedural management were left to the discretion of the practitioner; however, all percutaneous recanalization procedures used venogram and IVUS. Additional outcomes included: distribution of DVT at the time of VDU, distribution of DVT at the time of axial imaging, performance of percutaneous intervention, technical success of the percutaneous intervention, placement of an IVC filter, follow-up VDU patency, and persistence of severe symptoms on follow-up.
Follow-up VDU patency was defined as post-procedural patency in patients undergoing intervention or recanalization in patients receiving only medical management. The segments evaluated for patency or recanalization were the index thrombosed veins (i.e.femoral, common femoral, iliac or inferior vena cava). Persistence of severe symptoms was defined as the persistence of chronic venous insufficiency or post-thrombotic syndrome on latest follow-up with debilitating symptoms comprising a combination of heaviness, achiness, swelling, itching, venous claudication, skin changes, and ulceration. All variables were assessed using unpaired Student’s t-tests for continuous variables, and Fisher’s exact test for discrete variables. P < 0.05 was considered statistically significant.
Results
A search of the NYU VTEC registry from November 2014 through August 2017 identified 80 out of 303 patients, who presented with a diagnosis of any femoral DVT. Mean follow-up was 551 ± 502 days. Demographics for the cohort were as follows: average age (60.4 ± 15.6 years), gender (61.3% male), body mass index (28.7 ± 5.9 kg/m2), history of venous thromboembolic disease (35%), history of tobacco use (40%), known hypercoagulability disorder (5%), family history of venous thromboembolic disease (2.6%), history of symptomatic varicose veins (21.3%), sidedness of pathology (right 42.5%, left 37.5%, bilateral 20%). Group A (patients with central venous imaging) comprised 24 / 80 patients (30%), and Group B (patients without central venous imaging) comprised 56 / 80 patients (70%). In Group A, 16 patients underwent CTV (67%), 6 underwent MRV (25%), and 2 underwent venogram with IVUS (8%). The majority of imaging was requested by providers outside of vascular surgery (66%), while 33% of the imaging was obtained following vascular surgery consultation.
A comparison between the 2 groups revealed that baseline demographics and average follow-up did not differ significantly (Table 1). Evaluating each limb independently, right-sided femoral DVT presented less commonly in Group A as compared to Group B (17% vs. 48%, P = 0.0115). Left-sided DVT (50% vs. 34%, P = 0.2144) and bilateral DVT (33% vs. 18%, P = 0.1509) did not differ significantly between the 2 groups. Presentation with concurrent pulmonary embolism was more frequent in Group B (4% vs. 16%, P = 0.0081). After VDU imaging, Group A exhibited an increased prevalence of DVT in the common femoral vein, Group A (58% vs. 29%, P = 0.0221). In further assessment of the central extent of DVT at the time of venous duplex, there was a trend of greater incidence of iliocaval thrombus in Group A (29% v. 11%, P = 0.0523). Following axial imaging, there was a significantly greater amount of iliocaval thrombus in Group A (58% vs. 11%, P < 0.0001), P < 0.0001, with the anatomical distribution and extent of DVT shown in Table 2.
Patient Demographics.
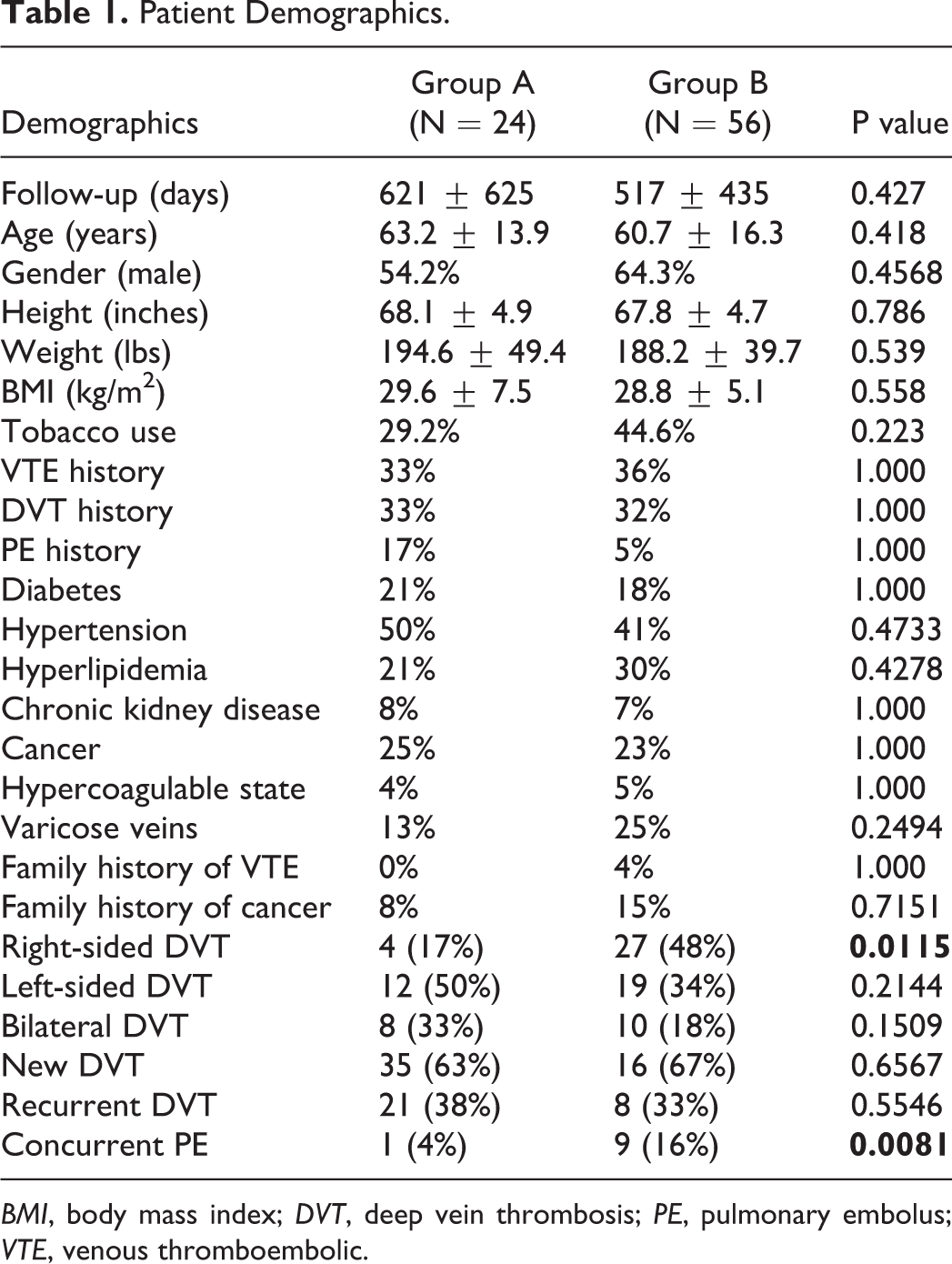
BMI, body mass index; DVT, deep vein thrombosis; PE, pulmonary embolus; VTE, venous thromboembolic.
Intervention, Distribution of DVT, and Outcomes.
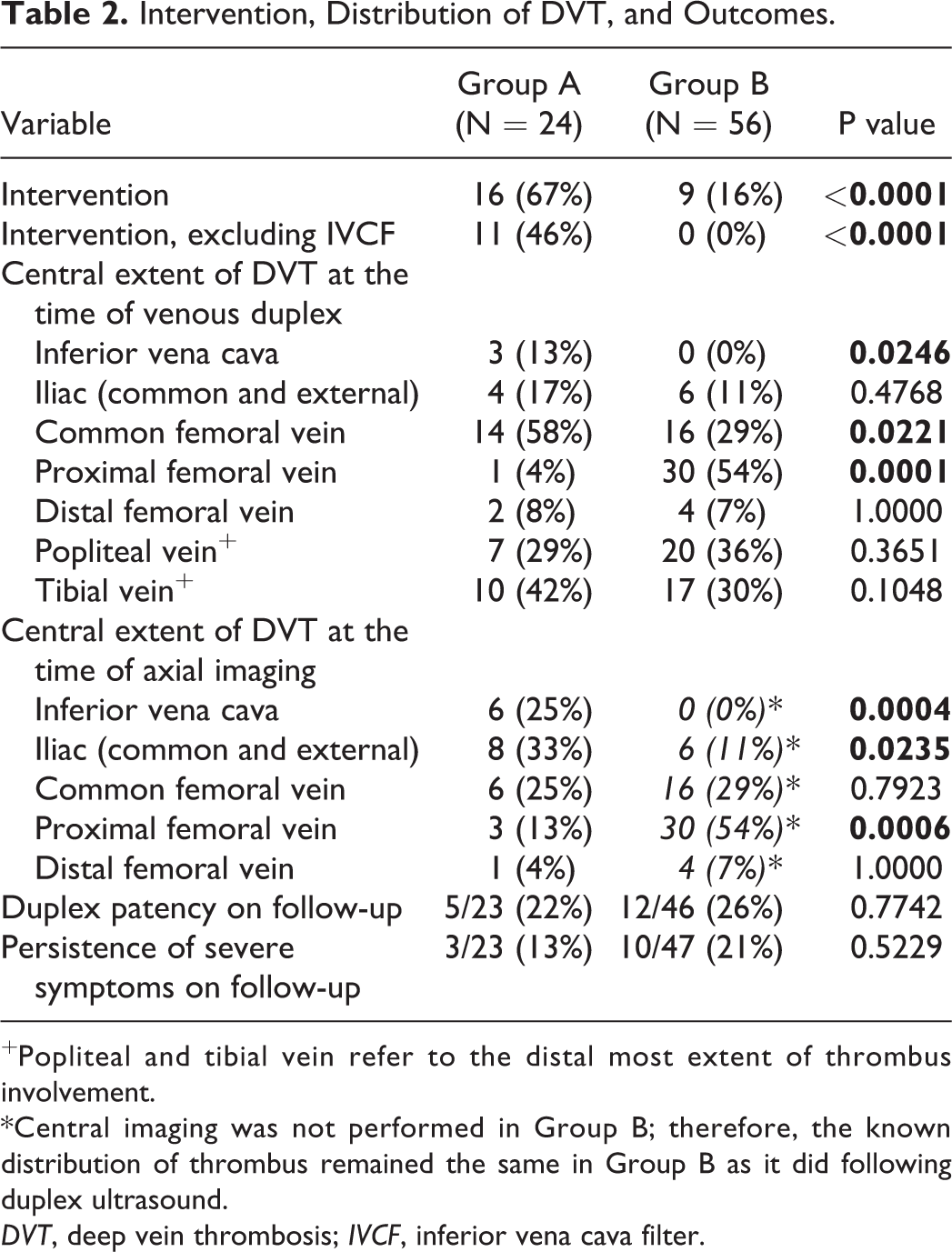
+Popliteal and tibial vein refer to the distal most extent of thrombus involvement.
*Central imaging was not performed in Group B; therefore, the known distribution of thrombus remained the same in Group B as it did following duplex ultrasound.
DVT, deep vein thrombosis; IVCF, inferior vena cava filter.
The number of patients who underwent any form of interventional treatment differed significantly between the 2 groups Group A 16/24 (67%) vs. Group B 9/56 (16%), P < 0.0001 (Table 2). If procedures of sole placement of IVC filters were excluded, the number of invasive procedures remained significantly different between the 2 groups, Group A 11/24 (46%) vs. Group B 0/56 (0%), P < 0.0001. Technical success for recanalizing the central veins was achieved in 8/11 (73%) of patients in Group A. The technical failures were due to the persistence of thrombotic disease (2) or to the inability to traverse chronic disease (1).
With regard to outcomes, VDU anatomic patency on latest follow-up did not differ significantly between the 2 groups, Group A 5/23 (22%) vs. Group B 12/46 (26%), P = 0.7742) (Table 2). However, when evaluating those patients in Group A who underwent an attempt at recanalization, 5/11 (45%) exhibited patency on latest follow-up. Moreover, if you only evaluate those who underwent successful percutaneous recanalization, 5/8 (63%) exhibited patency on latest follow-up. The number of patients who had persistent severe symptoms on long-term follow-up did not differ significantly, but there was a possible trend toward improvement in the imaging group, Group A 3/23 (13%) vs. Group B 10/47 (21%), P = 0.5229.
Discussion
The causes for DVT are multifactorial and based on Virchow’s triad (endothelial injury, stasis and hypercoagulability). 7 Lower extremity DVT is a condition commonly diagnosed in the acute setting. 8 The acute presentation may range in severity from being asymptomatic to presenting with pain and swelling, to limb threatening conditions such as phlegmasia cerulea or alba dolens. 9,10 In general, physical findings of DVT such as tenderness, cyanosis or a positive Homan’s sign are neither sensitive nor specific. Lower extremity DVT may present concomitantly with embolic complications including pulmonary embolism or stroke in the setting of paradoxical emboli. Futhermore, DVT may be a marker for the presence of central venous stenosis. 11 In the long-term, patients are also at significant risk for developing a post-thrombotic syndrome. 12,13
In efforts to improve the sensitivity and specificity for the diagnosis of DVT, multiple scoring methodologies have been developed such as the Well’s score, and these take into account clinical as well as historical variables. 14,15 Ultimately, VDU represents the most sensitive and specific modality for the diagnosis of DVT in the lower extremities. 2 The performance of venous duplex has been standardized by various accrediting bodies. 3 The typical venous duplex includes evaluation of the femoropopliteal system as well as the calf veins.
When it comes to evaluation of the central venous system including the IVC, the iliac veins, and the pelvic veins, diagnosis with non-invasive imaging becomes more limited. 16 -18 Evaluation of the abdomen and pelvis with venous duplex is not performed as commonly and is not standardized to the same extent as it is for the lower extremities. Therefore, there may be more variability based on the operator or institution. Lastly, even with highly skilled operators there are additional study limitations based on patient factors (e.g. obesity, bowel gas, patient cooperativeness, etc).
Although venous duplex remains the gold standard for evaluation of the lower extremity venous system, axial imaging such as CTV, MRV or venography sometimes accompanied by intravascular ultrasound, renders a more accurate evaluation of the central veins. Moreover, axial imaging may more completely delineate the distribution of the thrombus as well as any additional associated pathology. 19 -21 Such additional pathology may include a central venous compression (i.e. May-Thurner syndrome), tumors, retroperitoneal fibrosis, adjacent arterial aneurysms causing local compression, and aberrant deep venous anatomy.
The standard of care for the treatment of DVT remains anticoagulation. 22 Despite publication of Clinical Practice Guidelines of the Society for Vascular Surgery and the American Venous Forum in 2012, the treatment for iliofemoral or caval DVT remains highly individualized. 23 Treatment options may range from the requirement for an IVC filter, percutaneous pharmacomechanical thrombectomy, the newer percutaneous mechanical thrombectomy techniques, open mechanical thrombectomy, or to management of chronic central venous lesions with angioplasty and stenting. 24,25 In rare instances, aberrant anatomy, tumors or other retroperitoneal processes warrant open reconstruction. 26
The ATTRACT trial generated many questions regarding the use of lytic-based therapies for the treatment of iliofemoral DVT. 25 This was a randomized controlled trial that compared patients who were treated with pharmacomechanical thrombectomy with associated adjunctive treatments and anticoagulation, to patients who were treated with anticoagulation alone. The trial demonstrated that at 24 months, there were no significant differences in outcomes in patients who were treated for iliofemoral DVT with lytic-based therapies as compared to patients who were treated with anticoagulation alone. The data suggested a possible improvement in patients presenting with iliofemoral DVT, as compared to femoropopliteal DVT, and the study excluded patients who presented with extensive iliocaval thromboses, such as those with a thrombosed IVC filter. The CaVenT trial demonstrated improved patency and quality of life outcomes for catheter directed lytic therapy in patients presenting with iliofemoral DVT, initially and at 5 years. A Cochrane database systematic review came to same conclusions. 24,27 Moreover, newer methodologies or techniques such as the percutaneous mechanical thrombectomy devices, may lead to an altered risk-benefit ratio due to the avoidance of lytic agents. 28
Regardless of the state of controversy of central venous intervention for the treatment of DVT, the information from a venous duplex that stops routinely at the level of the common femoral vein may be incomplete. Detailed characterization of the central extent of venous thrombosis, and associated anatomy, may alter clinical decision-making and outcomes. The data herein suggest that characterization obtained from axial or venographic imaging of the iliofemoral system has the potential to alter patient diagnosis and management. This study demonstrates that patients with a femoral DVT on ultrasound who also underwent central venous imaging exhibited increased diagnosis of iliocaval disease and underwent 50% more interventions.
Interestingly, patients with left-sided and bilateral disease were evaluated more commonly with central imaging. This may have been due to selection bias, more severe symptoms at presentation, and pre-conceived notions that right sided iliofemoral disease extends less commonly into the iliocaval system as compared to left-sided disease, presumably due to standard May-Thurner anatomy. It is also true that significantly more patients in Group B as compared to Group A were diagnosed with a proximal femoral vein DVT, suggesting further that disease burden was less severe in the non-imaged group. Once again, the decision to obtain central imaging was due to various indications such as workup for malignancy, prior IVC filter, evaluating for May Thurner syndrome, and workup for other pathologies such as hydronephrosis or recent angiogram access with pseudoaneurysm. Obtaining central venous imaging is largely based on practitioner preference and may vary with each institution, and this emphasizes the role for careful patient selection and establishment of a protocol for pursuing more advanced imaging.
When imaging and clinical outcomes were evaluated, the following was gleaned. There was an increase in the diagnosis of iliocaval extension in the imaging group. Some of this may have been attributable to the increased severity at presentation with the attendant selection bias, but some may have been attributable to the improved diagnostic accuracy with axial imaging. This may have resulted in under-diagnosis in Group B, particularly in those patients with common femoral and iliac vein involvement on duplex. In terms of duplex patency on follow-up it is notable that there was no difference between the 2 groups; although, Group A with central imaging may have had more severe disease at presentation. This is relevant in the context of the evidence supporting catheter directed lytic therapy. 24,27 In addition, there was a possible trend toward a lower incidence of persistent severe disease in patients who underwent additional imaging, and again this is notable given that the initial presentation may have been more severe in this group. The trend in improved clinical outcomes occurred even in the setting of 3 interventions in the central imaging group that were not technically successful. Two of the technical failures were due to persistent thrombus, and one of the failures was due to the inability to traverse the underlying chronic lesion in the setting of a chronically occluded IVC filter. Although utility of deep venous interventions in the acute setting is still being debated, the treatment remains highly individualized, and this study suggests that management may be altered and clinical improvements may occur when a complete evaluation of the iliofemoral system is obtained in well-selected patients who present with DVT that involves the femoral vein.
One consideration for patient selection may be to perform central venous imaging on all patients with a common femoral vein (or higher) DVT on venous duplex ultrasound. This would have resulted in central imaging being performed in an additional 16/56 (29%) patients in Group B. With profunda femoris vein inflow being potentially compromised in these patients, there is a theoretically greater risk for synchronous iliocaval disease. The subcategory for proximal femoral vein DVT amounted to 54% of patients in Group B, and additional imaging may be performed more selectively in these patients depending on the clinical context (i.e. severity of the presentation, high index of suspicion for central disease) and careful review of the source images assessing for direct and indirect evidence for central venous disease. Although only comprising a small portion of the total cohort (8%), there were no patients with a distal femoral vein DVT who were found to have concomitant iliocaval disease.
This study was limited by being a retrospective review of a prospectively maintained registry, and therefore patients were not randomized. The demographic variables matched up well between the 2 cohorts; although there was a difference in sidedness between the 2 groups, and the patients in the central imaging group may have had a greater thrombus burden at presentation. Moreover, there may have been selection bias in the patients undergoing iliofemoral imaging. This may have been related to the patient’s index clinical presentation or to practitioner type and preference in terms of diagnosis and treatment.
The study demonstrated that diagnosis and treatment may change when central venous imaging is obtained. Limited trends could be shown with regard to clinical outcomes; however, it is notable that the imaging group, which was more severe, exhibited outcomes that were at least equivalent to the comparison group. This also raises the question whether outcomes in Group B would have been better if the patients with iliac and common femoral vein involvement would have undergone further evaluation. Moreover, the evaluation of clinical outcomes may be further refined with use of more accurate and comprehensive patient reported outcomes, such as the Villalta score. 29 Lastly, a prospective randomized evaluation would help to more definitively determine the utility of central venous imaging in patients diagnosed with a femoral DVT by duplex.
Conclusions
This study suggests that well-selected patients with a femoral DVT may benefit from additional central venous imaging. This may be accomplished by imaging all patients with a common femoral vein DVT and by selectively imaging patients with a proximal femoral vein DVT. Imaging of the iliocaval system may provide a more complete picture of the underlying anatomic distribution of disease, thereby potentially affecting management. Ongoing and prospective evaluations are required to assess if this strategy results in improved clinical and patient reported outcomes.
Footnotes
Authors’ Note
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.