
Abstract
Introduction:
Naftidrofuryl and cilostazol are drugs with proven efficacy in the treatment of claudication in peripheral vascular disease. In this experimental study, we evaluated the effects of naftidrofuryl and cilostazol in ischemia-reperfusion (IR) injury on various tissues.
Materials and Methods:
40 male albino Wistar rats (8-12 weeks old, 250-350 g.) are randomly divided into 4 groups: Control (Group 1), sham (group 2), cilostazol pre-treatment (group 3), naftidrofuryl pre-treatment (group 4). During 21 days placebo is given to group 2, 12 mg/kg/day cilostazol is given to group 3, 50 mg/kg/day naftidrofuryl is given to group 4 orally. Ischemia and reperfusion are induced at the lower hind limb in Groups 2, 3 and 4. Ischemic muscle, kidney, liver, heart, brain and blood samples are obtained. The total antioxidant capacity, oxidant levels and oxidative stress index are studied for each group.
Results:
Both drugs have protective effects of remote organ injury following IR. Systemic effects are similar to each other, both have protective effects of IR injury. It showed no statistical significance in the total antioxidant capacity. Total oxidant levels are significantly affected by cilostazol in the heart (p < 0.01) and by naftidrofuryl in the liver (p < 0.01). The effect on oxidative stress was only significant with cilostazol on the heart (p < 0.01).
Conclusion:
Cilostazol and naftidrofuryl had beneficial effects in all tissues against tissue damage caused by IR injury. In ischemic muscle, kidney and heart cilostazol had improved outcomes comparing to naftidrofuryl. Naftidrofuryl had benefits over cilostazol in liver tissue.
Introduction
Peripheral arterial disease of the lower extremities (PAD) is a major health problem that can cause significant morbidity and loss of the quality of life. The classic symptom is leg pain when walking which resolves with rest, known as intermittent claudication. Cilostazol and naftidrofuryl are vasoactive drugs that have been proven to improve walking distance in peripheral arterial disease (PAD). 1
Acute critical leg ischemia may develop in patients with PAD despite the use of vasoactive drugs. Revascularization is indicated for critical limb ischemia to prevent tissue or limb loss. Revascularization of an ischemic extremity may induce systemic complications and remote organ damage related to ischemia-reperfusion (IR) injury. IR injury is related to the balance between antioxidant and oxidant parameters. Determination of antioxidant and oxidant parameters can be done individually, but this is time-consuming and expensive. Erel 2 -5 developed the total antioxidant capacity (TAC), total oxidant status (TOS), and oxidative stress index (OSI) measurements that can reflect the status of all oxidants and antioxidants. Although the use of cilostazol and naftidrofuryl is well established in the treatment of PAD, previous studies focused only on the effects of one drug. Data comparing the effects of cilostazol and naftidrofuryl and in IR injury is lacking.
In this study, we compared the protective effects of the pre-treatment with cilostazol and naftidrofuryl against IR injury by measuring oxidant and antioxidant parameters.
Materials and Methods
This experimental study was carried out at the KOU Faculty of Medicine Experimental Research Laboratory after the approval of Kocaeli University (KOU) Faculty of Medicine Experimental Animals Ethics Committee dated 11.11.2014 with project number 45/2014 and decision number 9/2-2014.
Forty male rats, 8 to 12 weeks old, Wistar strain, 250-350 g in weight were included in the study. All rats were maintained under appropriate humidity (50 ± 5%) and heat regulation (22 ± 2 C) for a 12-hour light / dark cycle for 1 week before the study. All rats were given distilled water and a standard rat food diet until the 12th hour before the study. Wistar race male rats were randomly divided into 4 groups as follows: 10 rats in each group: The control group (Group 1) used to obtain baseline values without IR. The sham group (Group 2) given a placebo once a day for 21 days and showed the results of IR without pre-treatment. Rats in the cilostazol pre-treatment group (Group 3) were given 12 mg/kg/day cilostazol 2 times daily via oral gavage. Rats in the naftidrofuryl pre-treatment group (Group 4) were given 50 mg/kg/day naftidrofuryl 3 times daily via oral gavage.
At the end of 21 days, the IR model was created in rats in groups 2, 3, and 4. To create IR injury, 6-hour ischemia was created by blocking the circulation at the right lower limb at the trochanter major level under light ether anesthesia. 6,7 Ischemia was confirmed by Doppler ultrasonography (MD2, Huntleigh Diagnostics Ltd., South Glamorgan, UK). After 6 hours of ischemia, reperfusion was provided for 4 hours by releasing the of a tourniquet and was confirmed by Doppler ultrasound scan. Following 4 hours of reperfusion blood samples were taken intracardially. Tissues were washed by the administration of 100 mL 0.9%NaCl per rat. Ischemic muscle, kidney, liver, heart, and brain tissues were removed in all groups.
Tissue samples were weighed and homogenized in 0.15 M KCl solution (10%, w /v). After the blood samples were taken into an anticoagulant tube and the prepared tissue homogenates were centrifuged at 3500 rpm for 15 minutes, supernatants were stored at −40° C in the freezer until analysis. To evaluate IR injury and the effects of drugs on blood and tissues (liver, heart, kidney, brain, ischemic muscle), TOS levels as oxidant parameter and TAC levels as an antioxidant parameter were studied. Protein determination from tissue samples was studied with the Lowry method. Tissue TAC and TOS results are given in proportion to tissue protein. OSI value was calculated as a random unit by proportioning TOS levels to TAC levels. The formula [OSI (arbitrary unit) = TOS (nmol H2O2 Equiv / mg protein) / TAC (nmol Trolox Equiv / mg protein)] is used to calculate the OSI value. 5
Statistics
IBM SPSS 20.0 (SPSS Inc., Chicago, IL, USA) package program was used. Compatibility with normal distribution was evaluated with the Kolmogorov-Smirnov Test. Numerical variables were given as mean ± standard deviation and median (25th percentile-75th percentile). The difference between the groups was evaluated with the Kruskal Wallis one-way analysis of variance or Tukey Post Hoc Test after suitability for normal distribution was tested. p <0.05 was considered enough for statistical significance.
Results
Total Antioxidant Capacity
The TAC values in all tissues and the paired comparisons among the groups are shown in Table 1. There was a statistically significant decrease in TAC values in the sham group compared to the control group among all tissues.
Total Antioxidant Capacity Results.
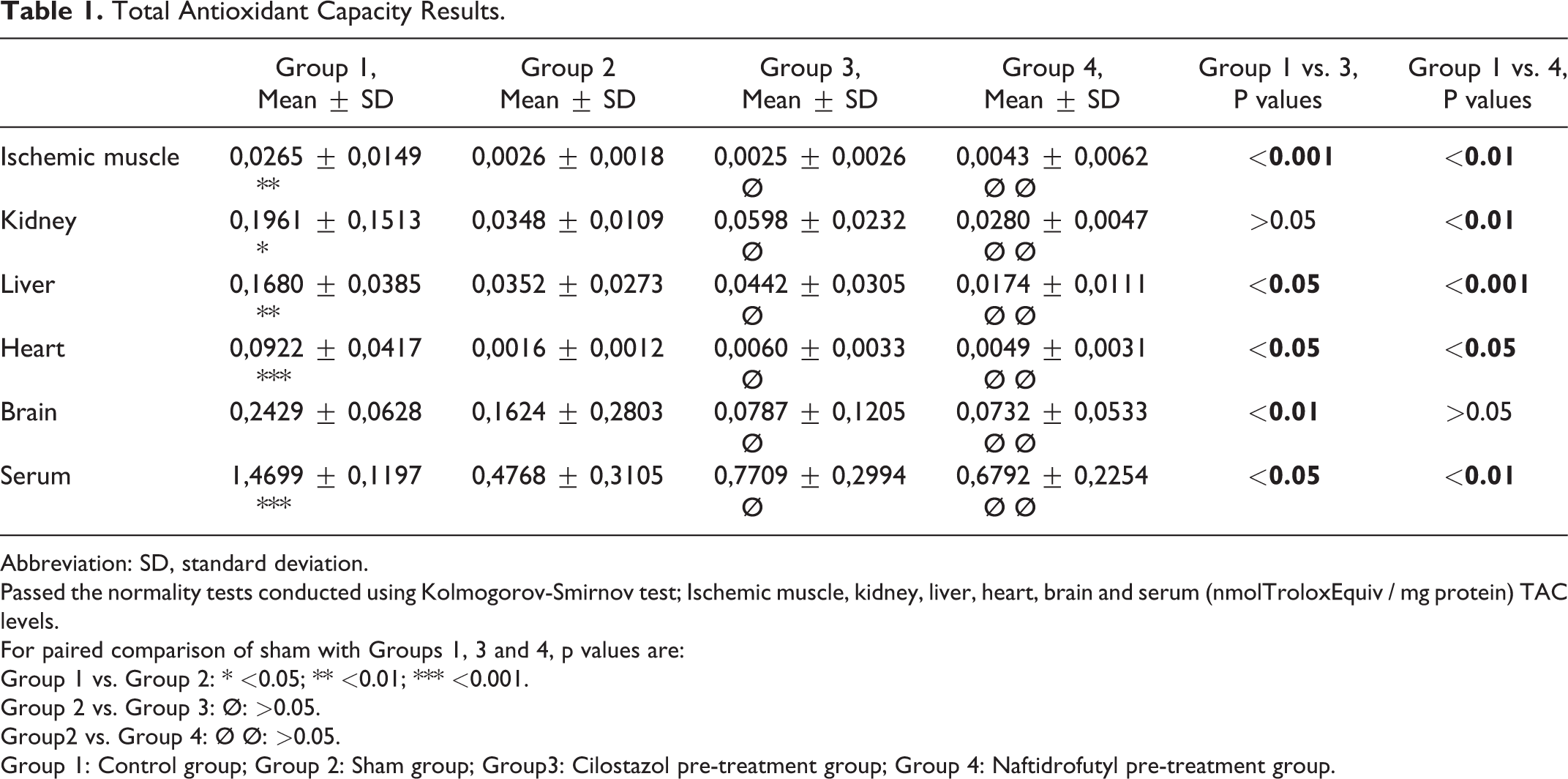
Abbreviation: SD, standard deviation.
Passed the normality tests conducted using Kolmogorov-Smirnov test; Ischemic muscle, kidney, liver, heart, brain and serum (nmolTroloxEquiv / mg protein) TAC levels.
For paired comparison of sham with Groups 1, 3 and 4, p values are:
Group 1 vs. Group 2: * <0.05; ** <0.01; *** <0.001.
Group 2 vs. Group 3: Ø: >0.05.
Group2 vs. Group 4: Ø Ø: >0.05.
Group 1: Control group; Group 2: Sham group; Group3: Cilostazol pre-treatment group; Group 4: Naftidrofutyl pre-treatment group.
In the paired analysis of TAC among all tissues, no significant difference was observed between the sham group and the pre-treatment groups.
Paired analysis of the TAC levels of the pre-treatment groups and the control group were made. Kidney TAC values in the cilostazol pre-treatment group and the brain TAC levels in the naftidrofuryl pre-treatment group were lower compared to control but had no statistical significance (p > 0,05). The TAC values in the remaining tissues were all decreased significantly for both pre-treatment groups comparing to the control group.
There was no statistically significant difference between the pre-treatment groups among all tissues (p > 0,05).
Total Oxidant Status
The TOS values in all tissues and the paired comparisons among the groups are shown in Table 2.
Total Oxidant Status Results.
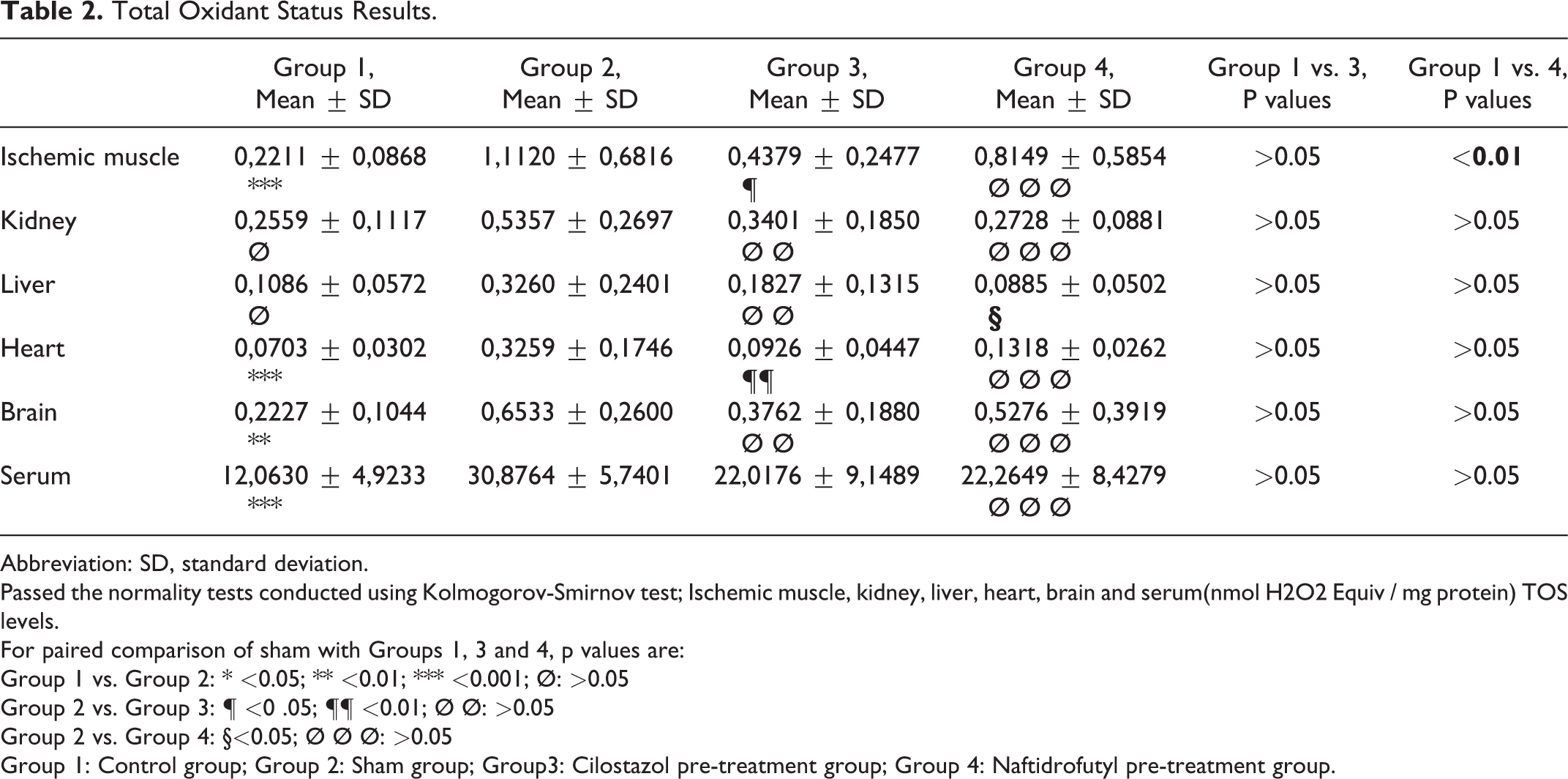
Abbreviation: SD, standard deviation.
Passed the normality tests conducted using Kolmogorov-Smirnov test; Ischemic muscle, kidney, liver, heart, brain and serum(nmol H2O2 Equiv / mg protein) TOS levels.
For paired comparison of sham with Groups 1, 3 and 4, p values are:
Group 1 vs. Group 2: * <0.05; ** <0.01; *** <0.001; Ø: >0.05
Group 2 vs. Group 3: ¶ <0 .05; ¶¶ <0.01; Ø Ø: >0.05
Group 2 vs. Group 4: §<0.05; Ø Ø Ø: >0.05
Group 1: Control group; Group 2: Sham group; Group3: Cilostazol pre-treatment group; Group 4: Naftidrofutyl pre-treatment group.
There was a statistically significant increase in TOS values in the sham group compared to the control group in ischemic muscle, heart, brain, and serum. A statistically insignificant increase is observed for the kidney and liver.
Paired analysis of the TOS levels of the sham group and pre-treatment groups were made. However, this decrease was only significant for naftidrofuryl pre-treatment in the liver tissue (p < 0,05) and cilostazol in the ischemic muscle (p < 0.05) and heart tissue (p < 0,01).
Paired analysis of the TOS levels of the control group and pre-treatment groups were made. TOS values in the ischemic muscle of the naftidrofuryl pre-treatment group were significantly higher compared to the control group. There was no other significant difference between the remaining results of the control group and pre-treatment groups.
There was no statistically significant difference between pre-treatment groups in other tissues (p > 0,05).
Oxidative Stress Index
The OSI values in all tissues and the paired comparisons among the groups are shown in Table 3.
Oxidative Stress Index Results.
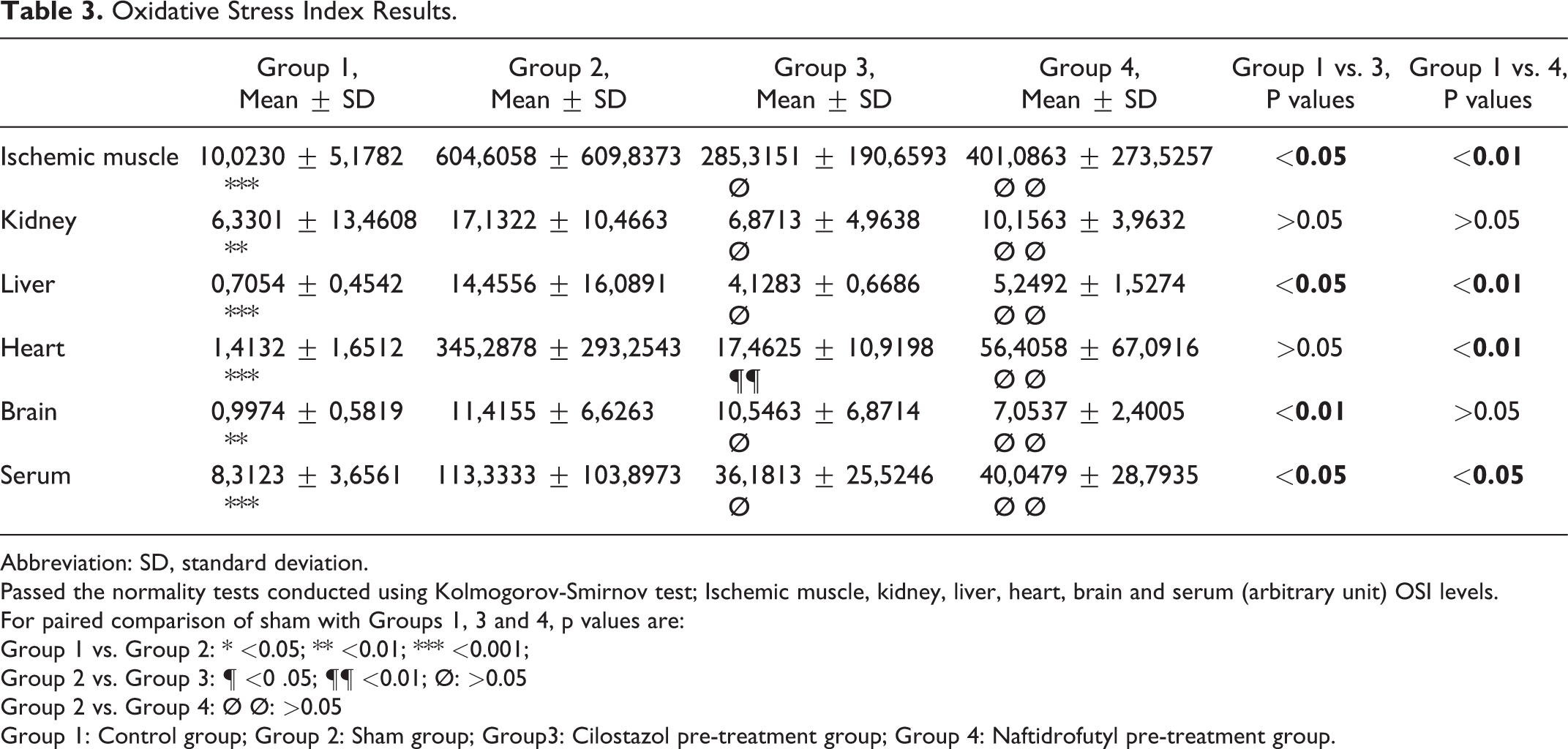
Abbreviation: SD, standard deviation.
Passed the normality tests conducted using Kolmogorov-Smirnov test; Ischemic muscle, kidney, liver, heart, brain and serum (arbitrary unit) OSI levels.
For paired comparison of sham with Groups 1, 3 and 4, p values are:
Group 1 vs. Group 2: * <0.05; ** <0.01; *** <0.001;
Group 2 vs. Group 3: ¶ <0 .05; ¶¶ <0.01; Ø: >0.05
Group 2 vs. Group 4: Ø Ø: >0.05
Group 1: Control group; Group 2: Sham group; Group3: Cilostazol pre-treatment group; Group 4: Naftidrofutyl pre-treatment group.
There was a statistically significant increase in OSI values in the sham group compared to the control group among all tissues.
The paired analysis showed a decreased OSI of all tissues for both of the pre-treatment groups comparing to sham. However, a statistically significant decrease of OSI is only provided with cilostazol pre-treatment in heart tissue (p < 0,01).
An increase is observed for OSI values in all tissues in the paired analysis of pre-treatment groups and control groups. This increase was statistically significant in the ischemic muscle, liver tissues, and serum samples for both drugs, in the heart tissues for naftidrofuryl pre-treatment, and brain tissue for cilostazol pre-treatment.
There was no statistically significant difference between the pre-treatment groups (p > 0,05).
Discussion
Naftidrofuryl and cilostazol are the most used oral vasoactive drugs to improve leg function in patients with intermittent claudication. 1,8
The effect of both drugs on decreasing walking impairment and cost-effectiveness are compared in several studies. 9,10 Stevens et al. 11 found that naftidrofuryl and cilostazol both provided effective treatment in terms of maximum walking distance and painless walking, but naftidrofuryl was found to be more effective and had fewer side effects.
A serious complication of chronic peripheral arterial disease is acute limb ischemia. It can cause limb and life-threatening complications even after successful revascularization. Toxic oxygen free radicals are formed in the ischemic period. Following reperfusion and with the effect of these radicals through regional pro-inflammatory mediators, endothelial damage develops, vascular permeability increases, and tissue edema occurs. 12 With the effect of activated neutrophils, adhesion molecules, and cytokines, a systemic inflammatory response develops throughout the body. This results in damage to remote organs. The lung, heart, brain, and kidneys are mainly affected by this chain of events which is called an IR injury. 13,14
The TAC values in our study decreased significantly in all tissues of the sham group comparing to the baseline values (control group) (Table 1). TOS increased significantly in ischemic muscle, heart, brain, and serum, a non-significant increase was measured in the kidney and liver (Table 2). Consistent with these findings, OSI increased significantly in all tissues after IR (Table 3). These results show us that our IR model successfully induced oxidative stress and free radical production that mediates to IR injury and the consumption of antioxidants in response.
Naftidrofuril acts by selectively blocking vascular and platelet 5-hydroxytryptamine 2 (5-HT2) receptors. 5-HT2 related amplification of platelet function and vasoconstriction is inhibited. 15 Additionally, it enhances aerobic glycolysis by action on succinodehydrogenase and, preserves the cell adenosine triphosphate pool and improves oxygen consumption in ischemic tissues. 1,16,17 Cilostazol is a phosphodiesterase inhibitor that both suppresses platelet aggregation and has a vasodilating effect. 1 The modulation of the oxidant-antioxidant system plays an important role in reducing the damage of IR injury. It is demonstrated that cilostazol pre-treatment significantly decreases IL-6 levels with prolonged use and decreases lipid peroxidation and reactive oxygen species following IR injury. 18 -20 TAC and OSI values were similar among pre-treatment groups in ischemic muscle compared to sham (Table 1, Table 3). Cilostazol pre-treatment enabled to maintain the TOS values of ischemic muscle near to baseline values despite IR injury(P > 0.05), while a significant elevation of TOS levels was observed in naftidrofuryl pre-treatment group comparing to control group (p < 0.01). Additionally, cilostazol pre-treatment provided lower TOS levels comparing to sham (p < 0.05) (Table 2). Despite both pre-treatment groups did not differ from each other in means of TOS levels in ischemic muscle. Cilostazol seems to be more beneficial in the IR injury of the ischemic muscle (Figure 1).
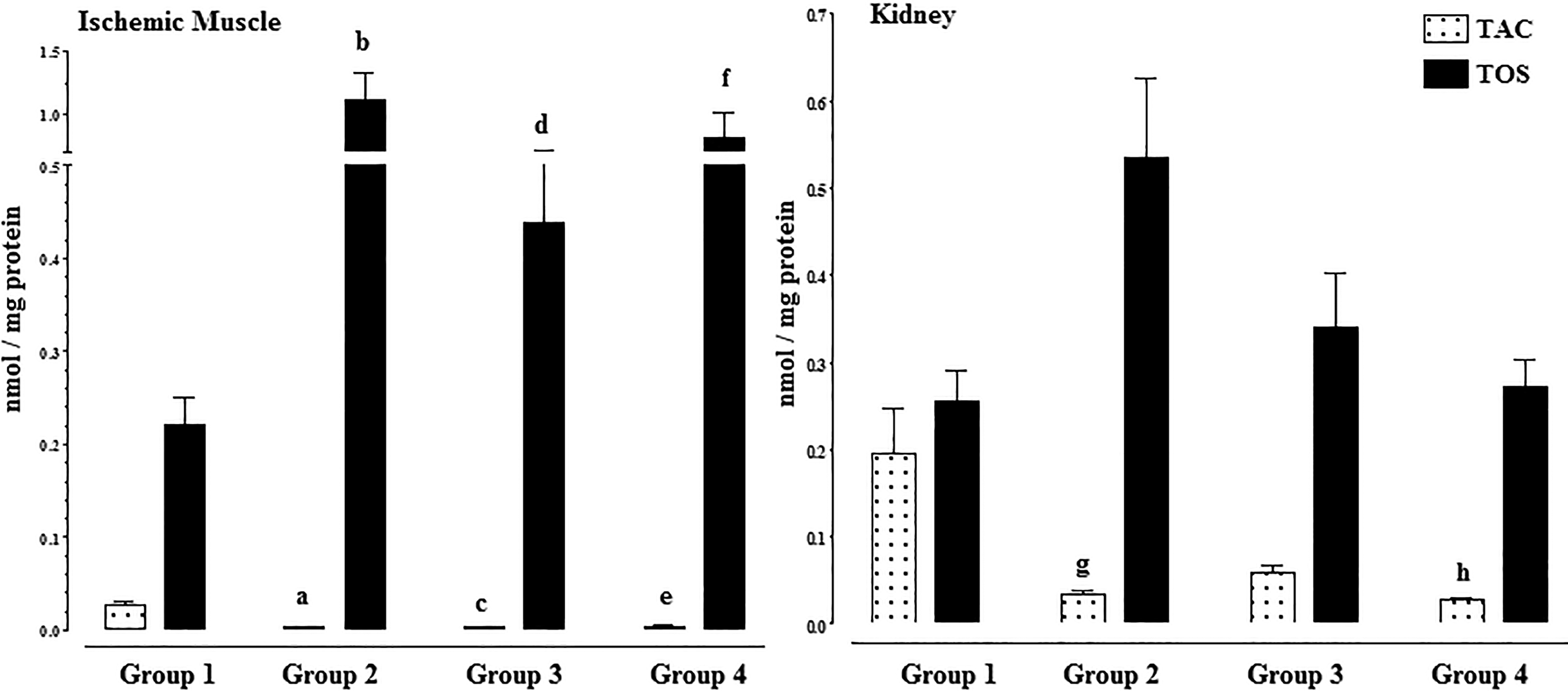
The distribution of total antioxidant capacity and total oxidant status values among groups (variables were given as mean ± standard deviation). a: Group 1 vs Group 2, p < 0.01; b: Group 1 vs Group 2, p < 0.001; c: Group 3 vs Group 1, p < 0.001; d: Group 3 vs Group 2, p < 0.05; e: Group 4 vs Group 1, p < 0.01; f: Group 4 vs Group 1, p < 0.001; g: Group 1 vs Group 2, p < 0.05; h: Group 4 vs Group 1, p < 0.01.
Cilostazol is known to reduce drug-induced nephrotoxicity by antioxidant and anti-apoptotic activity. 21,22 However its benefit in kidney injury following acute IR injury is not clear and the improved results might be dose-dependent. 23,24 In kidney tissue, no significant difference for TOS, TAC, or OSI was present among pre-treatment groups or by comparing the pre-treatment groups to sham. The TOS and OSI values in both pre-treatment groups did not differ compared to baseline (group1). The TAC of the naftidrofuryl pre-treatment group was significantly lower comparing to baseline values (p < 0.01) whereas it had statistically insignificant changes in the cilostazol pretreated group. This phenomenon can be a result of the augmented consumption of antioxidants in the naftidrofuryl pre-treatment group. In the cilostazol pre-treatment group, a similar result of TOS is reached in kidney tissue with less antioxidant consumption (Figure 1).
Recently an experimental study reported that damage in liver tissue caused by lower limb IR is as severe as IR injury on the liver itself. 25 In liver tissue, both drugs did not statistically significantly affect TAC levels comparing to the sham group. Additionally, no difference was present between TAC levels of pre-treatment groups. However, TOS values were significantly lower in the naftidrofuryl pre-treatment group comparing to the sham group (p < 0.05), where cilostazol pre-treatment did not provide a significant reduction comparing to sham. This suggests the benefit of naftidrofuryl pre-treatment in liver IR injury (Figure 2).
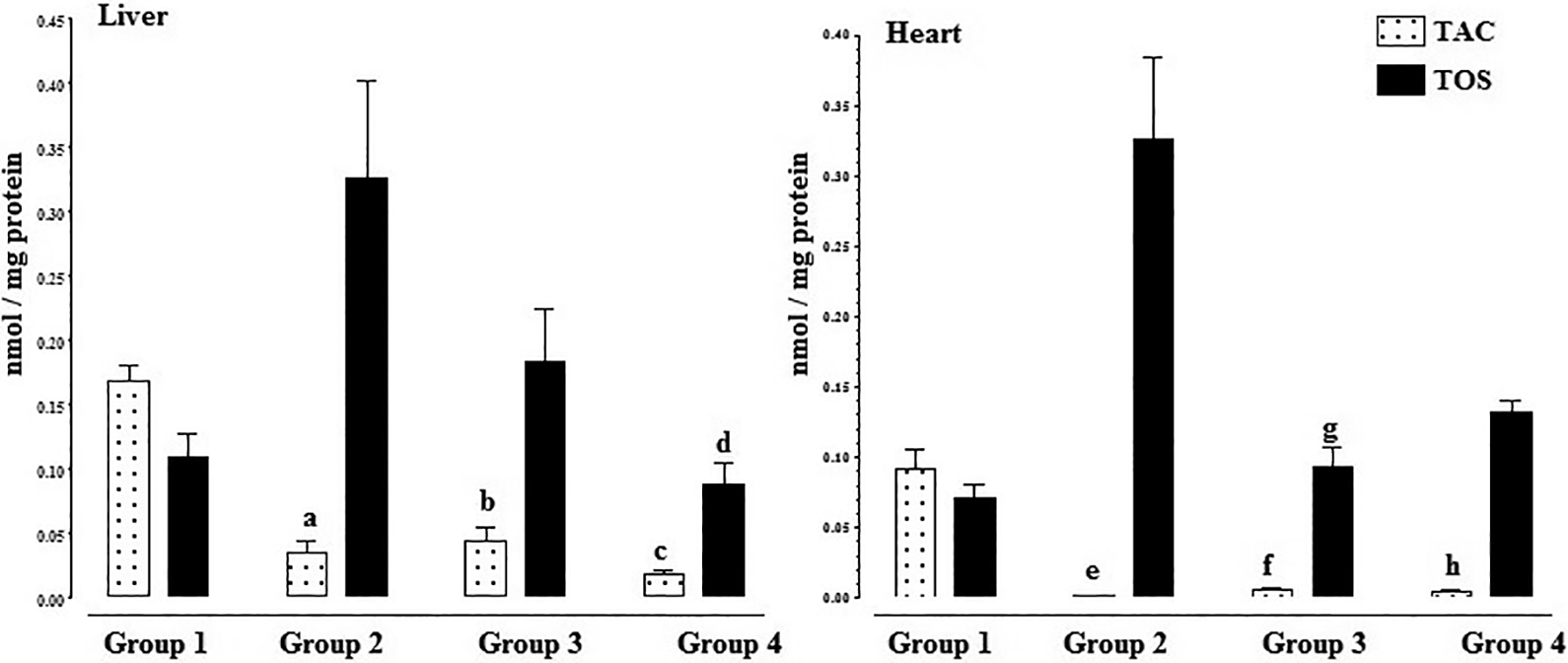
The distribution of total antioxidant capacity and total oxidant status values among groups (variables were given as mean ± standard deviation). a: Group 1 vs Group 2, p < 0.01; b: Group 3 vs Group 1, p < 0.05; c: Group 4 vs Group 1, p < 0.001; d: Group 4 vs Group 2, p < 0.05; e: Group 1 vs Group 2, p < 0.001; f: Group 3 vs Group 1, p < 0.05; g: Group 3 vs Group 2, p < 0.01; h: Group 4 vs Group 1, p < 0.05.
In heart tissue, both drugs did not statistically significantly affect TAC levels comparing to the sham group. Similarly, no difference was present between TAC levels of pre-treatment groups. TOS values were significantly lower in the cilostazol pre-treatment group comparing to the sham group (p < 0.01), where naftidrofuryl pre-treatment did not provide a significant reduction comparing to sham. Similarly, OSI with cilostazol pre-treatment was significantly lower compared to sham (p < 0.05). Additionally, naftidrofuryl pre-treatment had a statistically significant augmentation of OSI values comparing to baseline. This suggests a benefit toward cilostazol pre-treatment although the reduction of TOS and OSI values with cilostazol pretreatment was not statistically significant comparing to naftidrofuryl. Cilostazol is effective in repairing tissue damage caused by IR in the heart tissue and in reducing oxidant stress (Figure 2).
It is thought that cilostazol and naftidrofuryl have protective effects on brain tissue against ischemic damage in experimental studies. 26,27 In our study, we found that when TAC was evaluated in brain tissue, both drugs caused a statistically insignificant decrease compared to the IR group. TOS decreased in both groups, more notably in the cilostazol group. There was a decrease in OSI in the naftidrofuryl group was the more notable augmentation of OSI with naftidrofuryl pre-treatment was statistically insignificant compared to baseline (p > 0.05).
Naftidrofuryl helped to hold the OSI in the baseline but its reduction of TOS was lower than cilostazol. Both drugs may affect reducing oxidant damage but no clear benefit could be demonstrated (Figure 3).
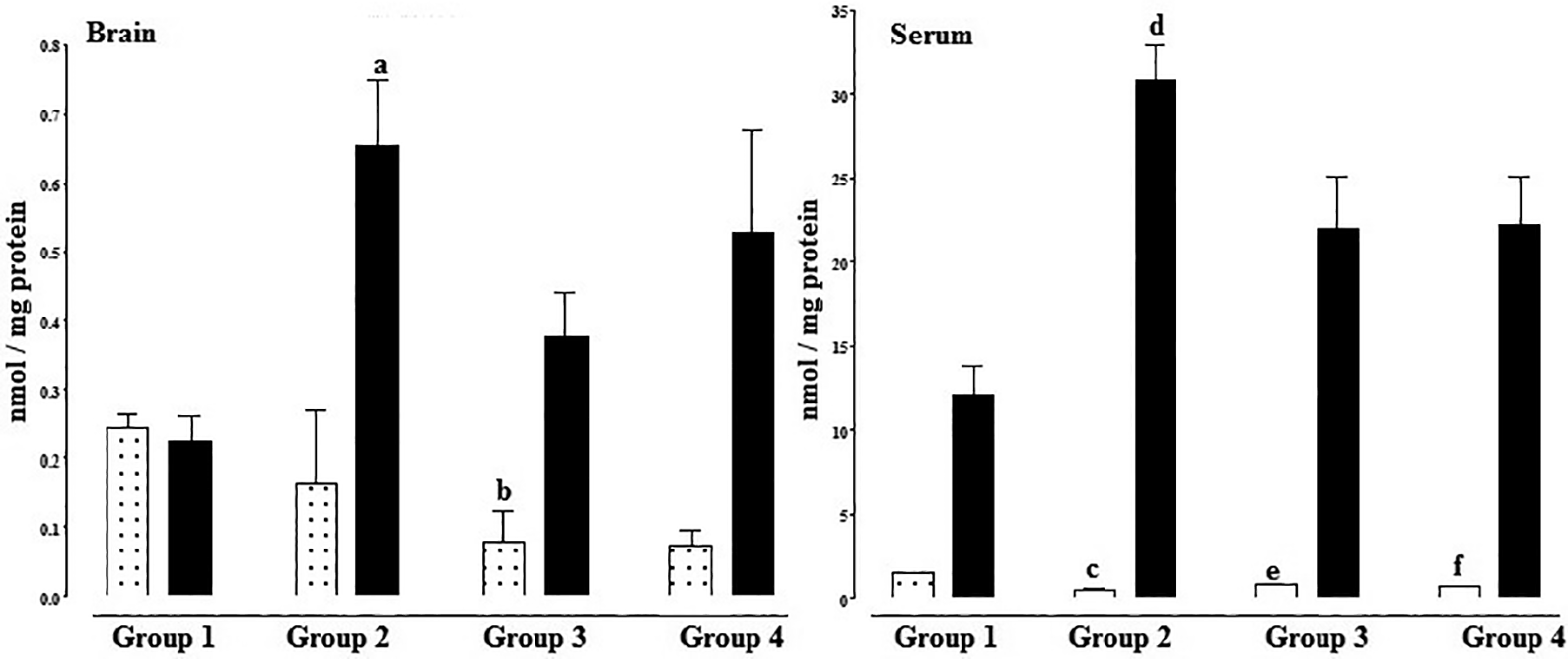
The distribution of total antioxidant capacity and total oxidant status values among groups (variables were given as mean ± standard deviation). a: Group 2 vs Group 1, p < 0.01; b: Group 1 vs Group 3, p < 0.01; c: Group 1 vs Group 2, p < 0.001; d: Group 1 vs Group 2, p < 0.001; e: Group 3 vs Group 1, p < 0.05; f: Group 4 vs Group 1, p < 0.05.
Serum TOS results did not differ significantly from baseline following pre-treatment with both drugs while TAC decreased and OSI increased significantly. TOS and OSI values were lower, TAC was higher in both pre-treatment groups comparing to sham but without statistical significance. A trend toward a beneficial effect due to suppression of TOS and OSI is reached with both drugs (Figure 3). Improved results could be achieved by different dose regiments, longer pretreatment durations or drug combinations.
Conclusion
We observed that cilostazol and naftidrofuryl had beneficial effects in all tissues against tissue damage caused by IR injury. In ischemic muscle, kidney and heart cilostazol had improved outcomes comparing to naftidrofuryl. Naftidrofuryl had benefits over cilostazol in liver tissue. Naftidrofuryl and cilostazol can be used alone or in combination with each other in ischemic patients is supported by a larger number of experimental and clinical studies using different doses. Both drugs provide protection following IR injury but the effects of both drugs on IR damage were limited.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.