
Abstract
Introduction:
aortic aneurysms involving the renal and visceral arteries are endovascular challenges, especially for emergencies. We report a case of ruptured thoracoabdominal aortic aneurysm (TAAA) in a morbidly obese 71-year-old man. The patient was admitted with a stable hemodynamic state. A computed tomography angiogram (CTA) revealed a contained ruptured TAAA with an occluded celiac trunk and left renal artery due to previous nephrectomy. Due to the emergency and his comorbidities, we performed an endovascular aortic repair with the sandwich technique and 2 chimneys. Two bridging stents (chimneys) were deployed between the aorta and the target vessels (superior mesenteric and right renal arteries) in a space created in-between 2 aortic straight endografts. Ten days postoperative, acute renal failure appeared and right renal stent occlusion was diagnosed on CTA. Unfortunately, no adequate kidney revascularization could be obtained, requiring permanent hemodialysis. At a 3-month follow-up visit, the patient did well with stable aneurysm dimensions.
Conclusions:
encouraging outcomes of chimney-EVAR techniques, comparable to those in published reports of fenestrated-EVAR and branched-EVAR, support this procedure as a valid off-the-shelf available alternative in emergency situations. Nevertheless, only few midterm results achieved are actually available and long-term outcomes are actually unknown.
Introduction
Aortic aneurysms involving the renal and visceral arteries are an endovascular challenge. Multiple endovascular techniques are available as custom-made fenestrated endovascular aneurysm repair (f-EVAR) and branched endovascular aneurysm repair (b-EVAR) but these grafts can take 1 to 3 months to manufacture. 1 An “off-the-shelf” alternative as chimney-EVAR (ch-EVAR) or the Zenith T-Branch from Cook are therefore required in emergency situations like ruptured aortic aneurysms. The chimney technique consist of putting a covered stent between a target vessel, which ostia is covered by an aortic endograft, and the aortic lumen. The Concerns with ch-EVAR regarding endoleaks, bridging stent patency and long term outcomes make this approach an oft-debated treatment strategy. 2 Early and midterm outcomes seem to have no significant differences between f-EVAR and b-EVAR techniques. 2,3 Nevertheless, only few midterm results achieved with a variety of devices used are actually available, hard long-term evidence is actually lacking. This promotes further studies with devices combinations standardization. We report a case of a contained ruptured thoracoabdominal aortic aneurysm treated by the sandwich technique with 2 chimneys. Informed consent has been obtained from the patient for publication of the case report and accompanying images.
Case Report
A 71-year-old man was transferred from a secondary hospital to our tertiary emergency department for a contained ruptured thoracoabdominal aortic aneurysm. His medical history was notable for morbid obesity (body mass index of 45 kg/m2), untreated arterial hypertension and a left nephrectomy for a congenital malformation. The patient was in stable hemodynamic state. A computed tomography angiogram (CTA) revealed a contained ruptured type 3 (Crawford classification 4,5 ) thoracoabdominal aortic aneurysm (7,8 x 7,6 x 14,2 cm) and an occluded celiac trunk [Figure 1]. The patient was transferred urgently to the operative room. Due to his major comorbidities, an endovascular approach was preferred. Upper access was obtained through a left axillary artery cut down. In both groins, a retrograde bilateral percutaneous access of the common femoral arteries was favored, with pre-placement of a Prostar (Abbott Vascular, California, United-States) closing device on each sides. Because no alternative off-the-shelf methods were available in our institution, the treatment strategy was a sandwich double chimney technique. As usually, coming from below, a proximal straight aortic endograft (Valiant 38x100 mm, Medtronic, Minneapolis, United-States) was first deployed just above the superior mesenteric artery to cover the thoracic portion of the aneurysm (the celiac trunk was already occluded). The catheterization of the target vessels (superior mesenteric and right renal arteries) from the axillar access was then performed, followed by a second distal straight aortic endograft deployment (Valiant 38x150 mm, Medtronic, Minneapolis, United-States). Between these 2 aortic endografts, we performed 2 chimneys from the aorta to each target vessels [Figure 2]. Three balloon expandable stents (Advanta V12 9x59 mm, Getinge Group, Merrimack, NH, United-States) were used to bridge the superior mesenteric artery (SMA), whereas 1 balloon expandable (Advanta V12 8x59 mm, Getinge Group, Merrimack, NH, United-States), and 1 self-expandable (Viabhan 7x100 mm, Gore, Arizona United-States) stents were necessary for the right renal artery. The completion angiography at the end of the procedure showed complete exclusion of the TAAA, no residual endoleaks, a good patency of the SMA and right renal artery, as well as a retrograde perfused celiac trunk by collateral arteries.
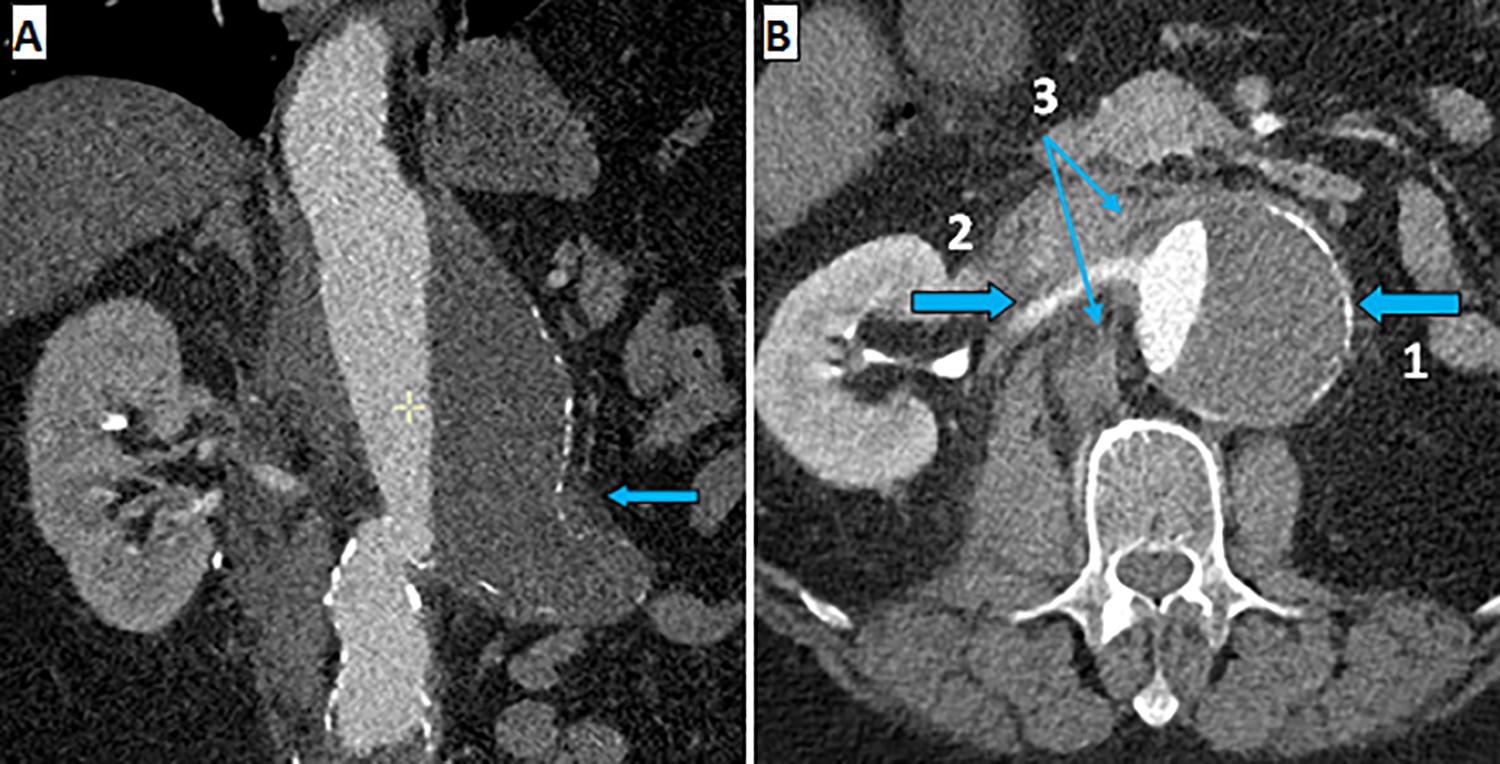
Panel A, thoracoabdominal aneurysm with parietal thrombosis protrusion (arrow). Panel B, contained ruptured thoracoabdominal aortic aneurysm (arrow 1) with a patent right renal artery (arrow 2) and perianeurysmal infiltration suggestive of aortic rupture (double arrow 3).
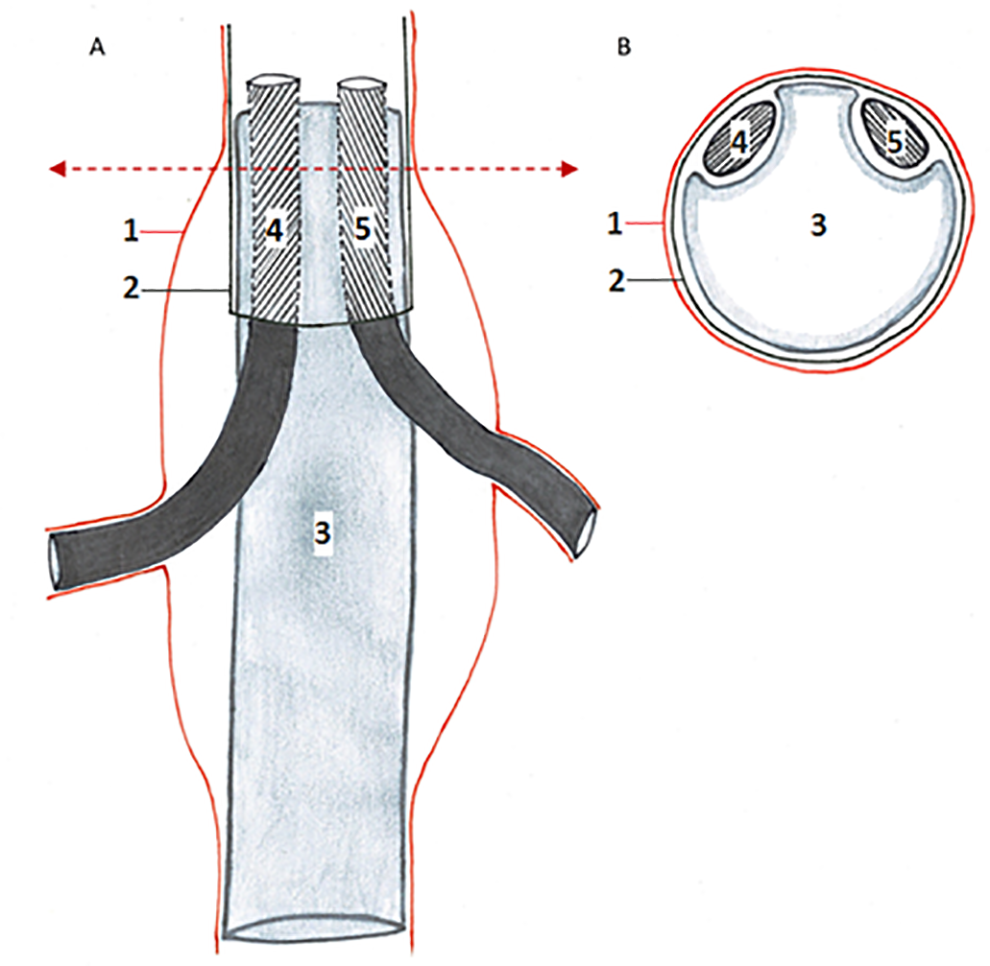
Schematic illustration of the sandwich technique with 2 chimneys (A) and an upper axial slice along the axis of the double arrow (B). Aorta and thoracoabdominal aortic aneurysm (1), proximal (2) and distal (3) thoracoabdominal endografts, bridging stent to the right renal artery (4) and bridging stent to the superior mesenteric artery (5).
In the immediate postoperative course, the patient had a single antiplatelet therapy (Asaflow 80 mg/day) to avoid excess bleeding risks. After 1 week, Clopidogrel 75 mg/day was added to the therapy and the patient was discharged with dual antiplatelet therapy to avoid further bridging stent occlusion.
The postoperative course was complicated at day 10 by an acute renal failure (plasma creatinine: 7 mg/dL) with oliguria. A CTA revealed a complete occlusion of the bridging stent to the right renal artery with a persistent perfused right kidney by a right superior polar artery [Figure 3]. No adequate kidney revascularization could be obtained, leading to permanent hemodialysis. At a 3-month follow-up visit, the patient did well with a urinary output of 500 milliliter daily. A CTA was performed to evaluate the endovascular reconstruction [Figure 4] and revealed stable aneurysm dimensions, but a type 1b endoleak for which a bifurcated endograft is considered.
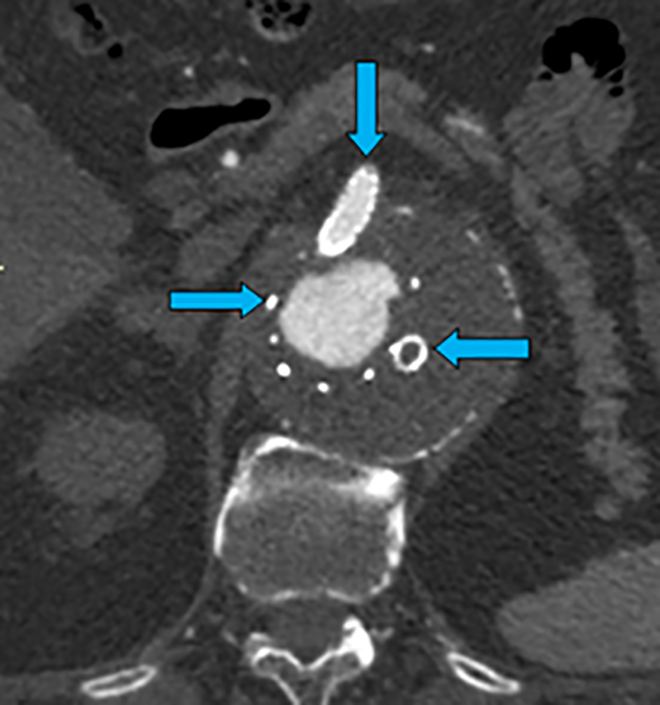
Aortic endograft (left arrow), bridging stent to the superior mesenteric artery (upper arrow), occlusion of the bridging stent to the right renal artery (right arrow).
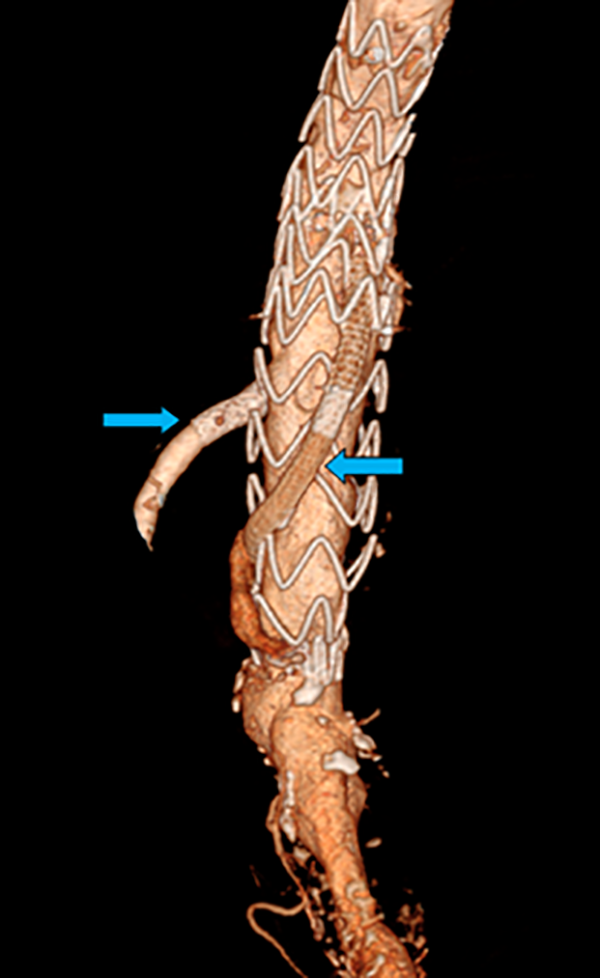
3D reconstruction of the 2 aortic endografts with the bridging stent to the superior mesenteric artery (left arrow) and the bridging stent to the right renal artery (right arrow).
Discussion
Our case concerns a type 3 TAAA in the Crawford classification, involving the distal thoracic aorta to the distal abdominal aorta. Endovascular or open surgical treatments are indicated for these types of aneurysms with a diameter exceeding 5,5 cm. 6,7 An acute intervention was performed in this life-threatening contained ruptured case. 8,9 Those emergency cases are very rare and this particular case demonstrated the feasibility as well as the possible complications related to an endovascular treatment. According to Orr NT et al., 10 open surgical repairs of juxta renal TAAAs seem to have no statistically significant difference in 30-day mortality rates versus endovascular approach (5,7% vs 2,7%, p = 0.126) but higher 30-day morbidity (35% vs 16%, p < 0.001). Concerning ruptured TAAAs, open surgical repairs seem to have higher mortality rates (until 50% vs 31%) as well as higher morbidity rates (overall morbidity until 73% vs 64%) compared to endovascular repairs. 9,11 -15
In our case, an endovascular access was preferred due to the major patient comorbidities and favorable anatomy with only 2 target vessels to bridge without ostial stenosis. Aortic aneurysms involving the renal and visceral arteries are endovascular challenges. Multiple endovascular techniques are available to treat this type of aneurysms including f-EVAR, b-EVAR and ch-EVAR procedures. F-EVAR using “fenestrated grafts” and b-EVAR using “branched grafts” are nevertheless custom-made devices according to individual patients anatomy and can take 1 to 3 months to manufacture. 1 An “off-the-shelf” alternative is required in emergency settings and stated the reason we performed a sandwich technique with 2 chimneys due to the unavailability of other off-the-shelf devices in our institution. First reported in 2003 and 2007, 16,17 the ch-EVAR technique ensures renal and superior mesenteric arteries flow by stenting these arteries in parallel to the main aortic body graft. The sandwich technique we used, in which the bridging covered stents run in a space created by the 2 straight aortic endografts to reach the aortic lumen, also permitted the exclusion of the entire TAAA. During our procedure, most chimneys were ballon-expandable covered stents, as it seems to have a lower type Ia endoleak rate than self-expanding covered stents. 2 Only 1 self-expanding covered stent was deployed in the right renal artery, allowing a sufficient chimney length (>59 mm) up to the aortic lumen.
In this emergency life-treating situation, the rupture had to be covered with an endograft, residual endoleaks can perfectly be treated, after the patient recovers, with an endovascular bifurcated graft extension in an elective setting.
Technical success in ch-EVAR is defined as complete exclusion of the TAAA with a patent aortic endograft and chimney grafts without type I or III endoleak. In our case, an occlusion of the right renal artery stent occurred at day 10 postoperatively requiring permanent hemodialysis. No stent crushing was observed on CTA. The exact cause of the renal bridging stent occlusion is still unknown.
The overall survival with ch-EVAR for TAAAs is between 79 and 83% and the 30-day mortality lies between 0,8 and 4,9% (less than 1% of deaths are procedure-related). 2,3 According to Donas KP et al. 2 in the PERICLES registry, the 30-day mortality for ruptured TAAAs treated by ch-EVAR reaches 24,1%. The overall primary chimney-graft patency in ch-EVAR for TAAAs varies between 94,1 and 95,7%. The majority of chimney occlusions occurs in the renal chimney stent graft and is usually identified during the first 2 months. 2,3 The suggested maximum lengths of the bridging stents are 10 cm for celiac trunk and superior mesenteric artery, 15 cm for antegrade renal arteries revascularization, and 5 cm for retrograde renal artery revascularization. 18 Long-term (dual) antiplatelet therapy seems to be an important adjunct to avoid late branch occlusion. 19 About 17,5% of patients develop some form of renal insufficiency, but only 1,5% require temporary or permanent dialysis. 2 In our case, the increased risk of dialysis was the single kidney condition of the patient. Concerning endoleaks, the perioperative technical success is of about 97%. 2 Endoleaks rate seems to be higher with the number of parallel grafts deployed and it is recommended to create a sufficiently long overlapping with the aortic graft, ranged from 15 to 20 mm 2,3 up to 50 mm. 18 Renal chimney occlusions can be treated by open surgery (iliorenal bypass) or by endovascular repair. Endovascular recanalization (local fibrinolysis, balloon angioplasty or thrombectomy catheter) of occluded renal bridging stents seems to be challenging due to technical difficulties with a few success rate. 3 In our case, no open surgery was performed due to the morbid obesity status of the patient, and no successful endovascular treatment could be performed due to the technical difficulty to recanalize the occluded stent and the lack of thrombectomy catheter.
Concerning TAAA treated by the chimney and sandwich technique, only few data are available, including case reports and small series. Results for acute TAAA are partially even totally combined with elective procedures and ruptures are sporadic cases. Overall, elective and emergency 30-day mortality rates are 6-20%, 7.7% and 100% respectively. Major adverse events were recorded about 15%, including 0-3% persistent paraplegia, 6% permanent renal failure requiring dialysis and 11% type III endoleaks. Primary patency rate was 97.9%. 19,20
Encouraging outcomes of ch-EVAR techniques, comparable to those in published reports of f-EVAR and b-EVAR, support this procedure as a valid life saving off-the-shelf available alternative in emergency situations. 2,3 We have to remember that complications as bridging stent occlusions and endoleaks can occur. Nevertheless, only few midterm results achieved with a variety of devices are available, long-term outcomes are actually unknown and strong data lacks concerning TAAA treated by the ch-EVAR and Sandwich technique, especially in ruptured cases. More and long term results are needed to confirm acceptable complication rates and safety with these procedures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.