
Abstract
Cystic adventitial disease (CAD) is a rare, non-atherosclerotic cause of peripheral arterial disease characterized by mucinous cyst formation in the adventitial layer of arteries; with approximately 80% to 90% of cases involving the popliteal artery. We describe a case of CAD presenting in a female with left external iliac artery occlusion and intermittent claudication, for whom an intra-operative diagnosis of CAD of the ilio-femoral segment was made. A 37-year-old mother-of-two was referred to a Vascular Surgeon with a 3 to 4-year history of progressive intermittent claudication. A computed tomography (CT) angiogram demonstrated a left external iliac artery occlusion. Given the location of the lesion, the absence of cardiovascular risk factors and the patient’s history of cycling, a diagnosis of left external iliac artery occlusion secondary to arterial endofibrosis or spontaneous arterial dissection was thought to be likely. A left Rutherford-Morrison incision was made and an extraperitoneal approach used to expose the left iliac system. A cyst was opened and marsupialized along the superior aspect of the external iliac artery, releasing gelatinous material. A provisional intra-operative diagnosis of CAD was made. The patient was systemically heparinized and an external iliac to common femoral artery bypass was performed using reversed ipsilateral greater saphenous vein. CAD primarily involves the popliteal artery. Under 40 cases of CAD with iliofemoral involvement have been reported. Our case is unusual given the location of CAD, as well as its occurrence in a female. Management options for similar cases have been described in the literature ranging from cyst excision and arterial patching, to interposition bypass and even exclusion bypass, in the case of longer segment occlusions. In our case, an exclusion bypass was deemed the most appropriate treatment given the extensive length and complete occlusion of the external iliac artery.
Introduction
Cystic Adventitial Disease (CAD) is a rare, non-atherosclerotic cause of peripheral arterial disease (PAD) 1 characterized by mucinous cyst formation in the adventitial layer of arteries 2 ; with approximately 80-90% of cases involving the popliteal artery. 1,3 CAD may present with intermittent claudication in young patients who lack cardiovascular risk factors, although it only accounts for less than 0.1% of total cases of claudication. 4 CAD affects males 15 times more than females. 4 We describe a case of CAD presenting in a female with left external iliac artery occlusion and intermittent claudication, for whom an intra-operative diagnosis of CAD of the ilio-femoral segment was made.
Case Report
A 37-year-old mother-of-two was referred to a Vascular Surgeon with a 3 to 4-year history of progressive intermittent claudication. Her symptoms began as a loss of leg power during intense exercise, and progressed to left calf pain and foot numbness when exercising. Her past medical history did not include risk factors for atherosclerosis. Notably, she had previously been a marathon runner and cyclist, and frequently participated in intense spin classes. On examination, she had absent left femoral, popliteal and pedal pulse—right sided pulses were present. A computed tomography (CT) angiogram demonstrated a left external iliac artery occlusion (Figure 1). Given the location of the lesion, the absence of cardiovascular risk factors and the patient’s history of cycling, a diagnosis of left external iliac artery occlusion secondary to arterial endofibrosis or spontaneous arterial dissection was thought to be likely. Surgical treatment options were discussed with the patient including external iliac endarterectomy and vein patch or iliofemoral bypass. The patient opted to proceed with surgical treatment.
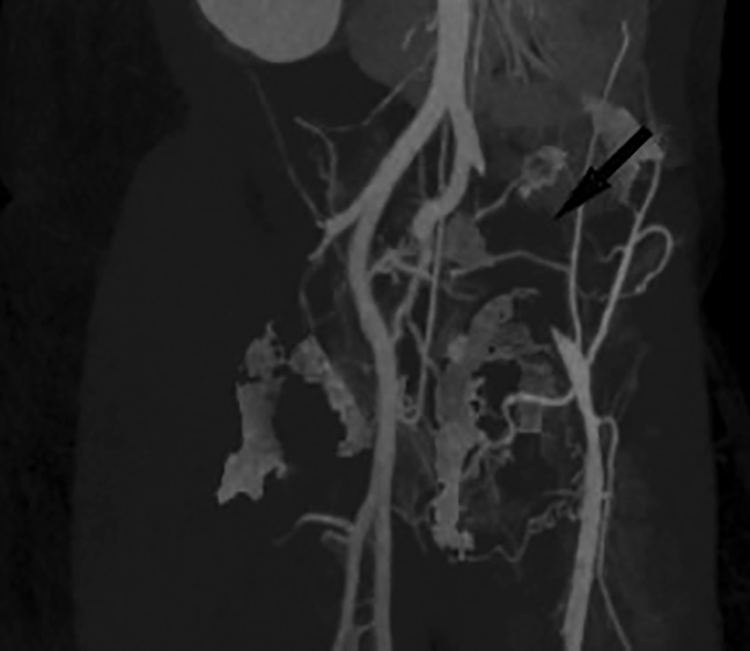
External iliac artery occlusion. Maximal Intensity Projection (MIP) image demonstrating the patient’s left iliac artery occlusion (indicated by black arrow).
A left Rutherford-Morrison incision was made and an extraperitoneal approach used to expose the left iliac system. An intense inflammatory reaction surrounded the origin of the left external iliac artery down to the origin of the common femoral artery. Macroscopically, there appeared to be cystic degeneration of the artery. A cyst was opened and marsupialized along the superior aspect of the external iliac artery (Figure 2), releasing gelatinous material. A provisional intra-operative diagnosis of CAD was made. A left groin incision was made to expose the left common femoral, superficial femoral and profunda femoris arteries. The left great saphenous vein was harvested. Surgeon preference was to use this conduit owing to its durability and autogenous nature. A cystic component was also noted in the lateral aspect of the common femoral artery—this was also decompressed. The patient was systemically heparinized and an external iliac to common femoral artery bypass was performed using reversed ipsilateral greater saphenous vein. The hood of the distal anastomosis extended into the superficial femoral artery to adequately clear the excised common femoral cyst.
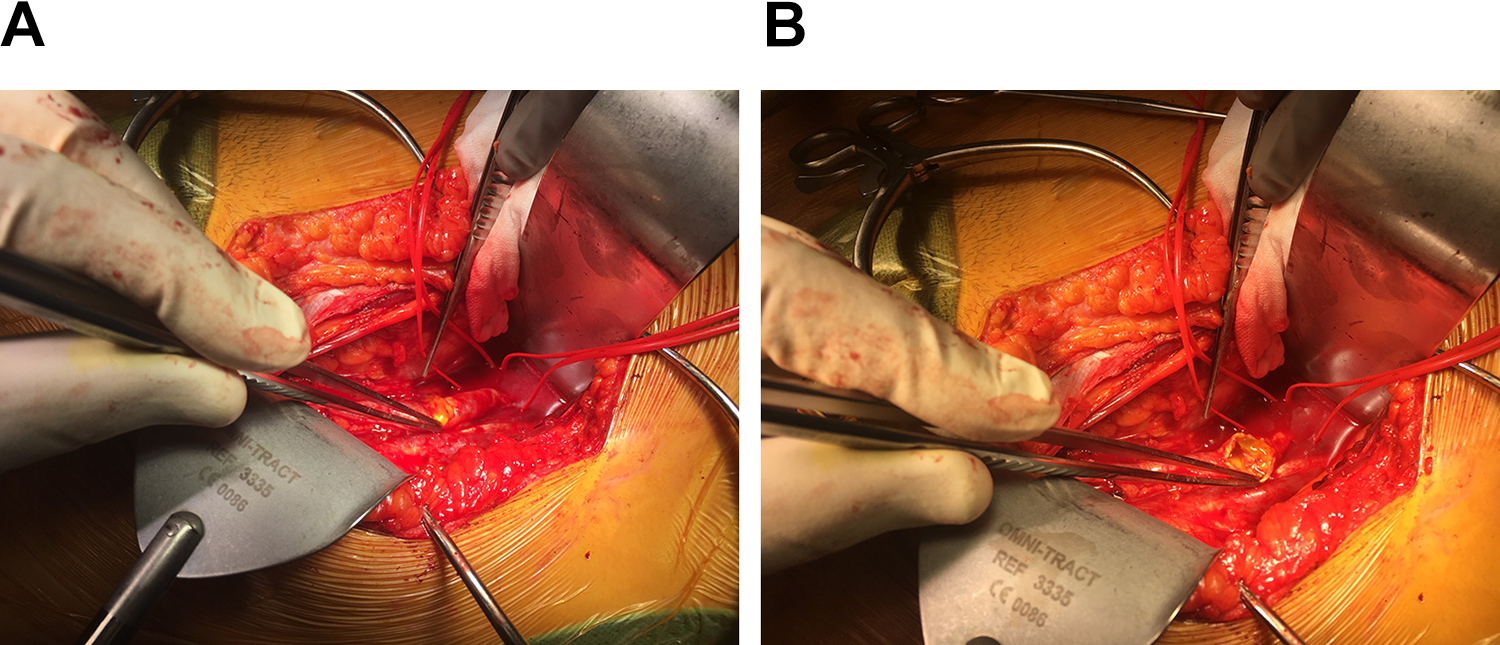
A. Intra-operative images of cystic degeneration of arterial wall. Upon exposure of the external iliac artery, there appeared to be cystic degeneration of the superior aspect of the artery (A). The cyst was opened and marsupialized, with a gel-like substance extruding (B).
Intra-operative specimens of the cystic lesions demonstrated a fibrous walled cystic area devoid of an epithelial lining (Figure 3), characteristic of CAD. The patient’s recovery was uncomplicated, and she remained free of claudication symptoms at her 6-week post-operative follow-up.
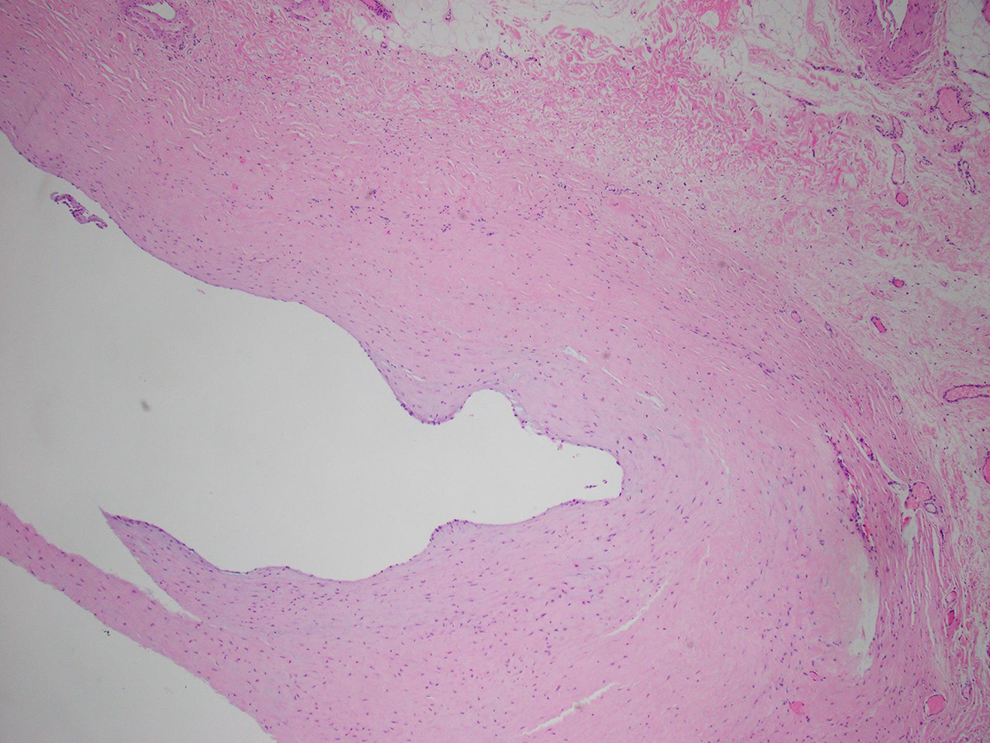
Histological section of cyst. Histological analysis with hematoxylin and eosin staining demonstrated a fibrous walled cyst, devoid of epithelial lining, characteristic of cystic adventitial disease. Image taken at ×40 magnification.
Discussion
CAD primarily involves the popliteal artery. Under 40 cases of CAD with iliofemoral involvement have been reported. 1,4 Our case is unusual given the location of CAD, as well as its occurrence in a female. Management options for similar cases have been described in the literature ranging from cyst excision and arterial patching, to interposition bypass and even exclusion bypass, in the case of longer segment occlusions. 5 -7 In our case, an exclusion bypass was deemed the most appropriate treatment given the extensive length and complete occlusion of the external iliac artery.
Given the patient demographics and history of cycling, arterial endofibrosis was thought to be the most likely diagnosis. Popliteal CAD has also been reported to mimic popliteal entrapment syndrome. 8 CAD may be diagnosed on CT angiography, by its pathognomonic “scimitar sign,” although MRI is regarded as the investigation of choice. 2 In our case, the external iliac occlusion on CT angiogram offered no clues to permit pre-operative diagnosis. While awareness of the diagnosis pre-operatively is not likely to have changed surgical management, it may have reinforced the decision to take an open operative approach. Open surgery is regarded as the management of choice for CAD, with poor outcomes reported from endovascular approaches, despite some case reports of success in certain circumstances. 2,9,10 Similarly, we caution against primary endovascular intervention in PAD patients under 40 where the etiology is unclear. We hope that this report highlights the possibility of this rare phenomena to masquerade as an alternative diagnosis, and underscores CAD’s presence on the list of differential diagnoses for young patients who present with intermittent claudication without atherosclerotic risk factors.
Footnotes
Authors’ Note
Informed consent has been obtained from the patient for publication of the case report and accompanying images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.