
Abstract
Background:
Inferior vena cava (IVC) filters are commonly used in China to prevent pulmonary embolisms in patients with deep vein thrombosis. However, IVC filter removal is complicated when the filter has penetrated the IVC wall and endovascular techniques usually fail. The purpose of this study was to evaluate the effectiveness and safety of retroperitoneal laparoscopic-assisted retrieval of wall-penetrating IVC filters after endovascular techniques have failed.
Patients and Methods:
We retrospectively evaluated a series of 8 patients who underwent retroperitoneal laparoscopic-assisted retrieval of a wall-penetrating IVC filter between December 2017 and November 2019. All patients had experienced at least 1 failure with endovascular retrieval before the study. The filters were slanted and the proximal retrieval hooks penetrated the posterior lateral IVC wall in all patients on computed tomography. Demographic information, operation parameters, and complications were recorded and analyzed. All patients were followed up for at least 12 months.
Results:
The procedure was successful in all patients. The median surgery time was 53.6 ± 12.7 min and the average blood loss was 45.0 ± 13.5 ml. No serious complication occurred during the patients’ hospitalization, which was an average of 6.4 days. The median follow-up time was 15.1 months, and no patient had deep vein thrombosis recurrence.
Conclusions:
Retroperitoneal laparoscopic-assisted retrieval is a feasible and effective technique, particularly when proximal retrieval hooks penetrate the posterior lateral wall of the IVC after endovascular techniques have failed. To some extent, the development of this technique at our institution has increased the success rate of filter removal and improved patient satisfaction.
Introduction
The placement of the inferior vena cava (IVC) filter has been widely used in China to prevent pulmonary embolisms in patients with deep vein thrombosis (DVT), as it seems to be a safer choice than surgical plication or ligation and can be performed with minimal morbidity and mortality. 1 However, chronic indwelling IVC filters are associated with many potential risks, including penetration of the IVC, migration of the filter, infection, thrombotic events, and the potential need for lifelong anticoagulation. 2 IVC filters should be removed once the risk of pulmonary embolism has returned to baseline to prevent the significant morbidity associated with retained filters. 3
Although the retrieval rate has increased in recent years, a proportion of retrievable IVC filters cannot be removed by conventional snare or cone recovery techniques, leading to a failure rate of 7%-19%.4,5 The main factors associated with complicated or unsuccessful retrieval are tilting of the filter, embedded or wall-penetrating retrieval hooks, and prolonged dwell-times.6,7 In particular, engagement of wall-penetrating filters using displacement and modified snare techniques remains the most difficult. 8 When the filters’ proximal retrieval hooks perforate the IVC wall and adhere to surrounding tissues, the situation becomes complicated and is usually solved by open surgical removal with longitudinal cavotomy, clamping, and repair. 9
In December 2017, our center started using a retroperitoneal laparoscopic approach for complicated IVC filters retrieval when filters’ proximal retrieval hooks penetrated the posterior lateral wall of the IVC. This study aims to review our initial experience with this technique for removing wall-penetrating IVC filters after endovascular techniques have failed.
Patients and Methods
Patients
A retrospective review was performed on 8 patients who underwent retroperitoneal laparoscopic-assisted retrieval of wall-penetrating IVC filters at Beijing Jishuitan Hospital between November 2017 and November 2019. The study was approved by the ethics committee of Beijing Jishuitan Hospital and written informed consent was received from all patients before the surgery. Patient demographics, medical histories, medical imaging studies, and procedure notes were reviewed. Most of the patients had no symptoms except for 1 who had low back pain due to a retroperitoneal hematoma. The malpositioning of the filter was the main indication for retrieval in order to avoid long-term complications. All patients had previously experienced at least 1 failure with endovascular retrieval with several instruments, including standard snares, guidewires, and endobronchial forceps. These patients had received follow-up for at least 12 months in the outpatient clinic to assess for delayed complications.
The filters were slanted and the proximal retrieval hooks penetrated the posterior lateral wall of the IVC in all patients on computed tomography (CT) (Figure 1). The positions of the IVC filters were classified as suprarenal in 2 cases, infrarenal in 2 cases, and renal in 4 cases, according to the relationship between the filter and the renal vein.
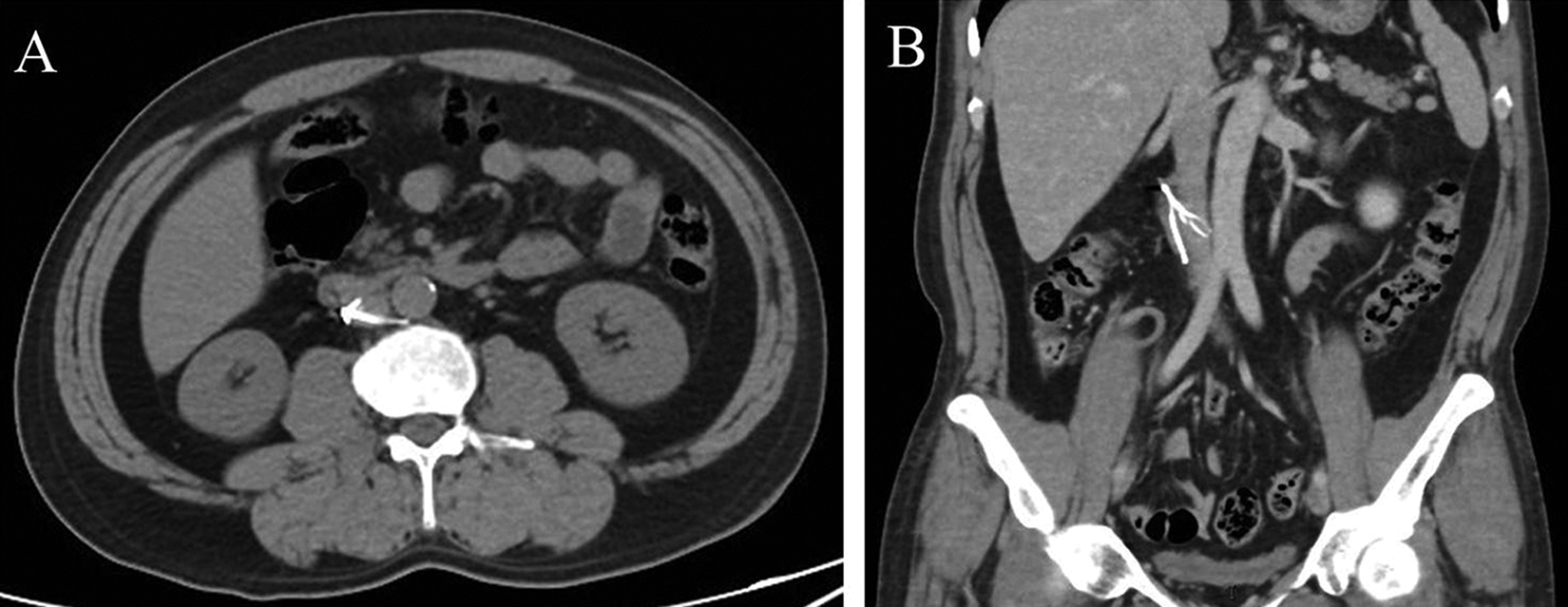
The Computed Tomography (CT) scan showed the filter’s proximal retrieval hook penetrating the posterior lateral wall of IVC. A, Axial CT image; B, Coronal CT image.
Surgical Procedure
All surgeries were performed by the same team, which was headed by a professor of urology and a professor of vascular surgery. The surgical technique was derived from a combination of retroperitoneal laparoscopic partial nephrectomy with traditional endovascular snare techniques.10,11 The patient was placed in the left lateral flank position under general anesthesia, and the procedure was performed using a retroperitoneal approach. The retroperitoneal cavity was formed by blunt dissection and balloon dilation from a small incision located 2 cm above the iliac crest of the midaxillary line. Three trocars were inserted on the right waist between the superior edge of the iliac spine and the inferior border of the rib, after establishment of the retroperitoneal space. For proper exposure of the IVC, the right kidney was laparoscopically mobilized along the anterior surface of the right psoas muscle. The renal artery and vein were cautiously dissected at the renal hilum. The IVC was found along the renal vein and dissected to expose the position of the proximal retrieval hook of the filter penetrating through the posterior lateral vein wall (Figure 2A). The tissue surrounding the filter proximal retrieval hook was usually adhesive and not easy to separate. Therefore, we cut directly into the IVC wall using a longitudinal 2-3 mm incision from the surface of the adhesive tissue using an electrotome needle to clearly expose the proximal retrieval hook (Figure 2B). The small amount of bleeding from the minimal IVC incision was usually controllable, and lumbar vein or renal vein occlusion was performed only when necessary. The filter was then retrieved using a gooseneck snare placed through the trocar port (Figure 2C and D). Finally, the IVC was sutured quickly with 5-0 prolene without active bleeding, and the abdominal incisions were then sutured with retroperitoneal drainage.
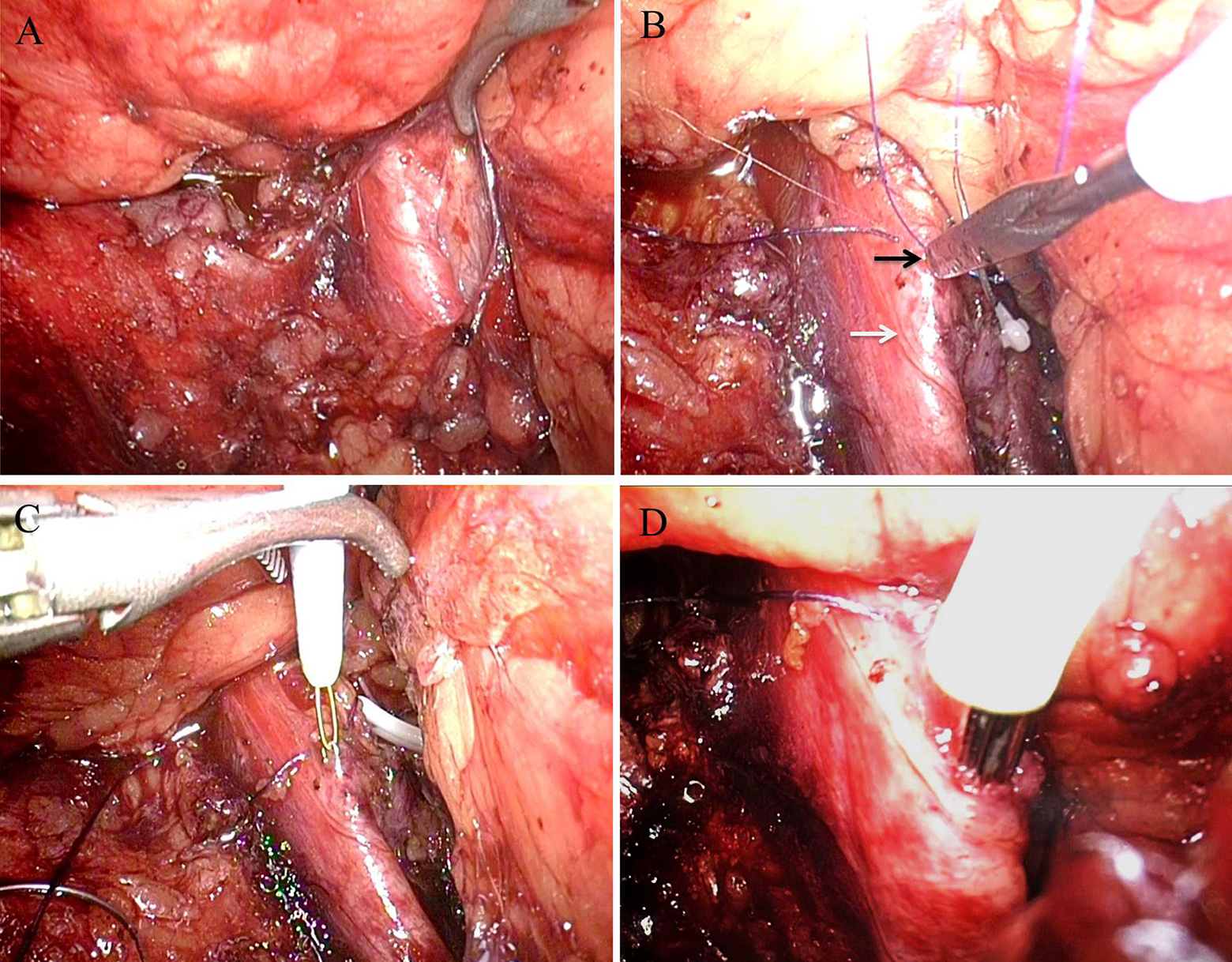
The key procedures in the retroperitoneal laparoscopic approach for filter retrieval. A, The IVC was found along the renal vein and then dissected. B, The IVC wall was cut with a longitudinal 2-3 mm incision from the surface of the adhesive tissue by an electrotome needle to clearly expose the proximal retrieval hook (white arrow: IVC; black arrow: the proximal retrieval hook). C, The proximal retrieval hook was exposed and seized by the gooseneck snare. D, The wall-penetrating filter was hauled out of the IVC and retrieved through the trocar port.
Follow-Up
All patients were administered subcutaneous heparin or oral rivaroxaban tablets 24 to 48 hours postoperatively, depending on coagulation markers. Postoperative complications were observed and recorded. All patients were followed up for at least 1 year with Doppler ultrasound to confirm the presence or absence of DVT of the lower limb.
Statistical Analysis
All statistical analyzes were performed using the SPSS statistical software (SPSS for Windows, version 22.0). Continuous variables are presented as mean ± standard deviation (mean ± SD). Qualitative variables were expressed as frequencies with percentages.
Results
Patient Characteristics
Baseline patient characteristics and preoperative variables are included in Table 1. In our series, the mean age of patients was 45.6 ± 10.7 years. The reasons for IVC filter placement were DVT in 6 cases and pulmonary embolism in 2 cases. The mean indwelling time was 2.4 ± 1.0 years, which indicated the complicacy for retrieval. Before the retroperitoneal laparoscopic approach, different vascular surgeons attempted retrieval of all of the IVC filters using various endovascular techniques, including standard snares, guidewires, and endobronchial forceps, with an average number of retrievals of 2.3 ± 0.8. Unfortunately, all endovascular treatments failed.
Patients’ Characteristics and Preoperative Variables.
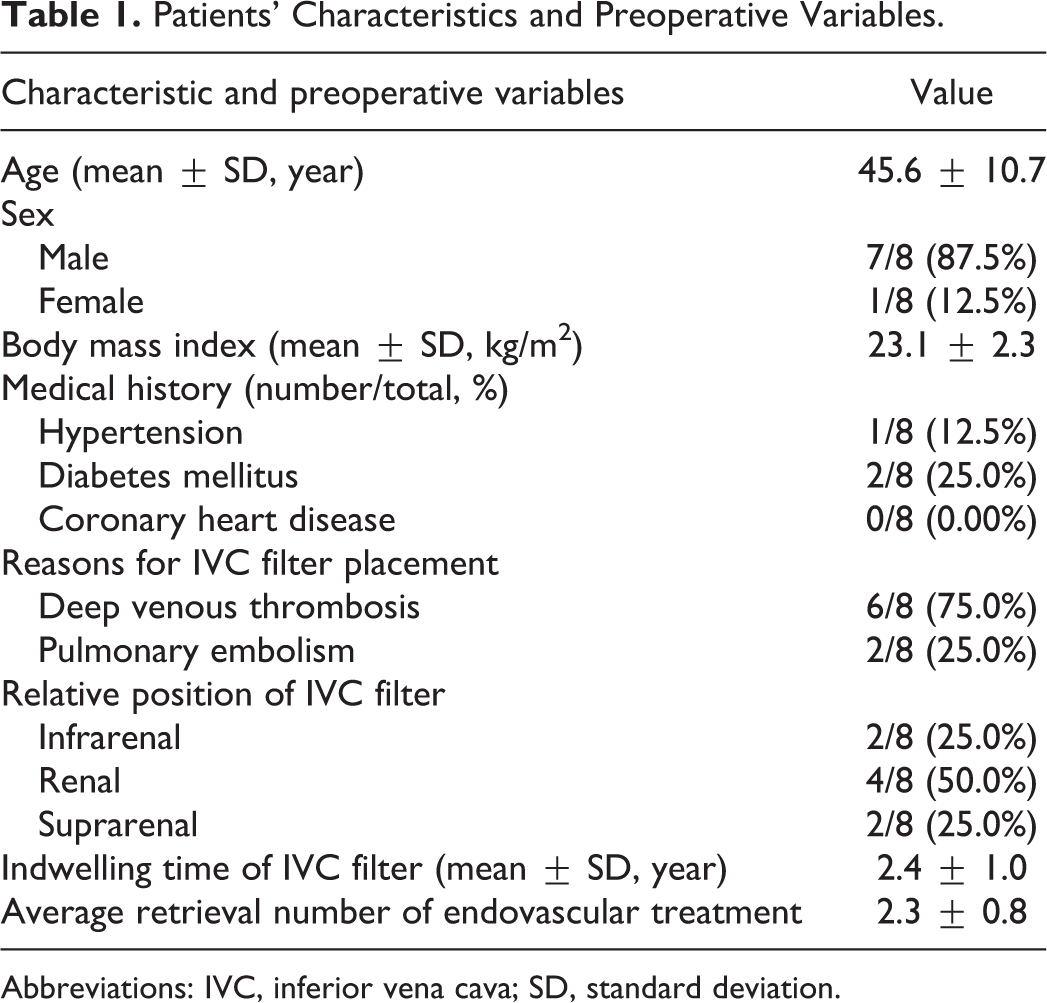
Abbreviations: IVC, inferior vena cava; SD, standard deviation.
Treatment Effectiveness
All patients underwent the retroperitoneal laparoscopic-assisted approach for wall-penetrating IVC filter retrieval without any conversion to open surgery. Postoperative complications and follow-up results are shown in Table 2. The mean surgery time was 53.6 min, estimated blood loss was 45.0 ml, and median hospital stay time was 6.4 days. Three patients experienced postoperative complications with Clavien grades I-II, including fever, hematuria, and moderate pain. No serious complication occurred perioperatively. The median follow-up time was 15.1 months. After IVC filter retrieval, all patients had no DVT recurrence and were satisfied with the surgical results.
Perioperative Results, Postoperative Complications and Follow Up Results.
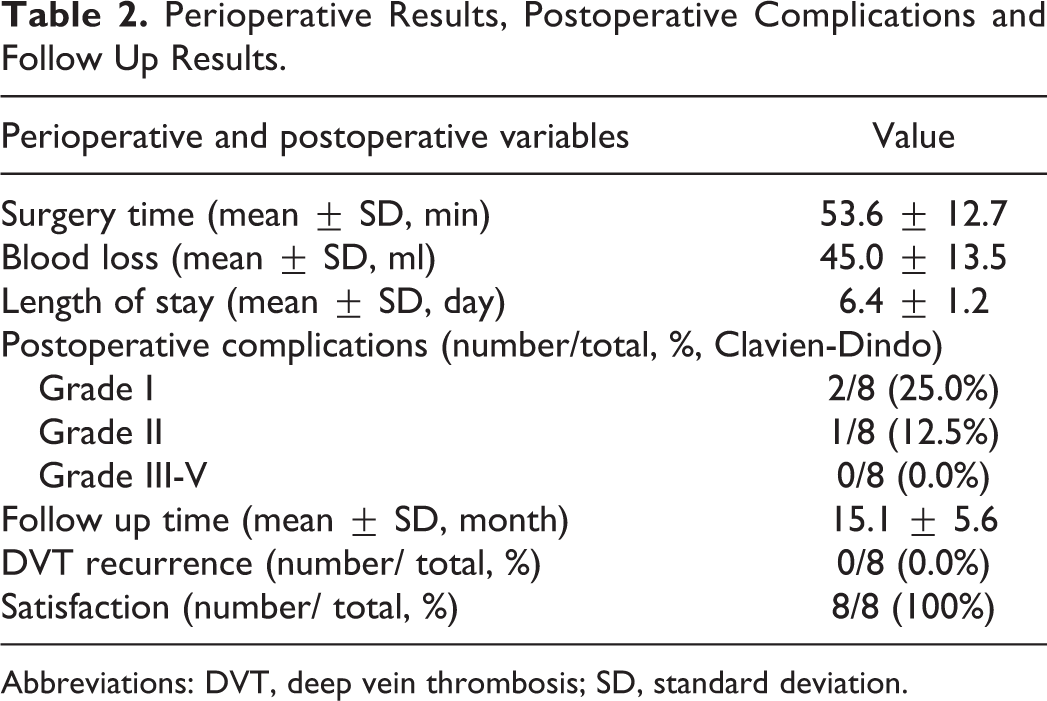
Abbreviations: DVT, deep vein thrombosis; SD, standard deviation.
Discussion
Since the early 2000s, the introduction of retrievable IVC filters has significantly increased their use as safe and effective temporary implants to prevent venous thromboembolism. 12 However, the long-term complications of indwelling IVC filters, such as in-filter thrombus formation, filter fracture, migration, and IVC perforation, alter the risk-benefit calculus of IVCF placement. 2 Although FDA advisories in 2010 emphasized the risk of the adverse events of retrievable filters after long-term placement, IVC filter retrieval rates remain low and are estimated to be around 12% to 45%.13,14 One reason is that sufficient attention has not been paid to patients with IVC filters. A retrospective survey demonstrated that 79% of patients were not aware of the long-term risks of indwelling IVC filters, and 78% were unaware of the importance of filter retrieval. 14 The authors concluded that patient education and regular planned follow-up could significantly increase the successful filter retrieval rate from 23% to 45%. 14
Another reason for low IVC filter retrieval rate is the filter itself. The main factors associated with complicated or unsuccessful retrieval are tilting of the filter and embedding or wall penetration of the filter hook, with prolonged dwell-times. 7 A wide variety of advanced techniques, including the use of angioplasty balloons, additional snares, guidewires, endobronchial forceps, and endovascular laser, can be used to retrieve embedded or wall-penetrating IVC filters when standard retrieval techniques fail. 15 However, these techniques have various technical success rates and complication rates, some of which are partly related to operator preference, experience, and prior success.16-18 Once endovascular techniques fail at retrieving wall-penetrating IVC filter, the filters may be retained with a risk of IVC perforation and injury to adjacent structures (aorta, duodenum, and pancreas). Recently, instead of open surgical methods, some scholars have reported the transperitoneal approach using laparoscopic or robot-assisted laparoscopic techniques for retrieval of partial IVC filters penetrating the anterior wall of the IVC.19-21 Although the transperitoneal laparoscopic technique is more minimally invasive than open surgery, difficulty remains in retrieving penetrating filters in the posterior lateral wall of the IVC.
In the present study, we first reported our initial clinical outcome with the retroperitoneal laparoscopic approach in retrieving filters with proximal retrieval hooks penetrating the posterior lateral wall of the IVC. All patients underwent the procedure successfully, without any severe complications. The patients were followed up for a mean of 15.1 months without suffering DVT recurrence. There are 3 key points that make this approach efficient. First, the operator needs to identify whether the position of the proximal retrieval hook is located in the posterior lateral wall of the IVC, according to the CT images. Second, the kidney should be fully dissociated to create ample space for exposure of the proximal retrieval hook of the filter. Finally, according to our experience, the adhesive tissue embracing the proximal retrieval hook does not need to be skeletonized to avoid bleeding exudation. Three patients experienced postoperative complications with Clavien grades I-II, which showed that this approach is safe as an alternative method for wall-penetrating IVC filter retrieval.
Although the intentional placement of an IVC filter in an infrarenal position is normal for retrieval, filter migration will occur with an overall rate of 11%. 22 Limited data describe how positional changes affect the success of complicated filter retrieval. Gotra reported that positional parameters such as lower mean tilt, caudal migration, and less caval wall penetration were positive predictors of successful IVC filter retrieval. 23 However, the differences among suprarenal, infrarenal, and renal positions have not been discussed. Mandel demonstrated that 84% of IVC filters placed in the suprarenal IVC were safely retrieved with no periprocedural complications, following a short indwelling period, in a small series. 24 In our study, the mean indwelling time of the filters was 2.4 ± 1.0 years, and the position of the IVC filters was infrarenal in only 2 cases, which indicated a phenomenon of filter migration and complicacy for retrieval by endovascular techniques. In the retroperitoneal laparoscopic approach, a similar result was observed when the filter migrated to the renal position, as the adhesion of the wall-penetrating IVC wall increased the anatomical difficulty in the renal hilum.
Based on the results available, this procedure should be used in carefully selected patients with the following conditions: multiple endovascular techniques failed to remove the filter, the proximal retrieval hook of the filter penetrates through the posterior lateral wall of the IVC filter, and the filter is displaced close to the renal vein.
Limitations
There were some limitations to our study. First, this was a retrospective analysis that could not show its advantages in comparison with the classical open technique, although we believe that this minimally invasive approach is theoretically better than the open technique. Second, it should be acknowledged that cases selected to be suitable for this technique were made at the operator’s discretion and thus introduces significant selection bias. Third, although the overall success rate of 100% showed an investment trend in our study, the sample size was too small to reflect the real situation in large-scale studies.
Conclusions
The retroperitoneal laparoscopic-assisted approach is a safe and effective method to remove filters with proximal retrieval hooks penetrating the posterior lateral wall of the IVC after endovascular techniques have failed. To some extent, the development of this technique at our institution has increased the success rate of filter removal and improved patient satisfaction.
Footnotes
Authors’ Note
Haidong Wang, and Zhenhua Liu drafted the article and analyzed the data; Xiaofei Zhu gathered the whole data; Haidong Wang, and Jianlong Liu performed the operations; Libo Man revised the article critically. This study was approved by the Ethics Committee of Beijing Jishuitan Hospital.
Acknowledgments
We thank the surgical staff and the nursing team involved in the care of the patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.