
Abstract
Venous aneurysms (VA), particularly superficial femoral VAs (SFVAs), are rare vascular lesions. A 65-year-old woman with a history of pulmonary embolism (PE), treated with tissue plasminogen activator and oral anticoagulation, was admitted to hospital for dyspnea. Enhanced computed tomography showed recurrent PE and right SFVA with a mural thrombus. The SFVA was not identified during the first PE. The PE was not massive and was treated with direct oral anticoagulants. The thrombus in the SFVA caused the PE, and surgical repair was performed to prevent further embolic events. Under general anesthesia, the SFVA was excised, and direct anastomosis was performed. PE recurrence, venous aneurysmal changes, and thrombosis were not noted at the 1-year follow-up.
Introduction
Popliteal vein aneurysms (VAs) below the adductor canal are the most commonly reported lower extremity deep VAs. 1 Altough lower extremity VAs are usually asymptomatic, they can cause pulmonary embolisms. We here reported a case of a middle superficial femoral VA (SFVA), I.e. a rare type of VA, located in the adductor canal which was successfully managed by resection and end-to-end anastomosis. This article was written with the patient’s informed consent and the approval of the institutional review boards.
Case Report
A 65-year-old woman with a history of pulmonary embolism (PE), which had been treated with tissue plasminogen activator and oral anticoagulation 7 years ago, was admitted to hospital for dyspnea. While PE was initially considered to be the result a right popliteal vein thrombosis detected on computed tomography (CT), a later review showed the presence of a central SFVA that had ben overlooked. She did not undergo duplex scanning of the lower limb at the time and medical evaluation excluded thrombophilia and malignancy. Oral anticoagulation was discontinued 1 year after the first PE and the patient was followed up annually. PE recurrence upon anticoagulation therapy withdrawal was not observed for 7 years.
Her enhanced CT showed recurrent bilateral PE and right SFVA, measuring 37 mm in diameter and 46 mm in length, with a mural thrombus. (Figure 1) Direct oral anticoagulant (DOAC) treatment immediately alleviated PE. One month after her PE recurred, CT and duplex scan echoes were repeated. The mural thrombus in the SFVA disappeared after DOAC. A retrospective examination of the previous CT also confirmed presence of the SFVA, which had been originally overlooked. The thrombus in the SFVA was the cause of repeated PE, thus we decided to surgically remove it. The operation was performed under general anesthesia. A skin incision was made inside the sartorius muscle in the right thigh, and the superficial femoral artery (SFA) was identified. The SFVA was located at the dorsal side of the SFA. (Figure 2) End-to-end anastomosis was considered possible by ligation of the branches and adequate dissection of the proximal and distal sides. After heparinization and aneurysm resection, veins without aneurysmal changes were anastomosed end-to-end. (Figure 3)
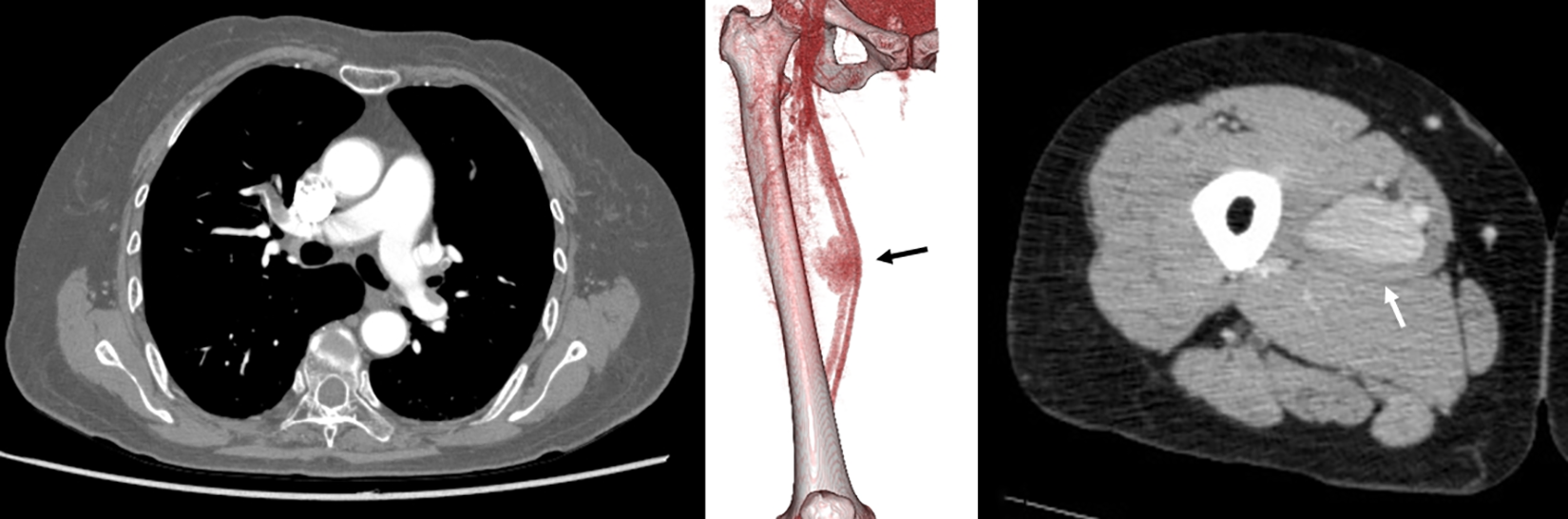
A, chest contrast-enhanced computed tomography showed a bilateral pulmonary artery embolism. B, 3-dimensional image. A superficial femoral vein aneurysm was found in the central part of the right thigh (arrow). The morphology of the venous aneurysm was a saccular aneurysm. C, axial image. The maximum diameter of the venous aneurysm was 37 mm (arrow).
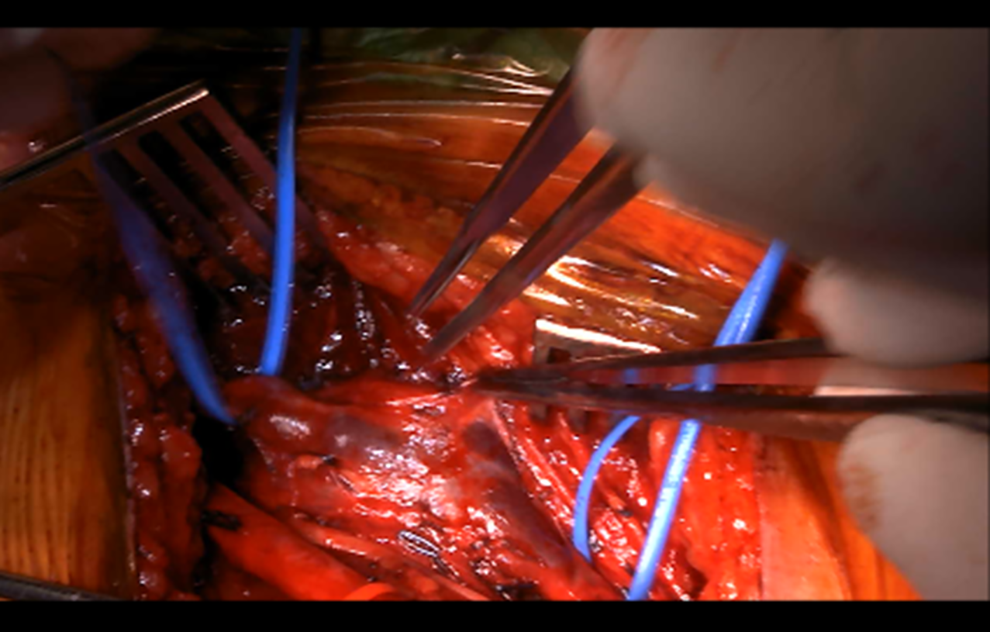
Surgical findings. Saccular aneurysmal change on the right superficial femoral vein. Aneurysm was on the dorsal side.
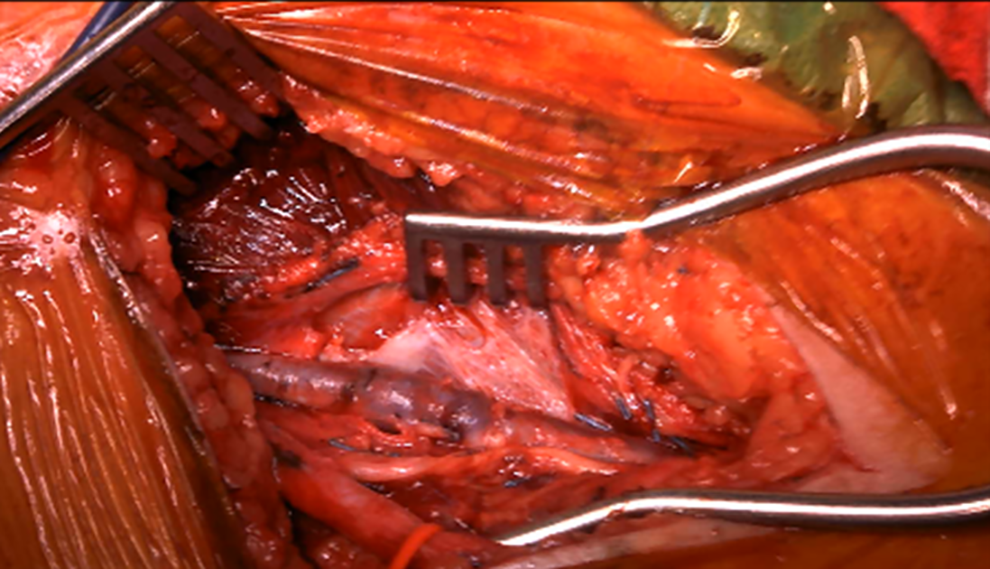
Aneurysm resection and reconstruction of the end-to-end anastomosis.
The patient was discharged without any complications postoperatively. Postoperative anticoagulation was continued to prevent venous thrombus formation. DOAC was maintained for 3 months postoperatively.
Duplex scanning at 1 month and 1 year after the operation confirmed that the SFV was patent without aneurysmal change. (Figure 4)
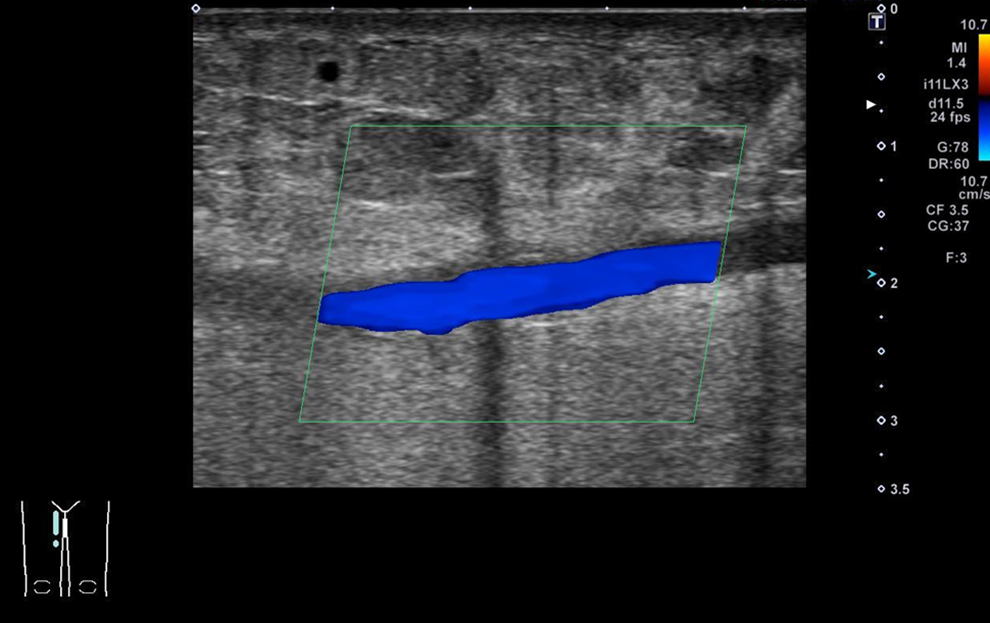
Duplex scanning of patent anastomosed site.
Discussion
The definition of VA remains unclear. Indeed, there is currently no set size or criteria for identifying venous dilations as aneurysms. Nonetheless, incidence rate of 24-32% and 76% have been reported in the literature for VAs with concomitant PE and chronic veous disease associated with VAs, respectively. 1 Similarly, the pathogenesis of VA also remains to be determined. Indeed, trauma, inflammation, congenital venous wall weakness, infection, venous hypertension, and localized degenerative changes have all been suggested as possible causes.1-3
Most VAs of the lower extremity occur in the popliteal vein, with 75% of the cases involving the upper knee segment. 1 Approximately 212 cases of popliteal venous aneurysm (PVA)have been reported in the literature.1,3 Given that the PVA is anatomically located outside of the adductor canal (such as the present case) are rare and only a few cases have been reported.2,4,5 PVA is histologically characterized by a thickened and fibrous intima with markedly decreased smooth muscle cells in the media. This can be thin or absent, it can exhibit different stages, and may or may not have internal elastic lamina.1,6,7 In this present case, pathology showed part of the VA wall to have defective smooth muscle and elastic lamina. (Figure 5) Although our pathological findings suggest either trauma, localized degenerative or congenital anomaly to be the cause of the aneurysmal change, this cannot be clearly determined.
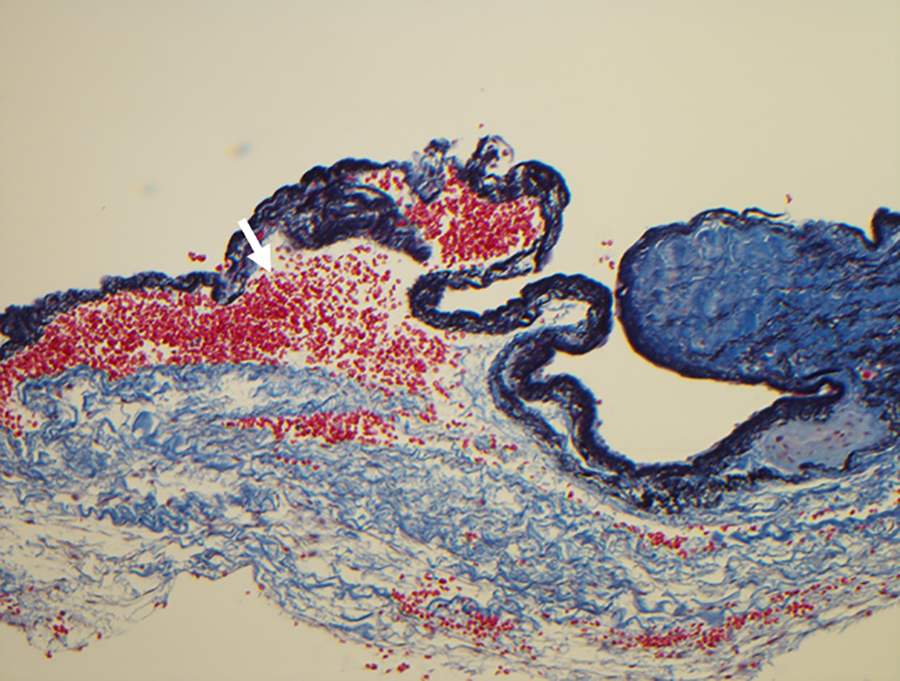
Histological findings of the resected superficial femoral vein aneurysm. The resected specimen was stained with Elastica Masson. Lack of smooth muscle and elastic lamina was observed in part of the vein aneurysm wall (arrow).
Duplex scanning is the preferred diagnostic modality, as it evaluates the VAs in the extremities and detects the thrombus in the VA.1,3,8 Unfortunately, venous duplex scanning was not performed during the first PE event of our patient, and the SFVA was overlooked on CT. Proper testing could have prevented PE recurrence.
Surgical intervention is generally indicated when VA is either an asymptomatic saccular aneurysm or a large (>20 mm) fusiform.1,3 Furthermore, several treatment options have been developed. Tangential aneurysmectomy and lateral venorrhaphy are valid options for treating saccular aneurysms. In contrast, fusiform aneurysms can be treated with resection and end-to-end anastomosis, graft interposition, or ligation of the proximal and distal veins. 2 Cases of recurrence of tangential aneurysmectomy and lateral venorrhaphy or saccular aneurysm have been previously reported. 9 Although, the SFVA here described was a saccular aneurysm, aneurysm resection and end-to-end anastomosis were selected to avoid the risk of recurrence. Another option is endovascular treatment, however, only 1 case of endovenous stent-assisted coil embolization has been reported, and the indication as well as the long-term results, are unknown. 4
While satisfactory patency rates following reconstruction have been reported in the literature, the long-term outcomes are not yet available.1-3,6 However, late thrombosis following the surgical procedure and surgical relapses have been previously reported in the literature (4 and 12%, respectively). 3
Conclusions
Middle SFVA located in the adductor canal is rare. Since the thrombus in the SFVA caused PE, surgical resection was performed.
Footnotes
Authors’ Note
The study was reviewed and approved by the Institutional Review Board (IRB number: 2–31). Conception and Design: YN, MK, Data collection: YN, MK, Writing: YN, Critical review and revision: all authors, Final approval of the article: all authors, Accountability for all aspects of the work: all authors. Informed consent has been obtained from the patient for publication of the case report and accompanying images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.