
Abstract
We report a case of successful percutaneous transhepatic, embolization of an iatrogenic extra-hepatic pseudoaneurysm (PsA) of the right hepatic artery (RHA) under combined fluoroscopic and ultrasonographic guidance. A 73-year-old man underwent percutaneous transhepatic biliary drainage placement in another hospital, complicated by haemobilia and development of a RHA PsA. Endovascular embolization was attempted, resulting in coil embolization of the proper hepatic artery, and persistence of the PsA. At this point, the patient was referred to our hospital. Computed tomography and direct angiography confirmed the iatrogenic extra-hepatic PsA of the RHA, refilled by small collaterals from the accessory left hepatic artery (LHA) and coil occlusion of the proper hepatic artery. Attempted selective catheterization of these vessels was unsuccessful due to the tortuosity and very small caliber of the intra-hepatic collaterals, the latter precluding endovascular treatment of the PsA. Percutaneous trans-hepatic combined fluoroscopic and ultrasound-guided embolization of the PsA was performed with Lipiodol® and cyanoacrylate-based glue (Glubran®2). Real time fluoroscopic images and computed tomography confirmed complete occlusion of the pseudoaneurysm. Surgical repair, although feasible, was considered at high risk. In our patient, we decided to perform a percutaneous trans-hepatic combined fluoroscopic and ultrasound-guided embolization of the PsA using a mix of Lipiodol® and Glubran®2 because of the fast polymerization time of the glue allowing the complete occlusion of the PsA in few seconds, thus eliminating the risk of coil migration, reducing the risk of PsA rupture and avoid a difficult surgical repair.
Introduction
Hepatic pseudoaneurysm (PsA) formation is a possible complication of liver biopsies or percutaneous biliary procedures, usually treated by minimally invasive interventional procedures using an endovascular and/or percutaneous trans-hepatic approach.1-4 We present a case of successful percutaneous trans-hepatic embolization of an iatrogenic extra-hepatic PsA of the right hepatic artery (RHA) in a patient with previous occlusion of the proper hepatic artery (PHA) using a mixture of Lipiodol® (Guerbet, Roissy, France) and cyanoacrylate-based glue (Glubran®2) (GEM, Italy) under combined fluoroscopic and ultrasonographic guidance.
Methods
A 73-year-old man known to suffer from autoimmune cholangitis underwent percutaneous transhepatic biliary drainage in another hospital, after several presentations with fever and jaundice associated with elevation of serum alkaline phosphatase and total bilirubin. A few days after his discharge from hospital, the patient was re-admitted with fever and haemobilia. Computed tomography showed an iatrogenic extra-hepatic PsA of the RHA. Endovascular embolization was attempted resulting in coil embolization of the proper hepatic artery (PHA) without occlusion of the PsA lumen. The patient was referred to our hospital. Computed tomography confirmed the occlusion of the PHA and the persistence of the iatrogenic PsA (27 mm diameter in the axial plane) in the extra-hepatic portion of the RHA (Figure 1
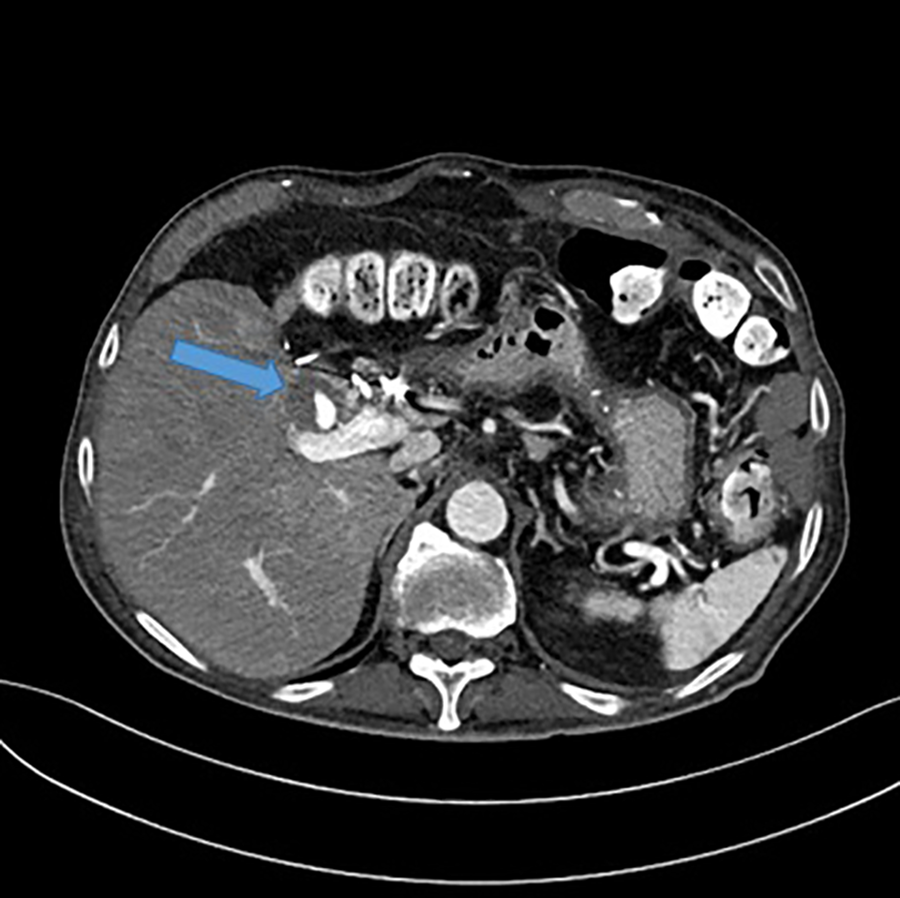
CT showing the iatrogenic PsA (27 mm diameter in the axial plane) in the extra-hepatic portion of the RHA.
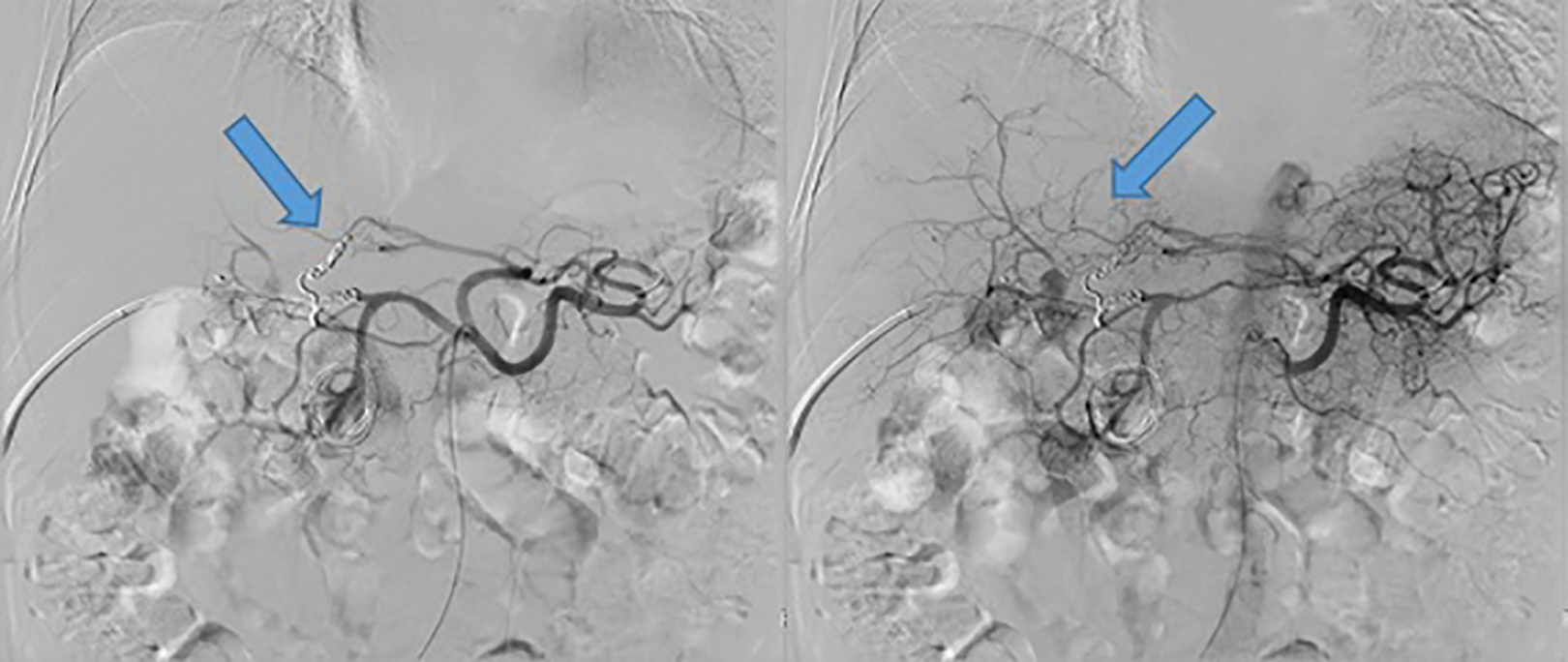
Celiac axis arteriography confirmed the occlusion of the PHA, and the persistence of the RHA PsA multiple small collaterals from the accessory left hepatic artery refilling the RHA branches and the PsA.
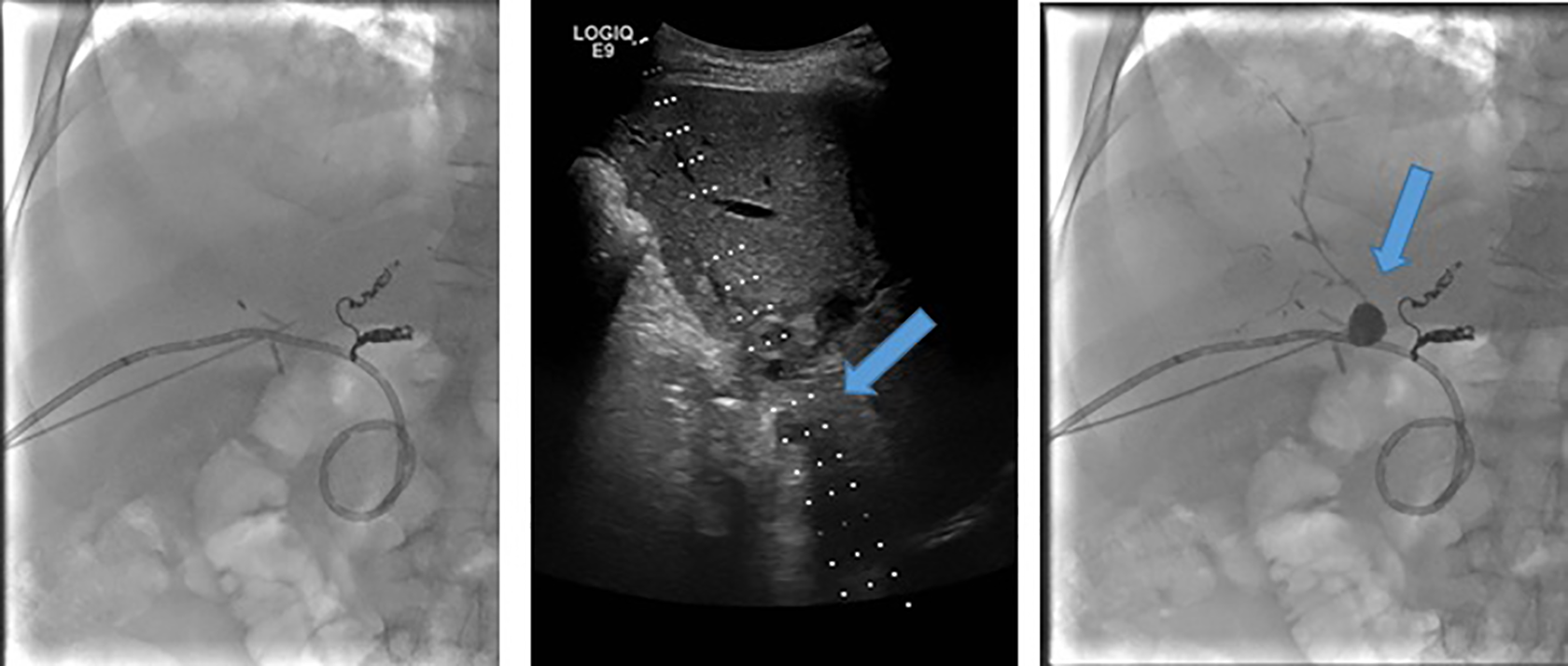
Percutaneous trans-hepatic puncture of the PsA, with an 18-gauge needle, under ultrasound and fluoroscopic guidance.
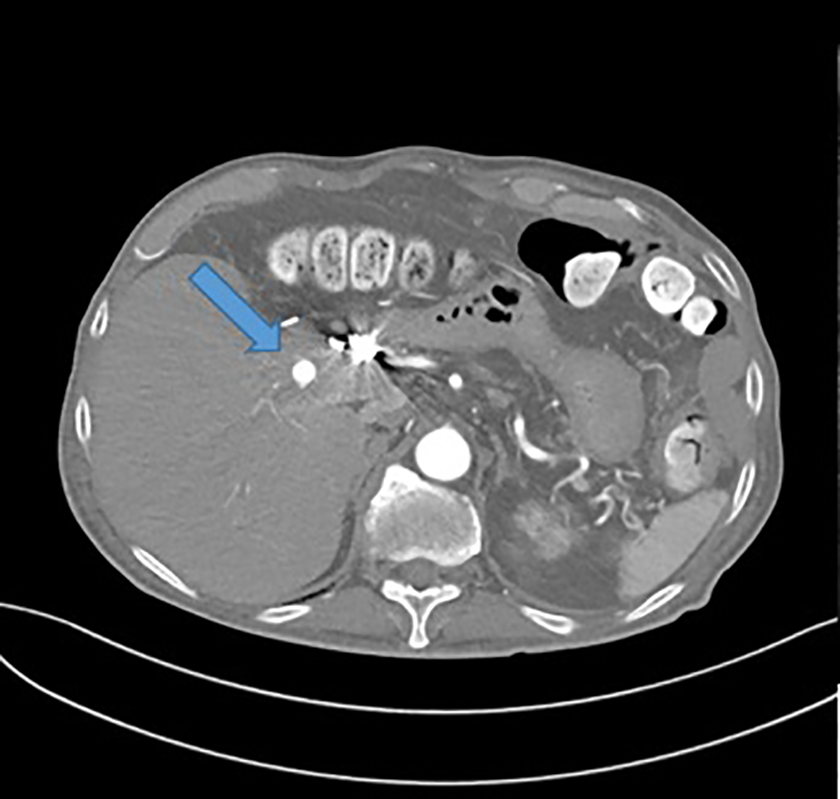
CT scan after the procedure, showed the complete occlusion of the pseudoaneurysm.
Discussion
Hepatic artery PsA is an uncommon but potentially lethal complication of hepatic, biliary, and pancreatic interventions. 7 Major complications associated with biliary procedures are reported in 5–7% of cases with arterial bleeding reported in approximately 2% of cases resulting in most cases in haemobilia. 8 The endovascular approach is usually the initial choice of treatment of a PsA, 9 however, in our patient, this was impossible because of the previous occlusion of the PHA.
Surgical intervention with ligation of the bleeding vessel is considered for unstable patients and when embolization fails or is not feasible. A low number of blood transfusions required prior to angiography was associated with better survival, which may simply reflect hemodynamic stability from a less severe pseudoaneurysmal rupture. 10
Percutaneous transhepatic PsA embolization, using a cyanoacrylate-based glue or coils, has already been described in the literature for intra-hepatic PsA1,2,3; in our case the technique was effective also in an extra-hepatic PsA, the latter having a major risk of rupture and consequent hemoperitoneum when compared to intra-hepatic PsA. In our patient, we decided to perform the embolization using a mix of Lipiodol® and Glubran®2. Coils could also be used, 10 however, we decided to use a mix of Lipiodol® and Glubran®2 because of the fast polymerization time of the glue allowing the complete occlusion of the PsA in few seconds, thus eliminating the risk of coil migration, reducing the risk of PsA rupture and avoid a difficult surgical repair.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Informed consent has been obtained from the patient (or patient’s family/guardian*) for publication of the case report and accompanying images.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.