
Abstract
Purpose:
The objective of this study was to evaluate the primary and assisted secondary percutaneous and non-invasive technical success of the ProGlide device on all-comers in a consecutive case series of percutaneous endovascular aortic aneurysm repair (P-EVAR).
Method:
A single-center consecutive case series where 434 elective and acute P-EVAR procedures were registered prospectively between May 2011 and July 2017. The mean age was 74.5 years ± SD 11.4 years. 82.3% of the patients were male. All patients were pre-planned from CT angiography. Percutaneous access punctures, performed in local anesthesia in the common femoral artery, with a final introducer size between 12-22 Fr OD were included and stratified in 2 groups, 12-16 Fr and 17-22 Fr.
Results:
By screening 868 access groins 22 groins were excluded. Of the remaining 846 groins, intended to be treated with ProGlide, 9 groins were excluded peri-procedurally and treated with the Fascia Suture Technique or surgical cutdown. The remaining 837 groins had access closure with ProGlide, with a mean value of 2.15 devices per groin with a slight significant difference between the 2 stratification groups. Primary ProGlide technical success was achieved in 68.1% of the groins. Secondary percutaneous or non-invasive technical success was achieved in 96.9%. Here there was no statistically significant difference between the 2 stratification groups. Thirty-one (3.7%) groin complications were registered during 30-day follow-up and 17 required additional treatment. Total mortality was 2.8%. None of these deaths were related to the access site.
Conclusion:
ProGlide by itself has a significant failure rate in the closure of large-bore access holes on an unselected cohort of patients eligible for P-EVAR. However, together with adjunct percutaneous or non-invasive methods a success rate of 97% can be achieved. The access complication rate was lower than 4% at 30-day follow-up.
Keywords
Introduction
Vascular access in the groin for large-bore catheters (12-22 Fr) has historically been performed through a cutdown. This was advantages because it provided direct visualization of the common femoral artery (CFA) and hemostasis could be confirmed before access site closure.
However, some complications can occur with an open surgical procedure, such as wound infection and seroma and lymphocele formation. This can prolong the hospital stay and lead to higher costs. Percutaneous endovascular aortic aneurysm repair (P-EVAR) has emerged with less wound complications, shorter hospital stays and substantially reduced costs.1,2 The suture-mediated closure device (SMCD), Prostar and Perclose ProGlide (ProGlide) (Abbott Vascular, IL, USA), have both shown efficacy and safety in closure of large-bore access holes (LBAH) in addition to being less invasive, quicker and with reduced incidence of access related complications than open surgery.2-7
In a systematic review an overall success rate of 92% was achieved for SMCD. 8 However, in many studies patients with heavy femoral artery calcification had been excluded. Other exclusion criteria were femoral artery aneurysms, scarred groins and obesity.8,9
The objective of this study was to evaluate the primary and assisted secondary technical success of the ProGlide device on all-comers in a consecutive case series of P-EVAR.
Materials and Methods
All P-EVAR procedures at a Regional Vascular and Endovascular Center were registered prospectively between May 2011 and July 2017. 434 patients with a mean age of 74.5 years (± SD 11.4) and 82.3% male were included. 95.9% were elective cases.
All groins were included except 22 groins with small-bore access (OD < 12 Fr), primary need for cutdown due to planned thrombendarterectomy, bypass surgery, procedural hematoma, when protocol was violated or due to organizational error.
Access sites were stratified into 2 groups. Group 1 with OD 12-16 Fr and group 2 with an OD 17-22 Fr. Access sites with OD of 17 Fr corresponds to the size of the Nellix EndoVascular Aortic Sealing System (Endologix Inc., Irvine, CA, USA), which was the smallest diameter for placement of a main body in our study.
Eligibility for primary treatment with ProGlide was considered from pre-operative CT angiography. Access puncture was performed under local anesthesia using a standard J-tip 0.035” guidewire in the CFA. Ultrasound guided puncture was implemented during the study period. Arterial puncture site was intended to avoid calcified plaques as well as puncture in the superficial and deep femoral artery or above the inguinal ligament. All punctures were performed or supervised by experienced interventionalists.
Endoprosthesis
Patients were treated with endovascular stentgrafts from Medtronic Endurant II (Medtronic, Minneapolis, MN, USA), Gore Excluder (W.L Gore & Associates, Flagstaff, AZ, USA) and Nellix and Ovation (Endologix Inc., Irvine, CA, USA).
Closure Devices and Methods
Percutaneous
ProGlide is a 6 Fr SMCD and was used in this study. The devices were deployed using a “Pre-close technique” according to the instructions for use (IFU). Two ProGlide sutures were used in each access hole placed at an angle of 30-45 degrees, medial and lateral to the median line. If pre-placement of a ProGlide suture failed, for example by suture breakage or tearing through the tissue, additional ProGlide suture(s) were placed. After completion of the EVAR procedure the large-bore sheath was removed and the pre-placed ProGlide sutures were tightened to obtain hemostasis. The number of ProGlide device per access site were counted and use of adjunct procedures was documented.
Angio-Seal (TERUMO International Systems, Tokyo, Japan) is a 6-8 Fr device with a plastic anchor on the inside of the vessel and a collagen plug outside the wall that is tightened over a suture toward the plastic anchor when the ProGlide sutures failed to close the puncture site.
Non-invasive
HemCon® Patch (Pro-tricol Biomedical, OR, USA) is a collagen patch that is placed on the skin over the puncture hole with an adhesive surface. Sometimes it was used together with a surgical clamp placed on the remaining ProGlide suture to increase the compression against the vessel for 30 minutes before removal. Manual compression was standardized to a minimum of 15 minutes and FemoStop™ II Plus (St. Jude Medical, Mn, USA) is a device with a band around the patient´s waist with an inflatable transparent plastic dome mounted on a rigid plastic platform. With the help of a manometer the pressure was controlled and successively reduced for at least 30 minutes.
Surgical
The Fascia Suture Technique is an open method that closes the hole of the femoral fascia, which is located just in front of the CFA. 10 Cutdown is a standard surgical approach of the CFA.
Endpoints
This study was focused on efficiency and safety of the ProGlide device. The efficacy endpoints were primary ProGlide technical success and with or without assisted secondary percutaneous or non-invasive methods. Primary ProGlide technical success was defined as hemostasis without the use of any assisted percutaneous, non-invasive or open surgical method at the completion of the procedure. Secondary technical success was defined as hemostasis after the use of one or more adjunct procedures without the use of surgical methods.
The safety endpoint was freedom from early access complications while the patient was admitted and late access complications after discharge.
Data on demographics, procedural details and complications were collected from our internal AAA Quality Control Registry. Data were entered both prospectively and retrospectively. Late 30-day complications were recorded from the follow-up CT angiography and/or our internal AAA Quality Control Registry. Data was then de-identified and made anonymous before this data aggregate was used to write this ProGlide article.
Ethics
The Data Protection Officer (DPO) at our Regional Center has approved the use of this de-identified and anonymous data aggregate to organize the ProGlide study data and publish the results. And therefore we were not required to obtain Regional Ethics Committee (REC) approval.
Statistical Analysis
Continuous variables were expressed as means ± SD, and comparisons between the 2 groups were made by the Mann-Whitney-U test. Categorial variables were expressed as numbers and percentages and comparisons between the groups were done using Pearson Chi-squared test. SPSS software (version 25.0) was used for the statistical analysis. Statistical significance was defined as P < 0.050.
Results were Analyzed Per Protocol.
Results
In the trial Consort flow diagram (Figure 1) patient enrollment, exclusion and outcome is summarized. Of 434 screened patients (868 groins), 22 groins (2.5%) were excluded due to small-bore access with an OD < 12 Fr (n = 10), primary need for cutdown due to planned thrombendarterectomy, bypass surgery or procedural hematoma (n = 7), procedural violation or organizational error (n = 5).
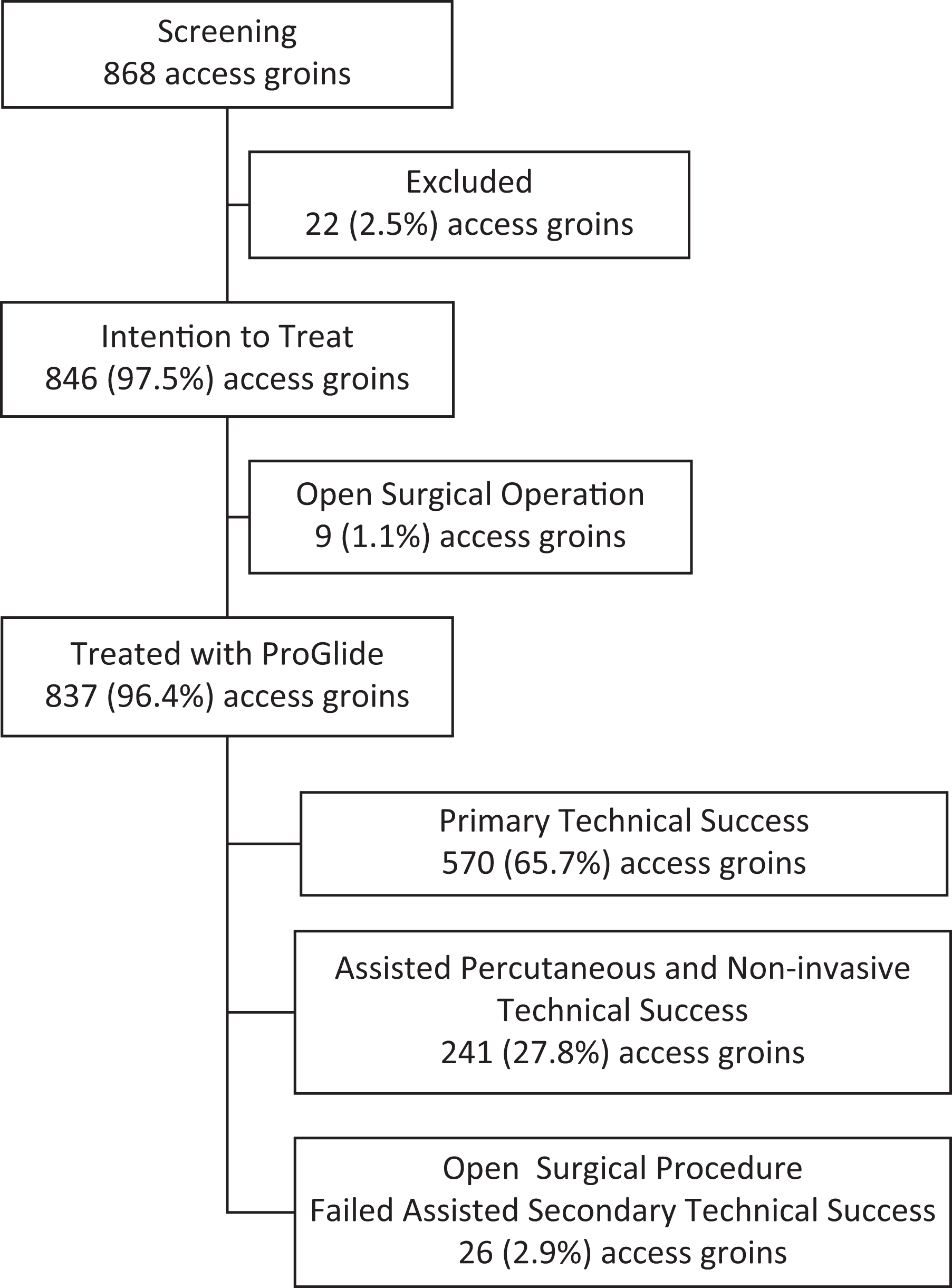
CONSORT Diagram showing flow through the access closure procedure.
Of the remaining 846 groins (97.5%), intended to be treated with ProGlide, 9 groins were excluded peri-procedurally on the discretion of the operator due to unstable rupture (n = 4), calcification (n = 3) and scar tissue (n = 2). In these cases, 5 groins were treated with the Fascia Suture Technique and 4 with surgical cutdown.
The remaining 837 groins (96.4%) where treated with ProGlide. There was no statistically significant difference between the 2 stratification groups regarding either primary ProGlide technical success (P = 0.063) or assisted secondary percutaneous and non-invasive technical success with ProGlide (P = 0.103, Table 1).
Primary and Secondary Technical Success.
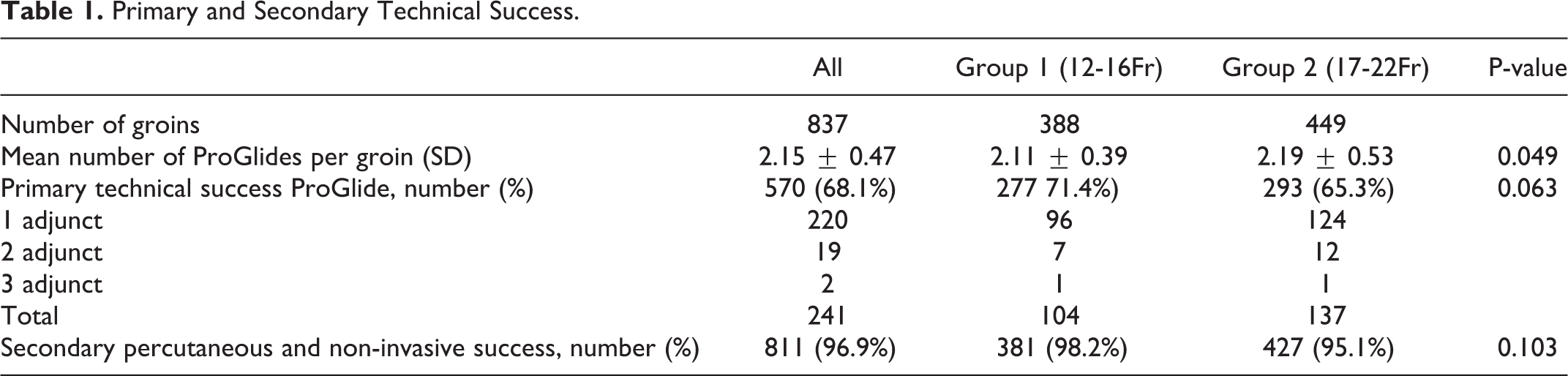
A numerically small, but statistically significant, difference in the mean number of ProGlide devices used in each groin was detected between the 2 stratification groups (Table 1).
The Primary ProGlide technical success was 68.1% for the total cohort, with no statistically significant difference between the stratification group 1 (71.4%) and 2 (65.3%) (Table 1). Secondary percutaneous and non-invasive technical success was 96.9% for the total cohort and with no statistically significant difference between the 2 stratification groups.
In total 264 adjunct procedures were used in 241 groins. AngioSeal was the most commonly used single adjunct device (n = 173).
Failure to obtain primary or secondary technical success occurred in 26 groins. Those groins were treated with the Fascia Suture Technique (n = 8), surgical cutdown (n = 16) or a combination of both (n = 2).
Thirty-one complications out of 837 groins (3.7%) were registered. Sixteen of them occurred while the patient was admitted (early complications) and 15 occurred after discharge (late complications), thus 96.3% of the groins were complication-free at 30-day follow-up. There were no statistically significant differences in frequency of complications between the 2 stratification groups (p = 0.096, Table 2).
ProGlide Complications.
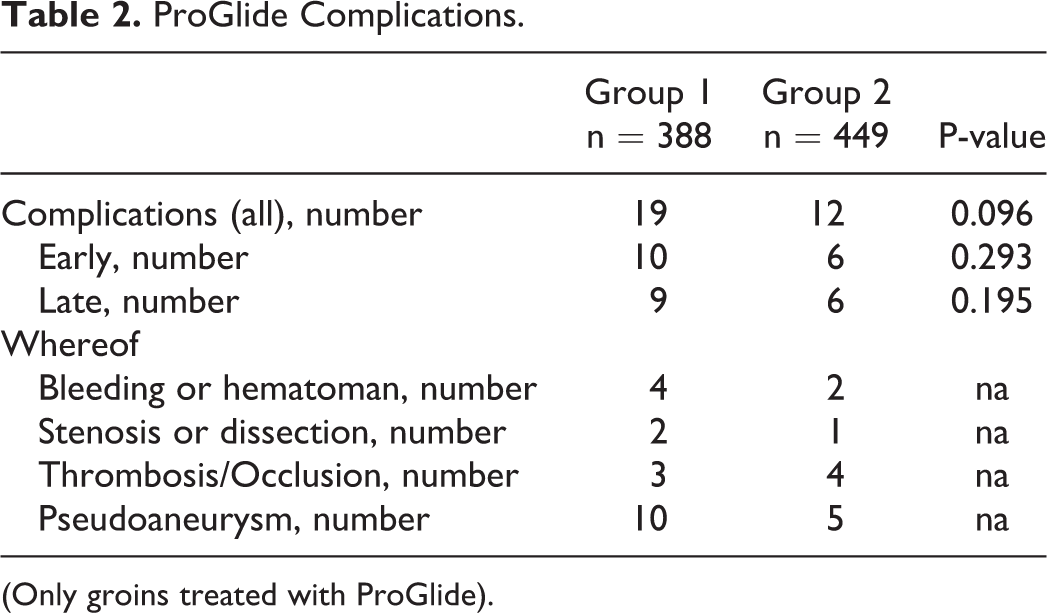
(Only groins treated with ProGlide).
Treatment of Complications
Seventeen groin complications required treatment, whereof 11 were in stratification group 1 and 6 in stratification group 2. In stratification group 1, there were 9 early complications requiring treatment: 3 groins with bleeding required external compression and 1 a cutdown. Three groins with thrombosis/occlusion were treated with cutdown. Two pseudoaneurysm required ultrasound guided thrombin-injection. Two late complications with pseudoaneurysms also required ultrasound guided thrombin-injection.
Stratification group 2 had 6 early complications: 2 bleeding groins where 1 was treated with external compression and the other with the Fascia Suture Technique. The other 4 were thrombosed and occluded and were treated with a cutdown.
Pseudoaneurysm and hematoma predominated in stratification groups 1, while pseudoaneurysm and thrombosis/occlusion dominated in stratification group 2.
Mortality
Total patient mortality was 2.8% (12/434). One patient was primarily excluded due to extremely calcified AFS and treated primarily with a bilateral surgical cutdown. Of the remaining 11 patients treated with a ProGlide, 2.07% (9/434) were early mortality within 30-days while admitted. Five of these patients were rAAA. 0.46% (2/434) were late mortality after 30-days while admitted due to other causes. None of these deaths were related to the ProGlide device or the EVAR procedure.
Discussion
This study shows that it is possible to attain closure of LBAH after P-EVAR for AAA by using the ProGlide closure device itself or together with adjunct procedures. Our primary technical success, with ProGlide itself of 68.1% is lower than has been reported in most of the trials where primary technical success rates for ProGlide have varied from 71-100% after P-EVAR.11-13 One explanation could be that this study intended to treat all-comers and have not excluded factors that have been associated with failure in other studies. Another likely explanation is that the definition of technical success differs between publications. The purpose of this study was to evaluate what can be achieved with the ProGlide device itself. One can argue that adjunct non-invasive procedures like HemCon Patch, FemoStop or manual compression are not significant procedures. However, they represent methods that facilitate hemostasis and therefore should be considered as adjunct procedures and be included just in the group of assisted secondary technical successes. We believe that this definition gives a fair picture of what the ProGlide technology alone can offer. We thus challenge the thinking behind the ProGlide that one or a couple of sutures through the arterial wall are enough to secure hemostasis. The results indicate that this only applies in two-thirds of the cases.
Proficiency level has been described as an independent factor for outcome.14,15 Our Regional Vascular and Endovascular Center is a high-volume center for endovascular aortic repair. The procedures are performed by a team of a few interventional radiologists and vascular surgeons, which gives every physician a good opportunity to fulfill the learning curve that is recommended by the manufacturers. For ProGlide, 30-40 cases has been considered as a sufficient number to become a proficient user.3,15 A strength in our series is that it represents many patients treated by a few physicians and probably what one can optimally achieve with this method. A weakness on the other hand, by keeping the procedure only on experienced hands, is that the learning curve will have a lesser impact on the primary and secondary technical success rates rather than from world data with expected worse results.
We have chosen to place 2 ProGlide devices per puncture site as pre-suturing which has been expected to provide technical success. This follows the IFU from the manufacturer. In case of bleeding we have used an AngioSeal device instead of an additional ProGlide device. The procedure has then been defined as a primary technical failure. 16
Based on our results with a low primary success rate for ProGlide itself one might consider that a standard procedure could be a combination of ProGlide and another closure device. A combination of ProGlide and AngioSeal devices could be an alternative and has been reported.17,18
Ultrasound assisted puncture is now highly recommended to achieve an optimal puncture site. 19 A disadvantage with our study, that started in 2011, is that we were unable to use ultrasound in early stages of the study.
This may have affected the outcome negatively. Some publications also advocate the use of micro-puncture technique which we have not adopted.20-22
We have used the Fascia Suture Technique in addition to traditional surgical cutdown as a “bail-out” procedure when the percutaneous options have failed.10,14,23,24 An advantage with the Fascia Suture Technique, in comparison to surgical cutdown, is that it is less invasive. It has also shown complication rates24,25 equivalent to the SMCD device Prostar (Abbott Vascular, IL, USA). 23
Unstable ruptured aneurysms were excluded peri-procedurally due to the necessity of pre-suturing of the ProGlide device. The method has a clear disadvantage in an acute setting as it will prolong the time until the ruptured aneurysm can be excluded.26,27
In our study we did not gather anatomical information about the CFA, such as diameter and degree of calcification. Therefore, we cannot conclude if these factors are predictors for failure.
In regard to the two stratification groups, we found no statistically significant differences in the technical outcome nor complication rates. Our results support that the size of the puncture hole does not play a significant role. Other circumstances such as the localization of the access hole and the ProGlide needles in relation to calcified plaques in the vessel wall can play a role. Side punctures giving awkward needle positions may be another factor. This may explain why the ProGlide device by itself may prove insufficient, but in combination with other adjunct procedures seems to work well.
A complication rate of 3.7% can be considered an acceptable level at 30-day follow-up. This is especially true when calcified vessels were not excluded.
Analysis Per Protocol was practiced in that we analyzed the success or failure of the ProGlide device and not patients morbidity and mortality.
Time and costs are important factors when comparing different closure techniques. Regretfully, our study was not structured in such a way that we could analyze and report the cost/benefit results. These variables are especially of interest if technical outcomes are equivalent. Also a randomized trial comparing different percutaneous closure devices for LBAH would be very desirable.
Conclusion
ProGlide by itself has a significant failure rate in the closure of LBAH on an unselected cohort of patients eligible for P-EVAR. However, together with adjunct percutaneous and non-invasive procedures a success rate of 96% or higher can be achieved and with no statistical difference between the 2 stratification groups. An access complication rate lower than 4% at 30-day follow-up is acceptable. Even though the ProGlide device is not an optimal method for closure of all groin puncture holes, in general, this study strongly supports that percutaneous P-EVAR procedures followed by the use of percutaneous access closure methods is the path forward.
Footnotes
Authors’ Note
Patient consent: The clinical data is collected prospectively and retrospectively in our AAA Quality Control Registry. The patients data was then de-identified and made anonymous. From this aggregated data file we organized the ProGlide results and wrote this article. Therefore according to The Norwegian Personal Data Law we may publish data in this form without the patients consent. The project ProGlide AAA EVAR was reviewed by the Data Protection Officer (DPO) Reference nr. 132655 on the 16 March 2020. In addition I have received approval from the Clinical Lawyer at The Oslo University Hospital, Ullevål. In addition I have applied to REC and they reviewed this study and concluded that we did not need a REC approval.
Prior presentation of the material: Some of the material in this study has been reported at the 2 following meetings. 1. 29-30 October 2018. Örebro, Sweden. A Endovascular Resuscitation and Trauma Management (EVTM) Workshop with emphasis on Resuscitative endovascular balloon occlusion of the aorta (REBOA). Title: Different ways to Close Large Bore Access Puncture Holes. 2. 15 March 2019. Geilo, Norway at the Winter meeting for the Norwegian Vascular Surgery Society. Title: Experience with the use of ProGlide SMCD in EVAR for AAA.
I presented both of these lectures.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Thomas Larzon is principle shareholder in Arterica Inc. (a company developing a vascular closure device).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.