
Abstract
Purpose:
The aim of the present study was to investigate a potential difference on the arterial stiffness among aneurysm patients and non-aneurysm controls, as well as to explore potential changes between patients treated either with endovascular or open repair.
Materials and Methods:
A 110 patients with an infrarenal AAA were prospectively enrolled in this study. Fifty-six patients received an EVAR, whereas 54 patients received an open surgical repair. Moreover, 103 gender and age-matched subjects without AAA served as controls. The cardio-ankle vascular index (CAVI) was applied for measurement of the arterial stiffness.
Results:
CAVI values were statistically higher in the AAA patients when compared with control subjects. Although at 48 hours postoperatively the CAVI values were increased in both groups when compared to baseline values, the difference in CAVI had a tendency to be higher in the open group compared to the endovascular group. At 6 months of follow up the CAVI values returned to the baseline for the patients of the open repair group. However, in the endovascular group CAVI values remained higher when compared with the baseline values.
Conclusion:
Patients with AAAs demonstrated a higher value of CAVI compared to healthy controls. A significant increase of arterial stiffness in both groups during the immediate postoperative period was documented. The increase in arterial stiffness remained significant at 6 months in EVAR patients. Further studies are needed to elucidate the impact of a decreased aortic compliance after stentgraft implantation on the cardiac function of patients with AAA.
Introduction
Despite the evolution of the treatment options and screening programs for abdominal aortic aneurysms (AAAs), the incidence, rupture risk and consequently the associated mortality rates remain considerable. 1 In the setting of an aneurysm, through complex pathways the normal vessel architecture is damaged, as the protease-antiprotease system of the arterial wall is unbalanced. The resultant elastin disturbances cause a stiffer, less compliant arterial wall. Enzymatic destruction of elastin is known to reduce elasticity, and in aneurysm formation. 2 The aneurysmal aorta is, therefore, significantly stiffer, than undilated age-matched aortas. 3
To date several methods have been suggested to assess arterial stiffness. Among them, pulse wave velocity (PWV),4-6 augmentation index,7,8 stiffness parameter β 9 and carotid-femoral pulse wave velocity (cfPWV) 10 have been used to quantitatively express arterial stiffness. During the last decade another parameter, the brachial-ankle pulse wave velocity (baPWV)11,12 has initiated as a further marker of cardiovascular disease. However, the blood pressure at the time of PWV measurement has considerable influence on final results and remains the main limitation of the aforementioned techniques of PWV assay.13,14 The cardio-ankle vascular index (CAVI) based on the theory of stiffness parameter β, was developed with the objective of obtaining an arterial stiffness index that is not affected by the blood pressure at the time of measurement.15,16 Moreover, several clinical studies have showed a great prognostic value of CAVI for cardiovascular events on patients with coronary artery disease, chronic renal insufficiency or diabetes mellitus.13,16-18 However limited data are up today available on the use of CAVI in patients with an AAA.
The aim of the present study was to investigate a potential difference on the CAVI values among aneurysm patients and non-aneurysm controls, as well as to explore potential changes of CAVI between patients treated either with endovascular or open repair.
Materials and Methods
Study Population
Between January 2014 and March 2015 110 consecutive patients with AAA were prospectively enrolled before undergoing elective endovascular or open surgical repair of their AAA (AAA group) at a tertiary institute. Fifty-six patients received an EVAR with a bifurcated stent-graft: Anaconda (Vascutek, a Terumo company, Inchinnan, Scotland); Endurant and Talent (Medtronic Vascular, Santa Rosa, CA, USA); Excluder (W.L. Gore & Associates, Flagstaff, AZ, USA); and Zenith FB (Cook Inc., Bloomington, IN, USA), whereas 54 patients received an open surgical repair with polyester graft (Gelsoft, Vascutek, a Terumo company, Inchinnan, Scotland).
Patients with thoraco-abdominal, thoracic or juxtarenal aortic aneurysms, aortic para-anastomotic pseudoaneurysms and ruptured aneurysms were excluded from our analysis. Also, patients with previous aortic surgery, aortic dissection, Marfan syndrome or other collagen-related disorders, advanced renal failure (GFR<30ml/min), or peripheral arterial occlusive disease (Ankle-brachial index ≤ 0.9 were excluded from the study.
Moreover, a total of 103 gender and age-matched subjects without AAA (91.3% males, mean age 71.1 ± 6.8 years), who were referred to our Institution for varicose or inguinal hernia repair, served as controls (CO group). The absence of AAA (infrarenal aortic diameter ≤ 3 cm) was documented by ultrasound or computed tomography examination within the last 2 years. They were considered eligible if they had negative functional testing for myocardial ischemia within the last 6 months.
Endpoints of the Study
The primary endpoints of the study were: to investigate a potential difference on the CAVI values among aneurysm patients and non-aneurysm controls and to explore potential changes of CAVI between patients treated either with endovascular or open repair. An ad hoc analysis was performed in an effort to correlate the changes in CAVI values with morphologic parameters of the aneurysm anatomy. This study was approved by the Committee on Research Ethics of our Institution (IRB Nr 806/23.09.2013) and informed consent was taken from all patients.
Patient’s Characteristics—Variables of Interest
Demographic data (gender, age) and co-morbidities (diabetes mellitus (DM); hypertension; coronary artery disease (CAD); nicotine consumption; chronic obstructive pulmonary disease (COPD); chronic renal insufficiency (CRI)) were obtained by a single researcher using explicit medical history. Systolic blood pressure (SBP), diastolic blood pressure (DBP) and heart rate (HR) as well as ankle-brachial index (ABI) were obtained at the time of CAVI measurement.
Moreover, morphologic parameters of the aneurysm (left iliac calcification, luminal volume (cm3), neck length (mm), left iliac diameter (mm), calcification >50% of the circumference, thrombus volume (cm3), neck diameter (mm), left iliac length (mm), neck angle > 45, thrombus > 50% of the circumference, right iliac diameter (mm), left iliac length (mm), right iliac calcification, AP diameter (mm), max length (cm), LL diameter (mm), MAX diameter (mm), sac volume (cm3)) were defined based on analysis of CT-angiography (CTA) with the Osirix MD software (Pixmeo SARL, Bernex, Switzerland).
Measurement of PWV With CAVI
The CAVI was measured 1-3 days before the procedure, within 48 h postoperatively and at 6-month follow-up visit using a VaseraVS-1000 vascular screening system (Fukuda Denshi, Tokyo, Japan). The participants rested in a supine position for 10 min, ECG electrodes were placed on both wrists, a phonograph for detecting heart sounds was placed on the sternum, and cuffs were wrapped around both the arms and ankles. CAVI can be calculated from PWV at the origin of the aorta to the distal segment of tibial artery (ankle), and the systolic and diastolic blood pressures can be measured at the brachial artery. After automatic measurements, obtained data were analyzed by software automatically and the CAVI was estimated.15,19 This index derives from the stiffness parameter β (β = In(Ps/Pd) x (2ρ/ΔP)xPWV 2 ), as suggested by Hayashi 9 by applying the Bramwell-Hill’s equation.15,16,18,20 In particular, CAVI is calculated by using the following equation: CAVI = aβ + b, where a and b are scale conversion constants, and β stiffness parameter. Hence, the equation for CAVI is: CAVI = a[(2ρ/ΔP × In (Ps/Pd) × PWV2] + b, where ρ: blood density; ΔP: blood pressure change; Ps: systolic BP in mm Hg; Pd: diastolic BP in mm Hg; PWV: pulse wave velocity from aortic valve to ankle.
Statistical Analysis
Continuous data were presented as the mean ± standard deviation or median (range), after Shapiro-Wilk test of normality of the distribution. Categorical data were given as the counts (percentages). Parametric variables were analyzed using Student t tests. A chi-square test was used for categorical data. A regression analysis was performed to explore the association between potential covariates related to arterial stiffness and the CAVI values. Furthermore, a multivariate analysis on AAA patients was conducted, in order to identify morphologic parameters that influence CAVI values. A p value < 0.05 was considered statistically significant for all measurements. All analyzes were performed using SPSS® Statistics Software Version 23 (IBM, Armonk, New York, USA).
Results
Comparison of PWV Between AAA and Control Patients
During the study, 1 patient succumbed due to respiratory failure, 4 patients dropped out due to personal reasons, and 2 patient experienced acute myocardial infarction 1 and 4 months after hospital discharge respectively. Thus, the final analysis included 103 patients (91.3% males, median age 71 years, range 62-84 years). Of these 53 underwent EVAR, whereas 50 underwent OSR.
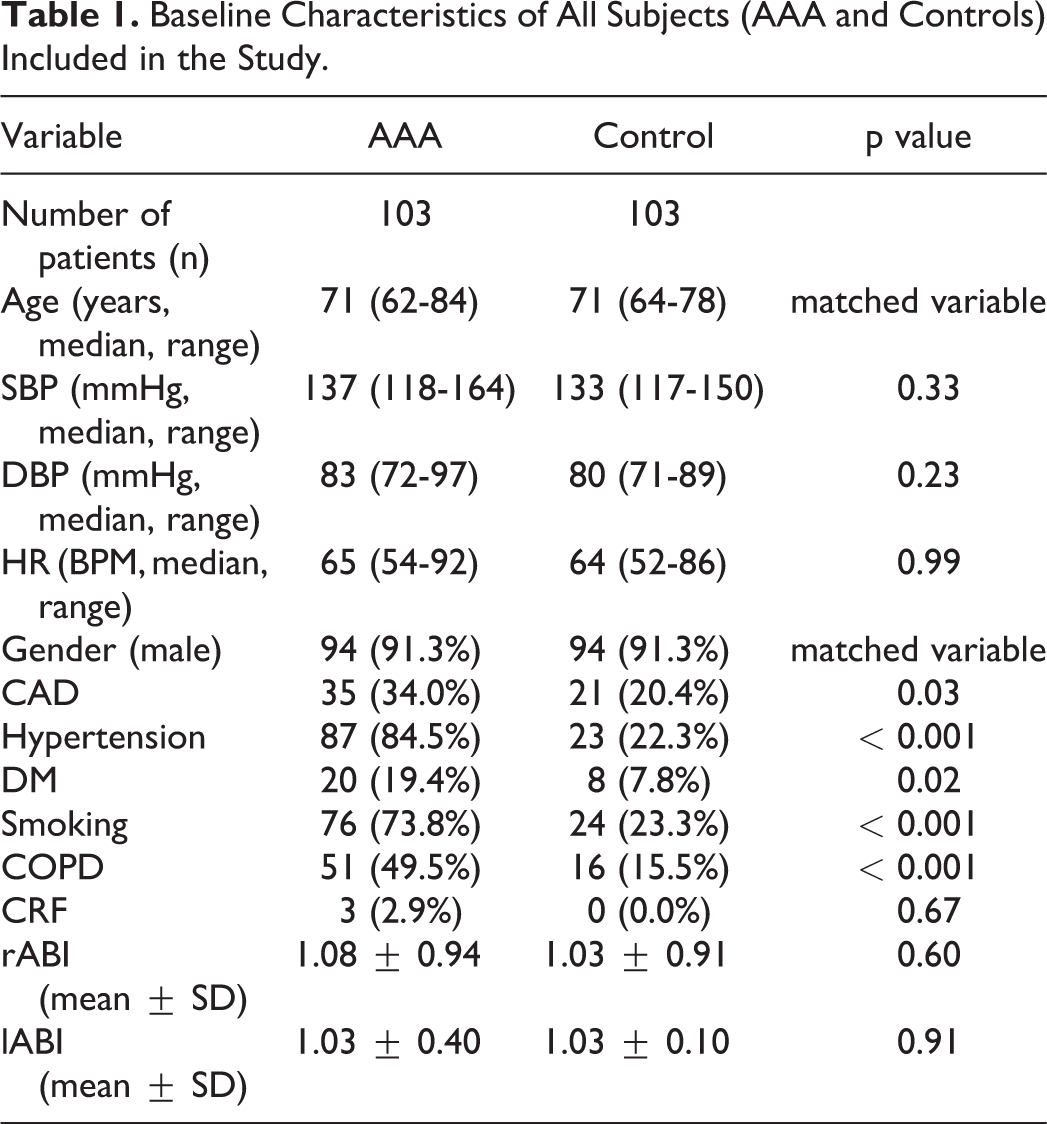
The Table 1 describes the baseline characteristics of all subjects. There was not a statistically significant difference in terms of gender (p = 0.99), median age (p = 0.94), SBP (p = 0.33), DBP (p = 0.23), HR (p = 0.99) between AAA patients and control subjects. However a statistically significant difference with regard to the frequency of history of CAD (P = 0.03), COPD, hypertension (p < 0.001), DM (p = 0.02), smoking (p < 0.001) and COPD (p < 0.001) was recorded.
Baseline Characteristics of All Subjects (AAA and Controls) Included in the Study.
The right CAVI (RCAVI) as well as left CAVI (LCAVI) were statistically higher in the AAA patients when compared with control subjects (9.86 ± 2.58 vs 8.80 ± 1.38, p < 0.001 and 9.54 ± 2.32 vs 8.79 ± 1.21, p = 0.003 respectively, Figure 1). The multivariate analysis revealed that only the presence of an AAA was a statistical significant confounder of the CAVI values (Table 2).
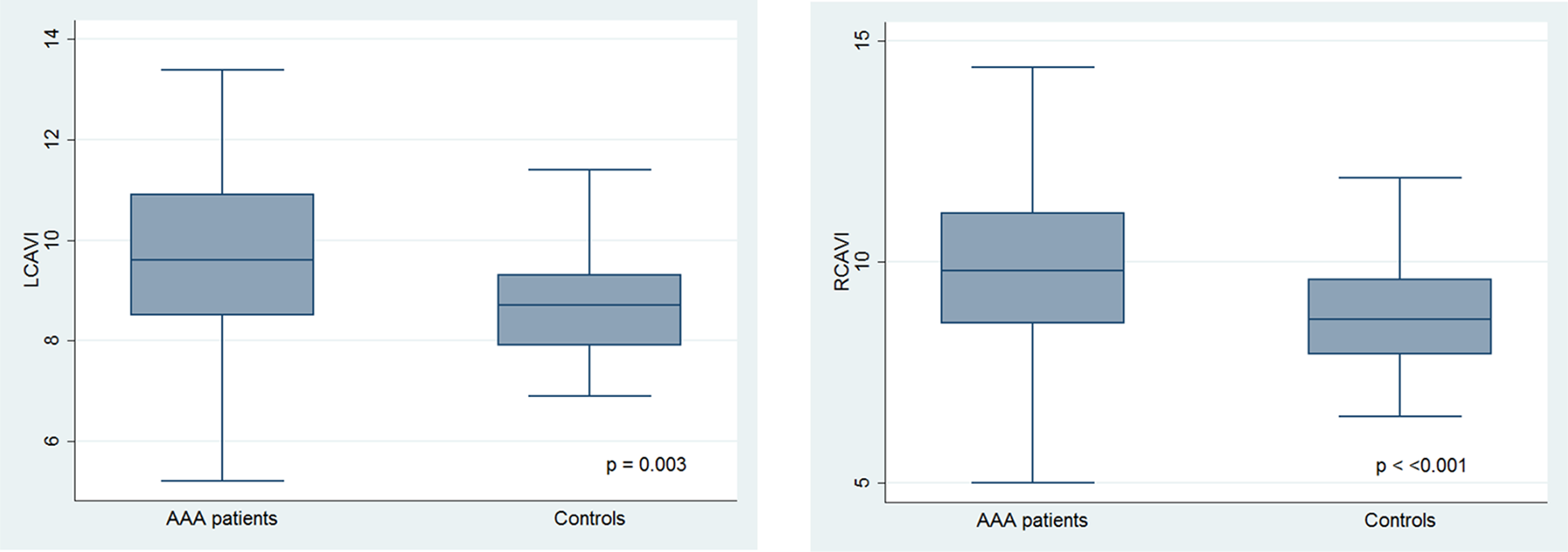
Comparison of CAVI values between AAA and control patients.
Multivariate Analysis for Confounders of the CAVI.
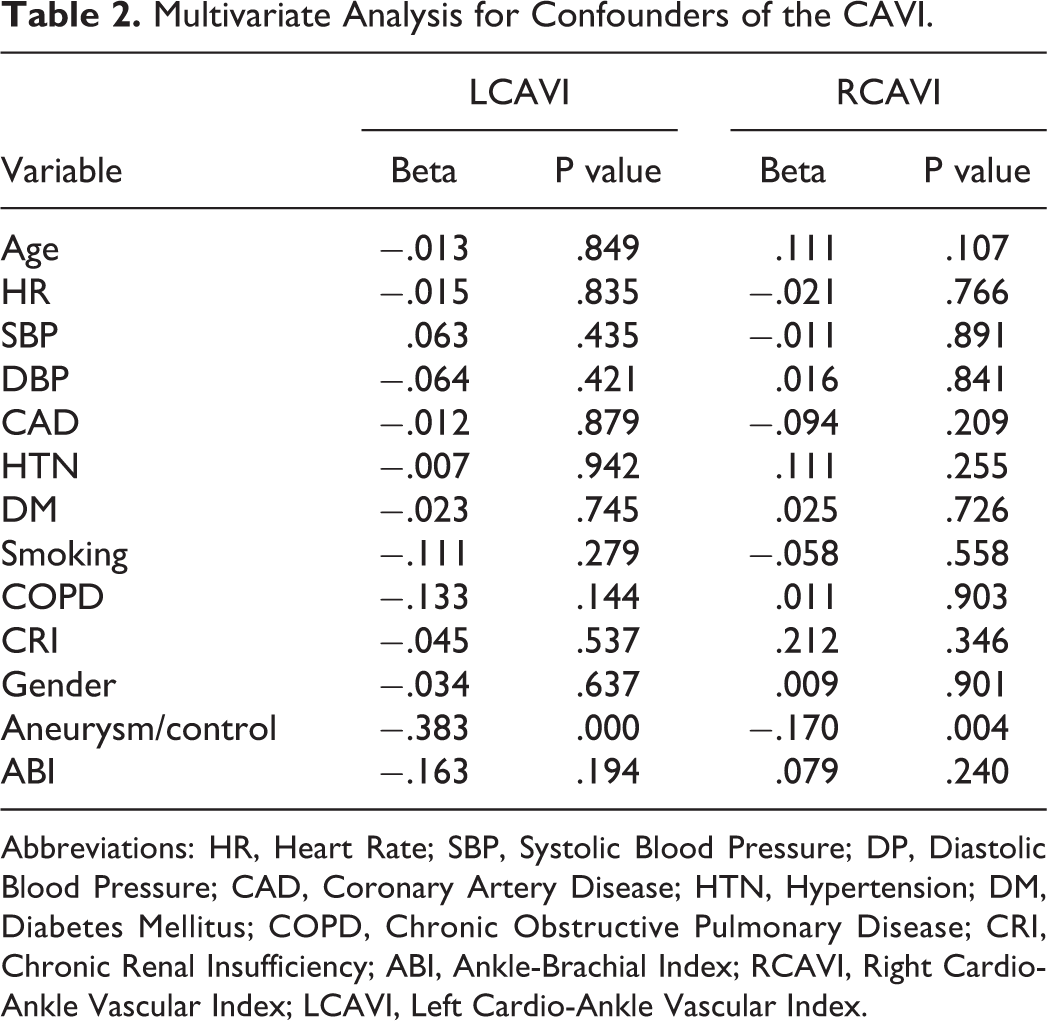
Abbreviations: HR, Heart Rate; SBP, Systolic Blood Pressure; DP, Diastolic Blood Pressure; CAD, Coronary Artery Disease; HTN, Hypertension; DM, Diabetes Mellitus; COPD, Chronic Obstructive Pulmonary Disease; CRI, Chronic Renal Insufficiency; ABI, Ankle-Brachial Index; RCAVI, Right Cardio-Ankle Vascular Index; LCAVI, Left Cardio-Ankle Vascular Index.
In an effort to identify potential morphological parameters, which could have an impact on the CAVI value, we conducted a regression analysis. None of the investigated variables was found to significant influence the CAVI values (Table 3).
Regression Analysis Correlating Changes in PWV With Morphologic Parameters of the Aneurysm Anatomy.
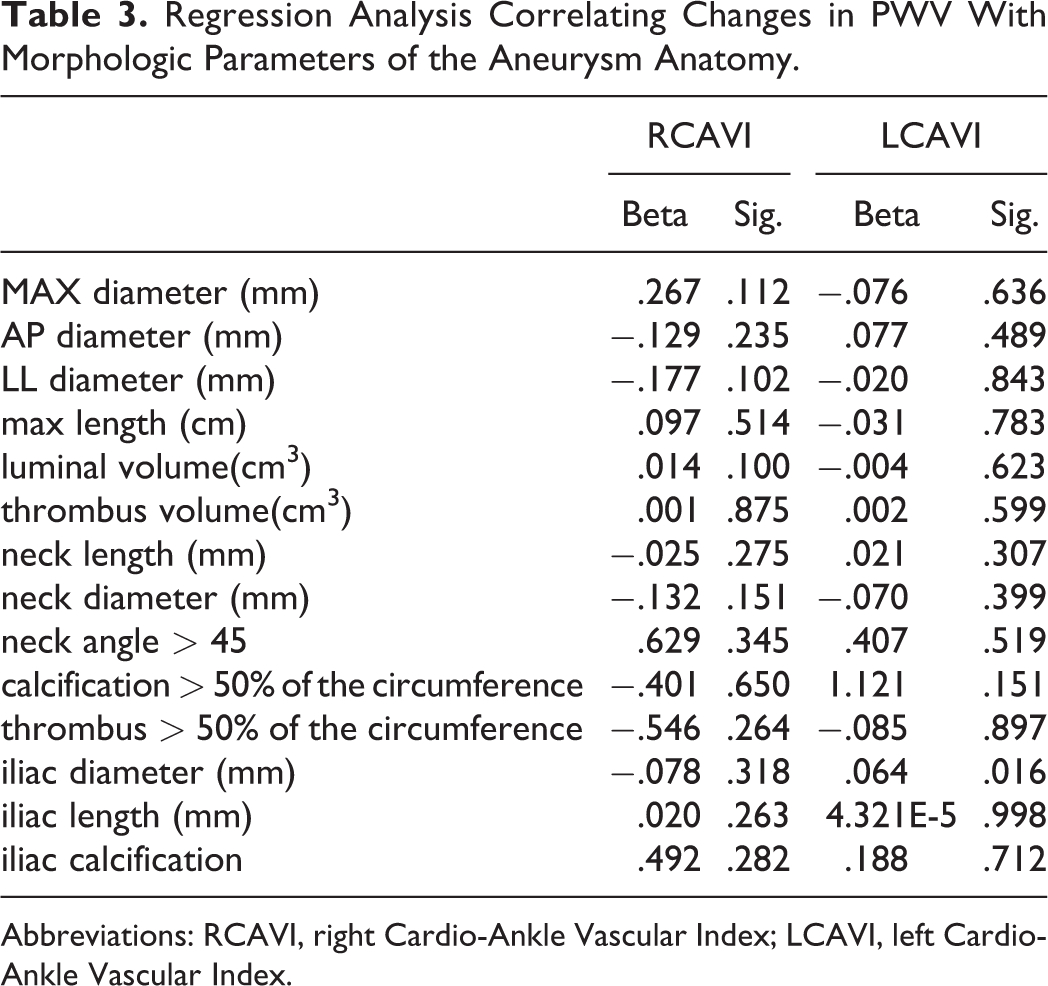
Abbreviations: RCAVI, right Cardio-Ankle Vascular Index; LCAVI, left Cardio-Ankle Vascular Index.
Comparison of PWV in Patients Undergoing Endovascular and Open Repair
In Table 4 are listed the baseline characteristics of the AAA patients undergoing endovascular or open repair. The CAVI was found significantly higher 48 hours postoperatively in the open repair group compared to the preoperative values (1.16 mean difference for LCAVI, p = 0.04, and 1.57 mean difference for RCAVI p = 0.024,) (Table 5). The CAVI was found significantly higher also in the endovascular group 48 hours postoperatively compared to the baseline values (mean difference 0.8 for LCAVI p = 0.04 and 0.8 for RCAVI p = 0.04) (Table 5)
Baseline Characteristics of the AAA Patients Undergoing Endovascular or Open Repair.
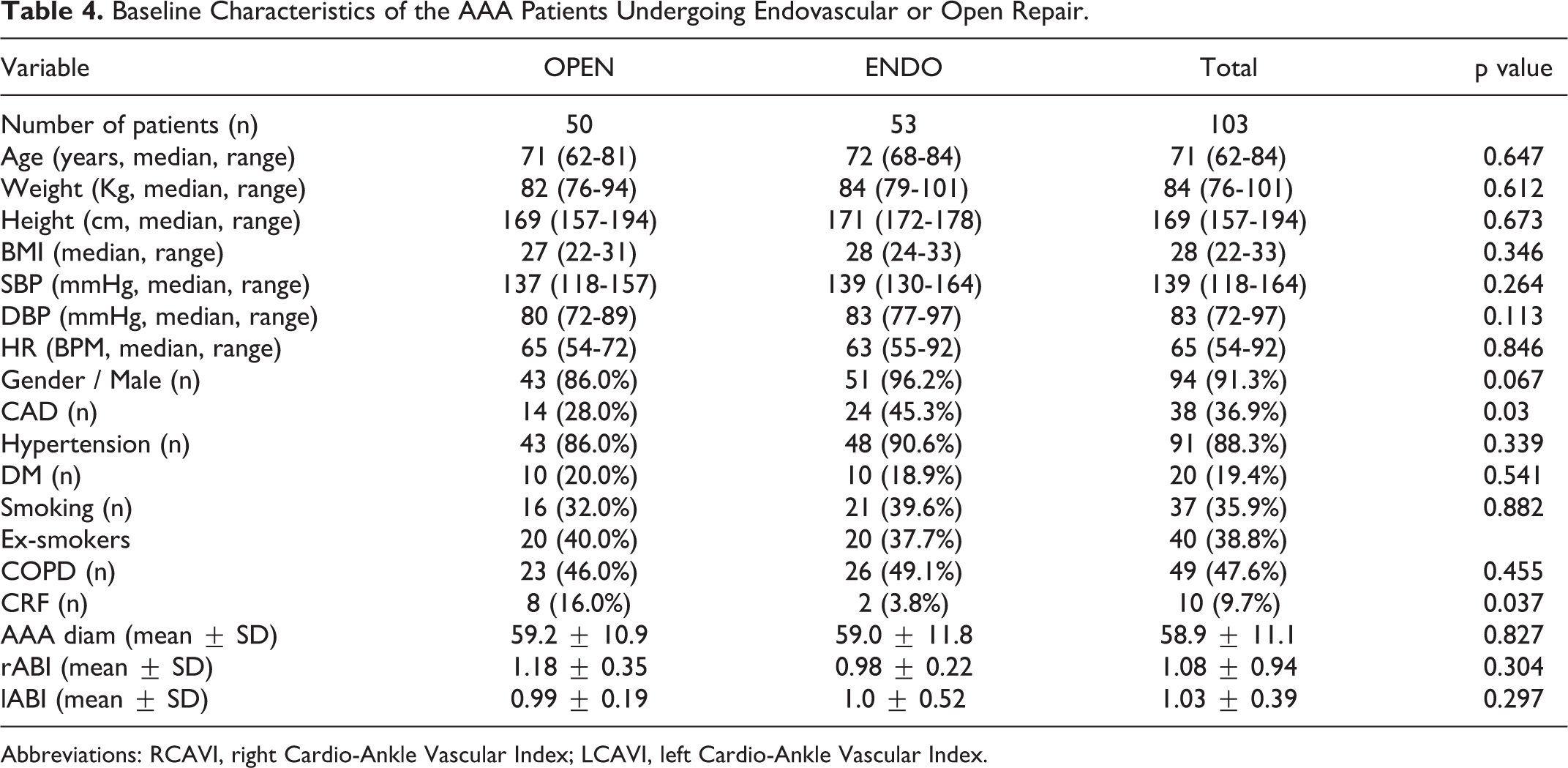
Abbreviations: RCAVI, right Cardio-Ankle Vascular Index; LCAVI, left Cardio-Ankle Vascular Index.
CAVI Values in the Endovascular and Open Repair Group Preoperatively, at 48 Hours Postoperatively and at FU. Dif.1: Difference Between Preoperative Values and Values 48h Postoperatively (Mean ± SD); Dif.2: Difference Between Preoperative Values and Values at Follow up Visit (Mean ± SD).
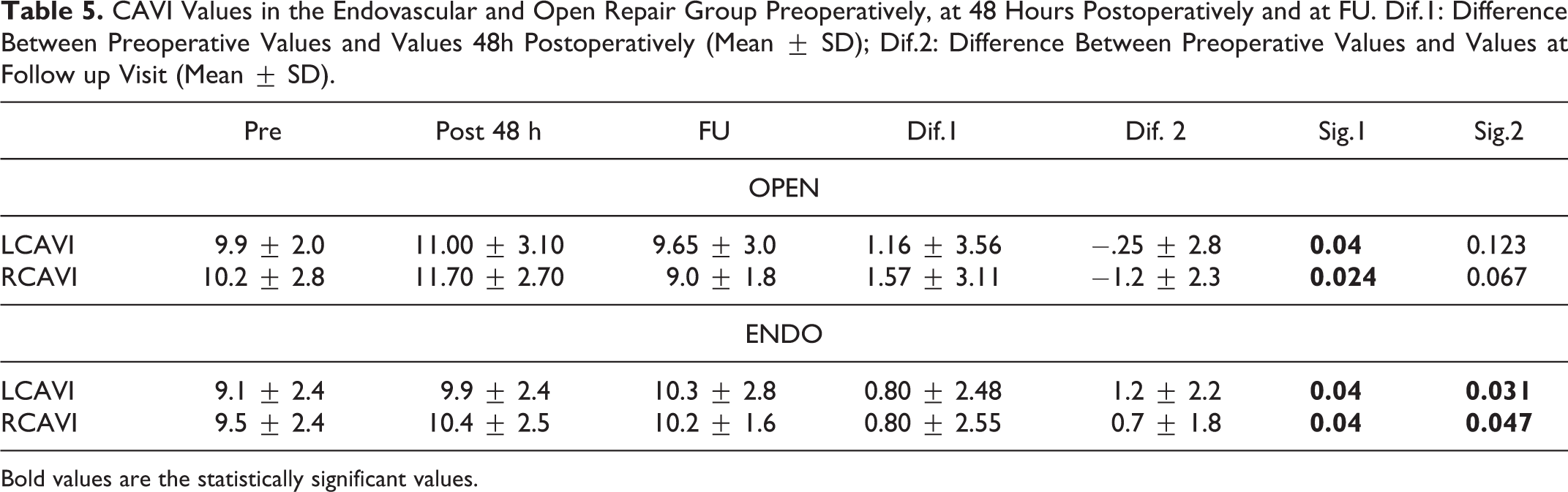
Bold values are the statistically significant values.
Although at 48 hours postoperatively, the difference in CAVI had a tendency to be higher in the open group (Open: 1.16 for LCAVI and 1.57 for RCAVI vs Endo: 0.8 for LCAVI and 0.8 for RCAVI) compared to the endovascular, the difference between the 2 groups, did not reach a statistical significance (p = 0.59).
At 6 months of follow up the CAVI values returned to the baseline for the patients of the open repair group (9.65 ± 3.0 for LCAVI and 9.0 ± 1.8 for RCAVI). However, in the endovascular group CAVI values remained higher (10.3 ± 2.8 for LCAVI, p = 0.031 and 10.2 ± 1.6 for RCAVI, p = 0.047) when compared with the baseline values. (Table 5)
Discussion
It has been well documented from the literature that arterial stiffness is an independent predictor of increased cardiovascular morbidity and mortality as an indicator of extension of atherosclerosis through the arterial tree.13,16-18,20 This could be attributed in several risk factors such as advanced age, smoking history hypercholesterolemia, hypertension, ect. Moreover, previous studies have shown that arterial stiffness appears to be significantly increased in patients with AAA.5,21 This is due to the reasonable hypothesis that on molecular basis infrarenal abdominal aortic aneurysms are associated with elastin degradation on the aortic wall, overproduction of abnormal collagen and calcium deposition leading to a stiffer, less compliant aneurysmal aorta.2,3 It is well known that these changes in aortic wall in case of aneurysm degeneration could have common risk factors with atherosclerosis.
We conducted this study applying a relatively novel marker of measuring the PWV, the cardio-ankle vascular index (CAVI), which has the considerable advantage of not being affected by the blood pressure at the time of measurement.15,16 It can, also, predict the cardiovascular events on patients with coronary artery disease, chronic renal insufficiency or diabetes mellitus.16,18 Although widely adopted, the reference values of CAVI are not worldwide standardized and several cut-off values have been proposed along age for PWV. In a large-scale study, which was conducted in Japan in healthy individuals free of cardiovascular disease, CAVI linearly increased with age, from 20 to 70 years. CAVI in men was higher than that in women for almost all age groups, but men and women showed a similar rate of increase in CAVI of approximately 0.5 per year. The clinical threshold appied was set at a value of 9.0. 20 The mean CAVI value in our control group of healthy patients was 8.80 ± 1.38. The multivariate analysis revealed that only the presence of an AAA was the statistical significant parameter that can influence the PWV, as expressed with CAVI values, in the study population (AAA patients and control subjects). This finding can highlight the prognostic significance of increased arterial stiffness and justify why the life expectancy of patients who undergo successful AAA repair is not as good as that of the age and sex-matched general population. 22
Aiming to further investigate the increased CAVI values of aneurysm patients compared to control subjects, we attempted to correlate the CAVI with morphologic parameters of the aneurysm. Several studies have suggested that the presence of intraluminal thrombus or the large diameter of the aorta can affect the haemodynamic properties of the aorta. 23 Thus, our initial hypothesis was that the quantity of wall thrombus, the maximum diameter of the aneurysm and parameters of the proximal and distal landing zone might affect arterial stiffness. However, none of the investigated variables was found to significant influence the CAVI values.
Another endpoint of our study was to explore comparatively changes of CAVI in patients treated either with endovascular or open repair. On this point it should be noticed that, on the contrary to aneurysmatectomy in open repair, the aneurysm sac in EVAR remains intact after aortic endovascular repair, and an intrasac pressure may often persist, due to endoleaks. 24 In EVAR patients a remodeling of the sac, which evolves over time, reflects the complex interactions between the intra-aneurysm sac pressure, the thrombus and the mechanical characteristics of the endograft. 25 We documented an increase of arterial stiffness in the early postoperative period with both techniques. There is an adaptation period for arterial elasticity after any arterial intervention, which might explain the temporal elevation of the CAVI values.
Although at 48 hours postoperatively, the difference in CAVI had a tendency to be higher in the open group compared to the endovascular, the difference between the 2 groups, did not reach the threshold of statistical significance. Our results are consistent with a study on 50 patients (39 with a graft-prosthesis and 11 with a stentgraft) by Lantelme et al, who suggested that stentgraft increases reflected waves, as recorded with carotid-femoral PWV, more than graft-prostheses. 26 Moreover, another study by Gray et al 27 reported a significantly higher postoperative PWV measurement than those undergoing open abdominal aortic aneurysm repair.
Six months after the procedure the CAVI values returned to the baseline levels for the patients of the open repair group, while in the endovascular group the CAVI values remained significantly higher when compared with the baseline levels. The hemodynamic impact and the clinical implication of altered arterial stiffness after EVAR remains obscure. A study by Takeda et al 25 investigating the echocardiographic changes of patients undergoing EVAR found that endografting leads to left ventricular (LV) hypertrophy and impaired LV diastolic function in the acute and chronic phase, which can severely affect cardiovascular reserve function. Increased arterial stiffness augments myocardial work and oxygen demands in systole and reduces myocardial oxygen supply in diastole, leading to subendocardial ischemia. 25 As a result, especially in high risk patients with preexisted cardiac disease who have LV diastolic dysfunction, EVAR may aggravate or even cause the clinical syndrome of heart failure in the mid or long term.28,29 A meta-analysis of individual-patient data from the 4 multicentre randomized trials of EVAR versus open repair, showed a lower risk of perioperative mortality with EVAR compared with open repair. 30 However after 3 years the aneurysm-related mortality was significantly higher in the EVAR group. Moreover, the authors reported no early survival advantage under EVAR in patients with previous coronary artery. 30
Our study has several limitations, which should be taken into consideration when interpreting the results. Although we included more than 100 patients, the inability to achieve a longer follow up, due to patients incompliance, led to a lack on the mid- to long-term results regarding mortality and cardiac morbidity. Moreover, our results could have further been supported with echocardiographic findings, which would have confirmed an alteration of the cardiac function after the aneurysm treatment. Another parameter, which could have an impact on the arterial stiffness and not further analyzed is the perioperative medication of the recruited patients. However, the application of the CAVI technique on estimating the PWV of the aorta, which overcomes the impact of the blood pressure on the measurements, as well as the presence of a control group improve the robustsness of our findings.
In conclusion, our study documented an increased PWV, as expressed with CAVI values, for patients with an AAA. Moreover, a significant increase of arterial stiffness in both groups—EVAR and open repair—48 hours postoperatively and a significant increase of arterial stiffness at 6 months in EVAR patients compared to the baseline values were found. Further studies are needed to elucidate the impact of a decreased aortic compliance after stentgraft implantation on the cardiac function of patients with AAA.
Footnotes
Authors’ Note
EBD 806 /23.09.2013 Review Board “Attikon” University Hospital Athens, Greece. Concept and design: SNM, KGM, NK. Analysis and interpretation: SNM. Data collection: SNM. Writing the article: SNM, KGM, NK. Critical revision of the article: TEK, JK, KK, CL. Final approval of the article: all authors. Statistical analysis: SNM, CA. Overall responsibility: SNM.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.