
Abstract
Introduction:
Intraluminal thrombolytic therapy is the first step treatment of thrombotic malfunction of tunneled hemodialysis catheters (THC). The factors that affect catheter restoration and also catheter survival following thrombolytic therapy are not well described. In this study, we aimed to reveal the predictors that affect the success of the procedure and also present post-restoration catheter patency after intraluminal thrombolytic administration.
Method:
This retrospective study included 62 patients with tunneled THC thrombosis treated with alteplase between 2017 and2020 in the study center. Age, comorbidities, the use of antiplatelet and anticoagulants, a history of catheter thrombosis, time on dialysis, the duration of the catheter were investigated as possible predictors of procedural success. The independent predictive factors for procedural success were evaluated by using backward stepwise likelihood ratio logistic regression analysis. Primaryand assisted patencieswere presented with Kaplan-Meier graphs.
Results:
Thrombolityc was administered to 62 patients 102 times. The median primary patency from the first thrombolytic administration to a second catheter thrombosis was 9 months (range 1-20 months). The overall median patency was 12 months (range 2-23 months). The overall procedural success rate was 79.4% (81/102).Multivariate analyses revealed that a history of prior catheter thrombosis was the only risk factor for procedural success (OR: 0.49; 95% CI: 0.26-0.91; p = 0.004). The need for a second dwell time among patients with prior history of thrombolysis was significantly higher compared to patients without a history of catheter thrombosis (12/26 patients, 46.2% and 6/55 patients, 10.9%; respectively; p = 0.001).
Conclusion:
The success of thrombolysis in subsequent de novo THC thrombosis decreases in patients who previously required intraluminal thrombolytic administration. Identifying patient subgroups with a high risk for THC thrombosis may be useful to investigate effective secondary prevention strategies.
Introduction
Hemodialysis is the most common method of renal replacement therapy. 1 Adequate vascular access is critical for these patients to maintain their hemodialysis sessions. Despite the advantages of arterio venous fistulas and grafts (AVF and AVG), a significant portion of patients rely on tunneled hemodialysis catheters (THC) at a certain period in their lives.2-4 More than half of the patients start their dialysis program with a permanent dialysis catheter 5 Delayed nephrology referral, ineligibility for AVF creation, limitation of access to surgical facilities, as well as dysfunction in the fistula all can result in a need for THC. One-year catheter durability rate has been reported to be less than 50%. 4 The most important reason limiting the durability THCs is catheter malfunction. The reasons for catheter malfunction are catheter malposition - usually early period (kinking or incorrect position), infection, catheter thrombosis, and fibrin sheath formation. Failure of the permanent dialysis catheter can cause delays in hemodialysis and a need for catheter interventions and their related complications.
Catheter thrombosis is responsible for approximately one-third of patients with catheter malfunction. 6 Thrombolytic therapy is a proven effective treatment method in catheter thrombosis. However, there is no robust consensus yet in terms of agent selection, dosage, and method of administration. 7 Favorable outcomes of systemic anticoagulation are reported for maintaining THC patency in some studies. 8 However, a meta-analysis found no clear benefit on catheter durability of systemic agents over conventional care with heparin based locking solutions 9 The 2019 KDIGO guidelines do not recommend routine use of warfarin however, low dose acetyl salicylic acid may be used in patients with low bleeding risk to maintain THC patency. 1 The same guidelines highlight the need for studies investigating thrombolytic techniques and their impact on THC patency outcomes and complications.
The aim of this study was to examine the catheter restoration rates and catheter patency in patients who underwent thrombolytic therapy with alteplase to treat tunelled CVC thrombosis. In addition, we aimed to determine the factors affecting the success of thrombolytic therapy. These factors may help to select patients in whom measures should be taken to prevent THC dysfunction.
Methods
Study Design
An observational, nonrandomized study was conducted in patients with tunneled THC thrombosis between January 2017 and January 2020. The population consisted of patients who were continuing the dialysis program with a permanent dialysis catheter in 4 hospital-based dialysis centers (a total of 55 hemodialysis devices). The study hospital was the only vascular access center in the city (estimated population 400,000). The treatment of all patients with dialysis catheter dysfunction was managed by the dedicated vascular access team. Written informed consent was obtained from all patients who were thought to be suitable for thrombolytic therapy. The study protocol was approved by the Ethics Committee of Bezmialem Vakıf University Faculty of Medicine (Certificate of Approval number:54022451-050.05.04/2020) after obtaining local hospital permission. The study was conducted in accordance with the Helsinki Declaration.
Patients with tunneled CVC thrombosis who were administered thrombolytic therapy were included in the study. The exclusion criteria were as follows: Patients who were administered any thrombolysis protocol in external centers before or during the study, except for the management vascular access team of the reference hospital Patients under the age of 18 or pregnant Patients who have previously reported a reaction to alteplase Patients with catheter malposition Patients who do not accept thrombolytic therapy Patients who need urgent hemodialysis for any indication
Intervention Protocol
Information about renal replacement therapy-based history, current medications, duration of catheter usage, previous catheterization, and catheter salvage therapies were recorded from all patients who presented with catheter malfunction.
Catheter dysfunction was defined as an inadequate blood flow to initiate or resume dialysis (peak flow <200ml/min or <250 ml/min during 2 consecutive dialyzes). Catheter thrombosis was confirmed by the push-pull technique. If catheter restoration could not be achieved with serial irrigation and forceful flush, a thrombolytic agent was administrated. Alteplase was used as a thrombolytic agent. One mg of alteplase (2 mg total) was instilled in both lumens. Aspiration was performed after 45 minutes. If there was no resistance in blood aspiration, the procedure was accepted as successful. If occlusion continues or the volume in aspiration is insufficient, the procedure was repeated with the same dwell time. Once patency was restored, 5 mL of blood was aspirated to ensure the removal of the thrombolytic agent and the residual clot. If patency was not achieved despite 2 thrombolysis attempts, catheter removal or exchange was performed. Following successful restoration of THC, patients immediately were referred to HD to confirm flow rates of 300 ml/min. Following successful restoration of the catheter, patients with a recurrent malfunction due to thrombosis at any time were treated with the same protocol. No additional systemic medication was used to prevent THC dysfunction
Analysis of Outcomes
Primary patency reflects thrombosis free survival after first successful thrombolysis. De novo catheter malfunction due to thrombosis is the endpoint of the primary patency. Assisted patency is defined as the overall time after the first successful thrombolytic therapy until the removal or exchange of the catheter due to thrombosis. Data on the removal of the catheter include only patients whose thrombosed catheter cannot be restored by thrombolysis. Catheter removal data do not include infection, changes to renal replacement therapy, or termination of dialysis. Safety outcomes include major bleeding, embolic events, and allergic reactions. A previous catheter malfunction due to thrombotic occlusion treated successfully by thrombolytic administration was defined as a history of catheter thrombosis.
Statistics
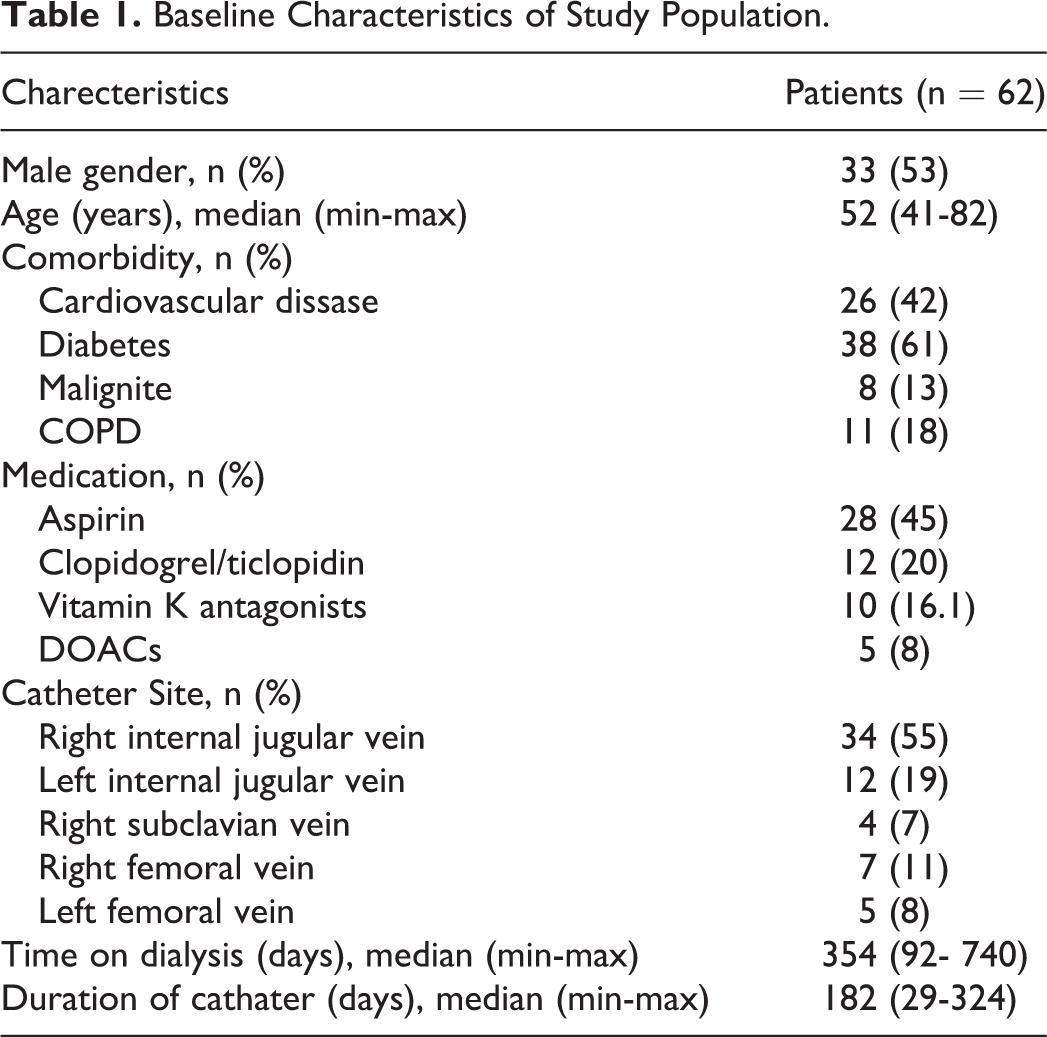
Gender, age, comorbidity (Cardiovascular disease, diabetes, malignancy, chronic obstructive pulmonary disease), current medications (Aspirin, Clopidogrel/ticlopidine, Vitamin K antagonists, DOACs), catheter site, time on dialysis, duration of catheters were analyzed for the multivariable logistic regression model (Nagelkerke R2 = 0.545). The final model was constructed by independent predictive factors for procedural success by using backward stepwise likelihood ratio logistic regression analysis. The most significant variables that predicted procedural fail were determined at the last step. Odds ratio (OR) and 95% confidence interval (Confidence Interval, CI) reported for all variables. A discriminative multivariate Cox proportional-hazards model could not be generated for predictive factors for catheter survival. Primary patency and assisted patency survival curves were shown with Kaplan-Meier graphs.
Categorical variables were presented as counts and frequencies; continuous variables as mean (Standard deviation, SD) or median (Interquartile range, IQR) as appropriate. Chi-square test or Fisher’s exact test was used for comparison between categorical variables. Student t-test or Mann Whitney U test was used to compare continuous variables. A 2-tailed p-value of 0.05 was considered statistically significant. SPSS version 23.0 (SPSS, Chicago, IL) was used for all statistical analyses.
Results
During the study period, the data of 62 patients meeting the study criteria were investigated. The study flow diagram was demonstrated in Figure 1. The main vascular access of the patients was the internal jugular vein. The detailed characteristics of the study patients are shown in Table 1.
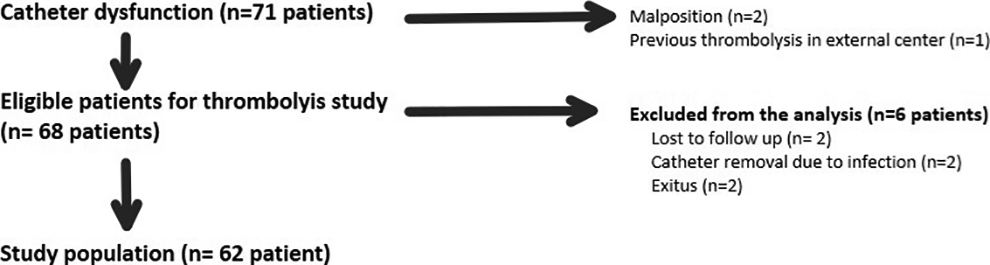
Study flow diagram.
Baseline Characteristics of Study Population.
Thrombolityc was administered to 62 patients 102 times (once for 36 patients, twice for 8 patients, 3 times for 16 patients). The overall procedural success rate was 79.4% (81/102). The restoration (i.e. patency) was achieved at the first dwell time in 63 of 81 (77.8%) successful attempts, while recanalization at the second dwell time was achieved in 18 (22.2%) attempts
The success rate was 88.7% (55 of 62 patients) in patients without a history of catheter thrombosis. In patients with a history of catheter thrombosis, the success rate was 75% (18 of 24) for patients receiving thrombolytics for the second time and 50% (8 of 16) for patients receiving thrombolytics for the third time. The multivariate analyses revealed that a previous history of catheter thrombosis was the only risk factor for procedural success (OR: 0.49; 95% CI: 0.26-0.91; p = 0.004). In patients with a history of catheter thrombosis, the requirement of a second dwell time of alteplase was much more pronounced than patients without thrombolytic history for successful restoration. The need for a second dwell time of alteplase among patients without a history of catheter thrombosis (6 of 55 patients, 10.9%), was significantly lower by comparing to the patients with a history of catheter thrombosis (12 of 26 patients, 46.2%),(p = 0.001).
The mean follow-up period of 55 patients after the first successful thrombolysis was 11.5 ± 4.6 months (range 1-23 months) (. The median catheter survival time for these patients was 442 days (range 32-816 days). The median primary catheter patency after the first thrombolytic administration was 9 months (range 1-20 months) (Figure 2). Following thrombolysis, 46 patients were thrombus-free at 6 months, and 21 patients at 12 months remained thrombosis-free. The median assisted catheter patency time was 12 months (range 2-23 months) (Figure 3). Considering catheter removal-free survival; 50 patients in the sixth month and 32 patients in the 12th month continued to use the original THC
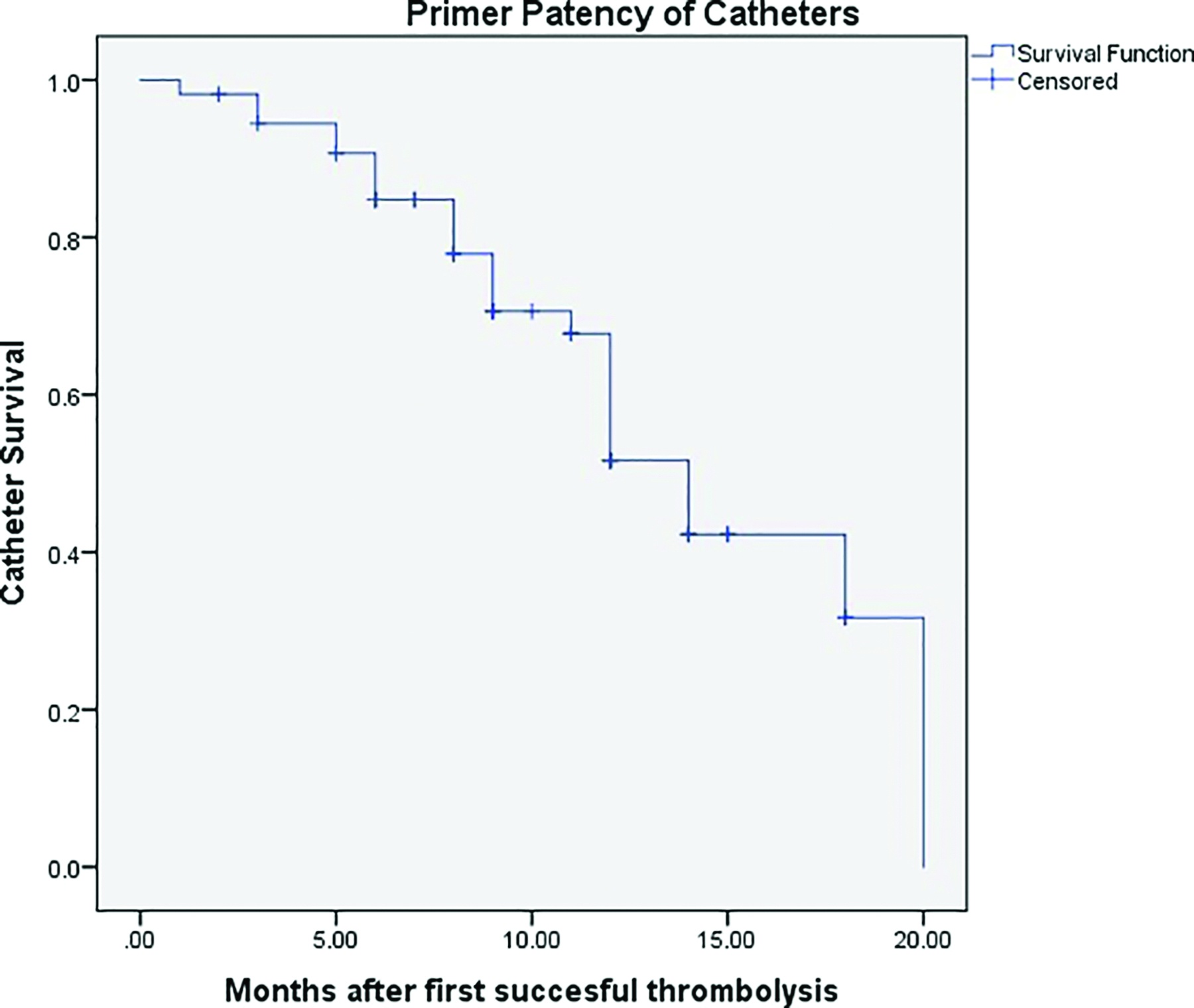
Thrombosis-free survival curves of the patients after first successful thrombolysis.
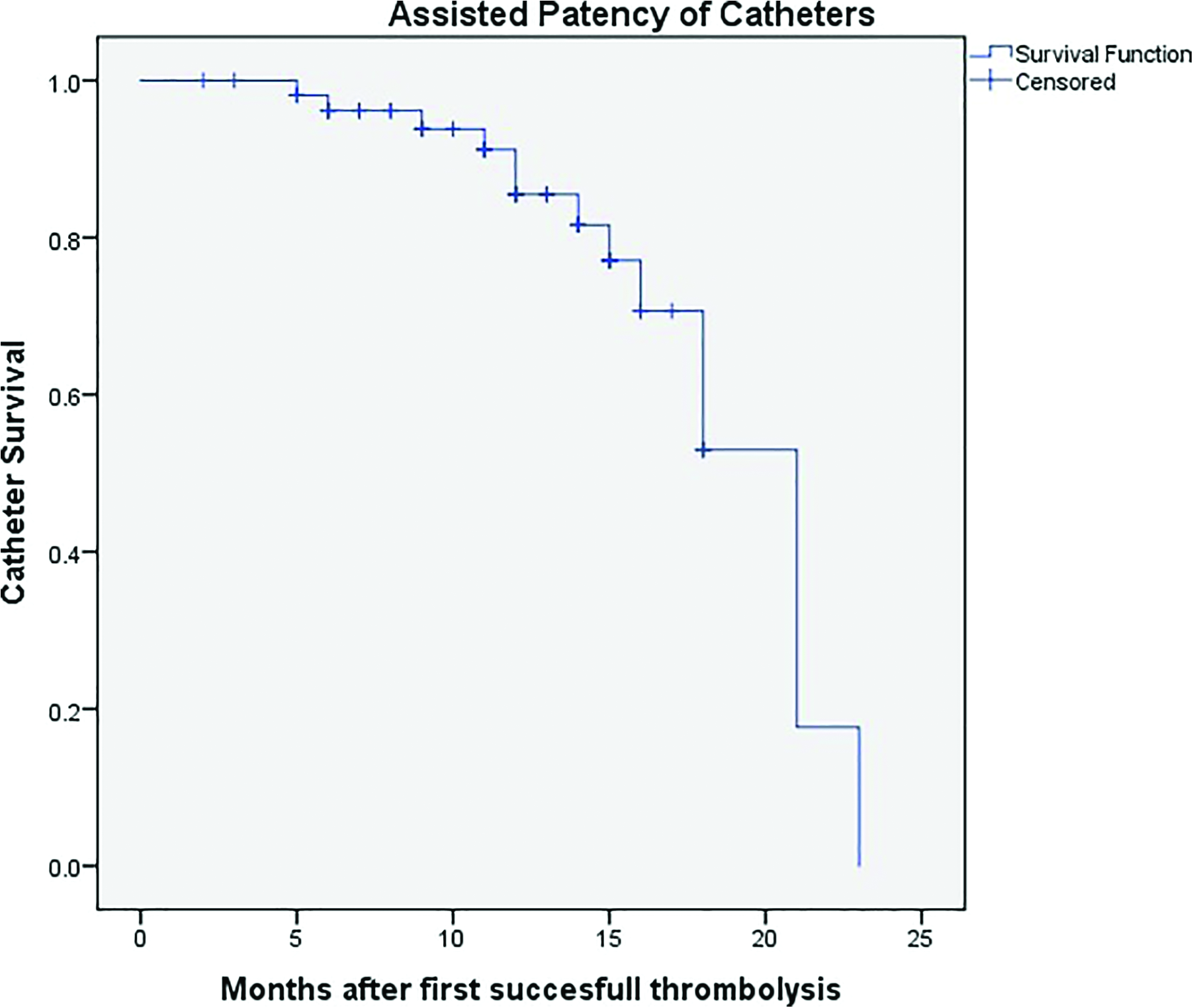
Assisted catheter patency survival curves of the patients after first successful thrombolysis.
Discussion
In this observational study, we have analyzed the efficacy of alteplase in catheter-related thrombosis. Additionally, we evaluated the long-term patency of tunneled HC following successful thrombolysis. In more than half of patients, catheter patency can be extended by up to 1 year with one or more treatments. Procedural success decreases with repeated thrombolytic attempts and requires a higher dose of alteplase for adequate restoration.
Thrombolysis interventions reduce the need for frequent catheter replacement and can avoid delays in dialysis due to catheter dysfunction. We submit that this approach is safer, more convenient for the patient, and more cost-effective than catheter replacement. The main pharmacological mechanism of thrombolytic agents is accelerating plasmin activation. Reteplase, urokinase, and alteplase are recommended products for catheter restoration in current guidelines.1,10 Alteplase is a commonly used fibrin-specific thrombolytic agent resulting in high restoration rates and low incidence of allergic reaction. 11 Alteplase has a cumulative success rate of 86,5% for catheter clearance with a maximum dwell time of 120 min and a maximum of 2 doses. 10 Different procedural results have been reported depending on the thrombolytic agent, administration method, patient population. Due to the heterogeneity of the studies, there is still no consensus on the optimal dose and method of administration. In accordance with the literature, this study also demonstrated that thrombolytic therapy is an effective (88.7% for the first administration, 79.4% for all administration) and safe method for restoring catheter patency in thrombosed THC.
Maintaining catheter patency remains an important challenge in the daily care of the HD patient. . Standard care in preventing catheter failure is the use of heparin solutions locked in catheter ports following dialysis. There is insufficient evidence for the effectiveness of alternative catheter locking solutions in catheter thrombosis prophylaxis. 12 Recent studies have speculated that the periodic use of thrombolytic agents as a catheter lock solution can prolong catheter survival compared to citrate or heparin based solutions.13-15 However, prophylactic use of recombinant tissue plasminogen activator has been found to be associated with high costs. 15 Systemic low dose anticoagulation was found to be ineffective for prophylaxis. 16 The routine use of systemic anticoagulation or antiplatelet drugs for secondary prevention of catheter thrombosis is not recommended due to potential bleeding risks. 12 However, a potential benefit exists for their use in secondary prevention of catheter thrombosis in patients with a high risk of catheter thrombosis, or for patients with limited vascular access. Intraluminal thrombolytic therapy remains the only proven effective catheter salvage modality that prolongs patency. Wojtowıcz et al. found that the occurrence of diabetes mellitus significantly decreases catheter maintenance after the first successful thrombolysis. 17 Another recent study revealed that the time since catheterization, diabetes, and exit site infection is associated with thrombotic obstruction after thrombolytic therapy. 18
The major limitation of our study is the lack of a meaningful multivariate model regarding the factors affecting catheter life after successful thrombolysis. This was a result of our low sample size and, short follow-up with missing data
After successful thrombolysis, a significant number of patients develop recurrent catheter thrombosis. Catheter life is the main focus of all dialysis access studies. However, factors affecting thrombolysis success remain poorly understood. Our study revealed that a prior hisoty of catheter thrombosis is a risk factor for future thrombolytic therapy failure. These findings indicate that this patient group is at risk for catheter thrombosis-related catheter loss. In this study no additional prophylactic measures were applied after successful thrombolysis. However, the majority of our cases were on antiplatelet or anticoagulant therapy for other causes; which may explain the relatively high CVC patency rates in our study group. Coli et al. found a benefit in warfarin administration, after CVC placement, in comparison to its administration after the first malfunction event. 8 Current guidelines recommend against the use of warfarin because of the potential harm of increased bleeding risk . Our study revealed that once CVC thrombosis occurs the success of its treatment with endoluminal thrombolytic therapy diminishes even if the first attempt is successful. To protect the patient from invasive procedures and to preserve vascular access sides, we believe that systemic agents to prevent catheter dysfunction such as warfarin can be administered to patients with previous thrombotic catheter malfunction who have acceptable bleeding risk.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.