
Abstract
Background:
Chronic limb-threatening ischemia is a severe form of peripheral artery disease that leads to high rates of amputation and mortality if left untreated. Bypass surgery and antegrade endovascular revascularization through femoral artery access from either side are accepted as conventional treatment modalities for critical limb ischemia. The retrograde pedal access revascularization is an alternative treatment modality useful in specific clinical scenarios; however, these indications have not been well described in literature. This case report highlights the use of retrograde pedal access approach as primary treatment modality in a patient with an extensive comorbidities precluding general anesthesia nor supine positioning.
Case Presentation:
The patient is a 60-year-old female with multiple severe cardiopulmonary comorbidities presenting with dry gangrene of the right great toe. Her comorbidities and inability to tolerate supine positioning precluded her from receiving open surgery, general anesthesia or monitored sedation, or percutaneous femoral access. Rather, the patient underwent ankle block and retrograde endovascular revascularization via dorsalis pedis artery access without post-operative complications.
Discussion:
The prevalence of comorbidities related to peripheral artery disease is increasing and with it the number of patients who are not optimal candidates for conventional treatment methods for critical limb ischemia. The retrograde pedal access revascularization as initial treatment modality offers these patients an alternative limb salvaging treatment option.
Introduction
Peripheral artery disease (PAD) is a highly prevalent disease that affects the lives of over 200 million people worldwide. PAD is associated with comorbidities such as diabetes mellitus, coronary artery disease, cerebrovascular disease, and obesity. 1 Chronic limb-threatening ischemia (CLTI) is a severe manifestation of PAD whose presentation includes rest pain, tissue loss, and gangrene. Without intervention, patients with CLTI have a 75% 1-year overall survival and 45% 1-year survival without major limb amputation. 2 Thus, it is imperative that every patient with CLTI is considered for intervention to revascularize the limb, both for limb salvage and overall survival. Given the significant comorbidities that are often present in the CLTI patient population, endovascular intervention has often become the first-line treatment for many patients.3-5 Endovascular revascularization is conventionally performed via femoral artery access, either through contralateral retrograde access or ipsilateral antegrade access.3,4,6 Retrograde tibiopedal access for endovascular revascularization is an alternative for patients who have failed or have absolute contraindications to the antegrade approach. 6 However, the use of retrograde pedal access as primary intervention is nascent in the literature. In this case report, we discuss the utilization of retrograde pedal access limb revascularization as the primary intervention in a patient who could not lie supine or tolerate anesthesia due to her extensive medical comorbidities.
Case Description
The patient is a 60-year-old female who presented to the vascular clinic with dry gangrene of the right great toe for several months (Figure 1). Her past medical history was significant for severe pulmonary hypertension (pHTN) on 4 L home oxygen and intermittent noninvasive average volume-assured pressure support, congestive heart failure (CHF), end-stage renal disease (ESRD) on hemodialysis, coronary artery disease (CAD), obstructive sleep apnea (OSA), and obesity with BMI of 45 kg/m2. At the time of initial presentation to the clinic, the patient denied lower extremity pain or systemic signs of infection. Additionally, the review of systems was positive for shortness of breath and general weakness. On physical exam, Doppler signals for dorsalis pedis arteries were appreciated bilaterally, both feet were warm to touch, right leg swelling was noted, and the right great toe was gangrenous. The ankle-brachial index (ABI) study done a month prior to the clinic visit showed a non-diagnostic right ABI due to non-compressible vessels and severe perfusion deficit to the right great toe with toe pressure of 0 mmHg. The left side showed partially non-compressible vessels with toe-brachial index of 0.27. From history and exam, the urgent need for a diagnostic angiogram with intervention to minimize the propagation of tissue loss was conveyed to the patient, to which the patient agreed.

Dry right great toe gangrene on initial evaluation in clinic.
The patient subsequently underwent a pre-operation evaluation; due to dyspnea on minimal exertion, CHF, OSA (Mallampati Class 3), pHTN, and obesity, the patient was classified in the ASA IV category. Thus, only minimal sedation was recommended, precluding general anesthesia and open surgical intervention. The patient’s cardiopulmonary comorbidities presented a significant risk to the patient undergoing a procedure that may require her to lie supine on the operating table for a prolonged amount of time. Thus, the decision was made to perform an angiogram with possible intervention via retrograde pedal access while having the patient sitting up, with regional anesthesia for the toe amputation.
In the operating room, the patient was prepped with her upper body propped up to a near 90° by adjusting the operating table angle and utilizing multiple pillows for support. The patient did not undergo any sedation. After a popliteal nerve block was performed by the regional anesthesia team, the right dorsalis pedis artery was accessed under ultrasound guidance using a 5-French micropuncture slender sheath set. Back bleeding was noted, and fluoroscopic imaging confirmed the intraluminal position of the access wire. Diagnostic angiogram was notable for moderately diseased superficial femoral artery (SFA), moderate-to-severely diseased but patent popliteal artery with multiple areas of high grade stenoses, and severely diseased but also patent right anterior tibial artery with stenoses down to the ankle (Figure 2A). The peroneal artery was notable for moderate disease but demonstrated flow to the ankle (Figure 2B), while the posterior tibial artery occluded prior to the medial malleolus. In addition, we performed intravascular ultrasound (IVUS; Visions PV.014, Philips) examination of the iliac arterial system, common femoral artery, superficial femoral artery, popliteal artery and anterior tibial artery via the 5Fr sheath after exchanging for an .014” wire. Given the described findings, the decision was made to intervene, and balloon angioplasty was performed to the SFA and popliteal artery using 6 mm and 7 mm balloons over the .014” wire; the anterior tibial artery was balloon angioplastied with a 3 mm balloon. Maintaining retrograde dorsalis pedis access, the peroneal artery was selected via an “up-and-over” approach from the anterior tibial artery. This was performed by using a Glidewire GT (Terumo) with a double-curved tip and an .018” Quick Cross catheter (Philips) to carefully select the tibioperoneal trunk and subsequently the peroneal artery down to the ankle. (Figure 2C) The .014” wire was again placed and the tibioperoneal trunk and entire peroneal artery was angioplastied with a 3 mm balloon. Repeat angiogram demonstrated significant improvement of the SFA, popliteal, anterior tibial, and peroneal arteries with flow down to the ankle. (Figure 3). Hemostasis was achieved by manual compression for 5 minutes, and strong biphasic Doppler signals were appreciated for both the anterior tibial artery and the dorsalis pedis artery. After hemostasis was achieved, the right great toe was amputated at the metatarsophalangeal (MTP) joint, and gross purulence was noted upon incision. The wound edges were pulled together with Nylon suture with the MTP joint left open, which was then packed with betadine-soaked gauze. The patient was tolerated the procedure without difficulty and did not require additional sedation.
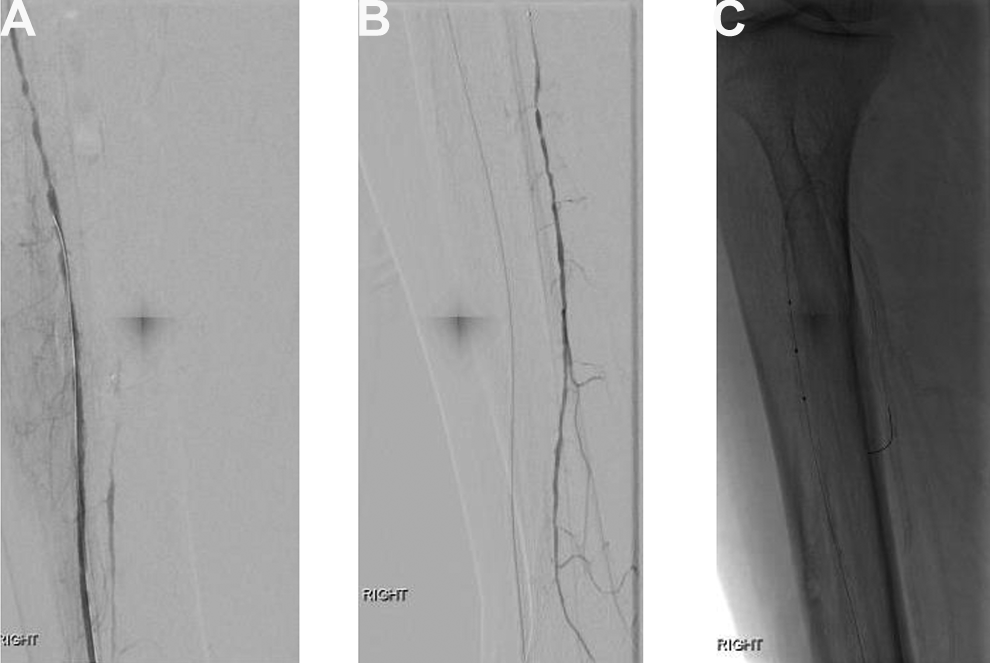
Pre-intervention angiography findings. A, Diffuse anterior tibial artery disease. B, Diffuse peroneal artery disease. C, Wire access to peroneal artery via anterior tibial artery.
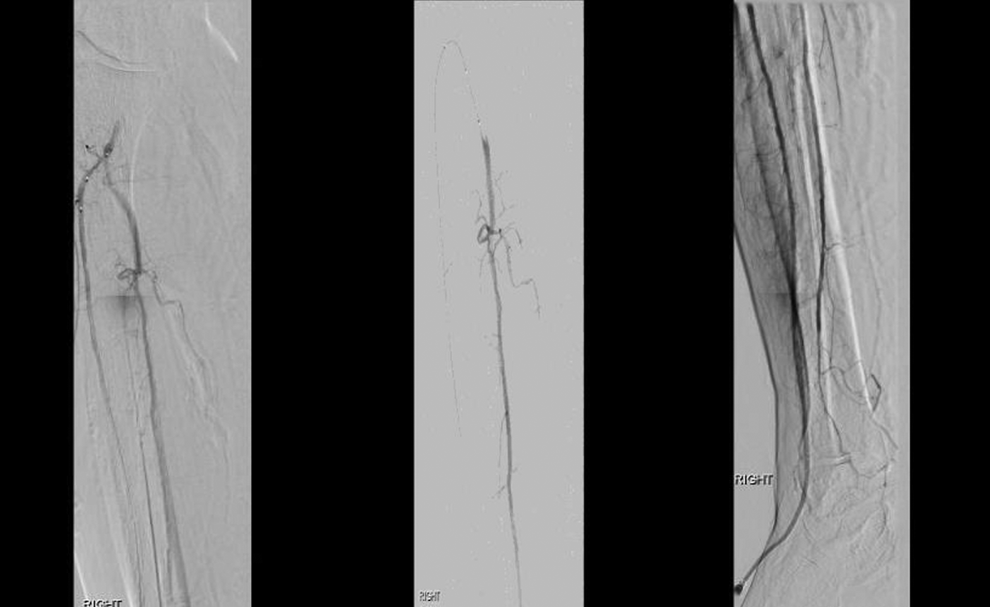
Post-intervention angiography findings with improved anterior tibial and peroneal artery flow.
Post-operatively, the patient was without any complications relating to the procedure including but not limited to hematoma, bleeding, or acute occlusion of the right dorsalis pedis access site. At the time of this writing the surgical site was nearly healed and she was more ambulatory, aiding in her pulmonary rehabilitation.
Discussion/Conclusion
Advantages of the retrograde pedal approach over the antegrade approach are as follows: 1) the proximal portion of atherosclerotic plaque is more calcified; thus, the softer distal portion may be easier to traverse retrograde and cross the lesion; 2) often yields shorter distance from the target lesion, implying stronger wire “pushability;” 3) less chance of entering branch vessels via retrograde access due to branching angles; and 4) minimizes access complications seen with femoral access.3-5 Complications of the retrograde pedal access may include pain, compartment syndrome, pedal access site acute thrombosis, dissection, bleeding, vasospasm, hematoma, access artery perforation and pseudoaneurysm.3,4,7 Disadvantages of retrograde pedal access compared to antegrade approach are: 1) higher theoretical risk of thrombosis at the access site due to smaller vessel diameter; 2) higher risk of complication from vasospasm due to smaller vessel lumen; and 3) more difficult access due to smaller vessel diameter.3-5 Utilizing sheaths designed for smaller vessels such as transradial sheaths (e.g. Glidesheath Slender sheaths, Terumo) and treating the access vessel with an intra-arterial solution of anticoagulation and vasodilators (e.g. heparin and nitroglycerin) intermittently or as a slow continuous infusion supports this access for longer revascularization procedures. We tend to use 5Fr slender sheaths but 7Fr is possible depending on the diameter and quality of the pedal vessel. This allows for use of many endovascular devices, including balloon angioplasty and IVUS as demonstrated here, but also atherectomy devices and some stents to treat the femoro-popliteal system in addition to the infra-popliteal system.
There is no randomized clinical trial to date comparing the antegrade and the retrograde approach. The retrograde pedal access approach is reported to have a technical success rate of 69 to 100%, though a review paper by Kang et al reported a technical success rate of 84.9% with pooled data from other studies. 4 This is comparable to the technical success rate of 89.0% published in a meta-analysis study by Romiti et al, pooling data from 30 articles on infra-popliteal percutaneous transluminal angioplasty. 8 Unfortunately, the long-term clinical outcomes such as the limb salvage rates for retrograde technique are not well-understood. 4
Even with its shortcomings, retrograde pedal access is treated as a suitable alternative after a failed antegrade revascularization.4-7,9 Indeed, this is the most common indication for the retrograde pedal access revascularization4,7; however, there are limited studies demonstrating the use of retrograde access as primary intervention. Awasthi et al published a case report describing 2 cases; the indications for primary retrograde pedal access revascularization were bilateral iliac artery aneurysms precluding contralateral femoral artery access and SFA occlusion at the ostium precluding ipsilateral femoral artery access. 10 Another case series published by Mustapha et al described the use of retrograde pedal access through the posterior tibial artery for a patient with an extensive list of comorbidities. The patient experienced circulatory and respiratory distress during a diagnostic angiogram done via the conventional femoral artery access. The diagnostic angiogram also resulted in a groin hematoma. During the retrograde revascularization, the patient’s upper body was elevated at 45° to encounter for the risk of supine positioning. Indications for the retrograde pedal access listed by Mustapha et al includes unsuitable vascular anatomy for antegrade approach, morbid obesity, and conditions preventing patients from lying flat. 9 There is limited data to support multiple tibial revascularization over single vessel revascularization in CLTI, in general, if the single vessel is in-line to the foot.11,12 The impetus in this case was to maximize the angiosome perfusion to this region of the foot to offer the best chance of healing the site of great toe amputation. This is of particular importance when considering a patient with limited or nonexistent options for further revascularization.
In this case report, we describe a patient whose comorbidities—pHTN, OSA, CHF, ESRD, CAD, and morbid obesity—precluded anesthesia or lying flat. The retrograde pedal access served many purposes in our patient: 1) bypass the need for difficult groin access; 2) prevent groin complications such as groin hematoma and infection; 3) use a peripheral nerve block alone as adequate anesthesia; and, importantly, 4) allow the patient to remain in a sitting position throughout the procedure. The local anesthesia and the sitting position, similar to the cases reported by Mustapha et al, prevented cardiopulmonary complications from occurring in the operating room while still allowing the patient to receive an endovascular intervention to improve perfusion to her foot. Our patient underwent both the diagnostic angiogram and the angioplasty of diseased vessels in 1 procedural setting. Thus, this case report demonstrates an example of the retrograde pedal access approach without previous antegrade approach attempt and failure in a patient whose medical conditions were contraindications for the antegrade revascularization. The retrograde approach has become more practical and usable over the years with advances in technology, e.g. retrograde pedal access kits by different companies and the shared experiences by experts in the field.6,7,9 With the comorbidities in CLTI patients becoming increasingly more prevalent, it is important to recognize the patient population who would benefit from the retrograde pedal access revascularization approach as the initial treatment modality. Long-term outcomes in this patient population need to be studied for future direction.
Footnotes
Authors’ Note
Informed consent has been obtained from the patient for publication of the case report and accompanying images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.