
Abstract
Objectives:
Patients often require multiple access re-interventions to improve fistula patency and the overall usable lifespan of autogenous arteriovenous fistula (aAVF). There is no consensus on the appropriate number of re-interventions after which an access should be abandoned and new access placed. We evaluated whether repeated endovascular interventions for failing/failed aAVF are worthwhile or futile.
Methods:
A retrospective review was performed on aAVFs created between 2009-2014. Fistula function was evaluated until January 2017. Functional fistula patency (FFP) was defined as the total time of functional fistula use for hemodialysis, from time of cannulation to time of measurement or fistula abandonment, including all interventions performed to maintain/reestablish patency. Primary outcomes were FFP duration and number of post-dialysis interventions.
Results:
The study included 163 patients. Mean age was 67 (SD = 15.03). The only variable statistically different between functional fistulas and abandoned fistulas was obesity (p = 0.03). At the end of the study period, 145 (89.0%) patients continued to have functional fistulas, and 73 (44.8%) patients died, but had functional fistulas at time of death. Median FFP for the functional group was 3.18 years (range 0.01-7.01 years) and median number of interventions was 1 (range 0-13). In 18 patients (11%), the fistula was abandoned, most commonly due to thrombosis (47.1%), followed by infection (23.5%). No fistula was abandoned because of an unacceptable rate of reintervention. Median FFP in the abandoned group was 0.91 years (range 0.03-5.30 years), and median number of interventions was 0 (range of 0-5).
Conclusions:
Through repeated interventions on aAVFs, none of the patients in our study exhausted all hemodialysis access options prior to transplantation, death or loss to follow-up. These results may indicate repeated and/or more frequent revisions do not negatively affect the FFP nor do they increase the overall risk for abandonment of aAVFs.
Introduction
Chronic kidney disease is a steadily increasing problem in today’s aging population estimated to affect nearly 650,000 patients in the United States with an incident growth rate of more than 1% per year.1,2 In 2010, the overall incidence of end-stage renal disease (ESRD) was 348 per million population, or 105,923 dialysis patients. 3 Although the annual incidence has remained relatively stable, the prevalence in 2010 increased by 49% since 2000. 3 KDOQI guidelines have emphasized the importance of increasing the prevalence of autogenous access compared to grafts and catheters. Autogenous fistulas have been shown to have greater patency rates, lower associated morbidity and mortality, and decreased overall cost.4-6 Thus, the Fistula First initiative recommended institutions should aim for >65% of patients to have functional autogenous fistulas, and <10% should have catheters.4-6 Following the publication of these guidelines, the prevalence of autogenous access doubled, while grafts and catheters decreased. Almasri et al showed an increase in autogenous arteriovenous fistula (aAVF) prevalence from 24% to 68% between the years 1997 to 2013, whereas graft and catheter prevalence decreased by half from 49 & 27% to 18 & 15%, respectively. 7
The growing population of dialysis patients has presented challenges, such as the means and methods for improving and maintaining access patency. Indeed, the primary assisted and secondary patency of aAVF has improved markedly with the advent of endovascular interventions, with secondary patency rates being upward of 70% after intervention. 8 In order to achieve improved fistula patency and the overall usable lifespan of aAVFs, patients are often required to undergo multiple access interventions. KDOQI previously suggested surgical revision should a fistula or graft require angioplasty more than 2 times within 3 months; however, this is not Grade 1 evidence and is primarily based on opinion in the field.4-6 However, these have since been modified in the 2019 revision of KDOQI to recommend surgical revision after endovascular failure, lesions not amenable to endovascular treatment, and situations where surgical outcomes are markedly better. 9 There is, unfortunately, still no evidence-based consensus on the appropriate number of aAVF re-interventions after which an access should be abandoned and a new access placed.
In our vascular surgery practice, we perform repeated endovascular revisions of malfunctioning aAVF in our efforts to delay or avoid the need to place reduced patency, more complication prone, nonautogenous grafts. Therefore, we wanted to evaluate if our practice of repeated endovascular interventions for failing or failed aAVF are worthwhile or futile and perhaps lend suggestions on the long-term management of malfunctioning AVFs.
Methods
A retrospective chart review was performed on all aAVFs created between the years 2009 and 2014 at a single center. AVFs created included radiocephalic, brachiocephalic, and basilic vein transpositions. Patient characteristics were evaluated for age, gender, comorbidities, smoking status, and use of anticoagulation. Data on each aAVF was further extracted from the electronic health records (EHR), including date of creation, type of fistula, date of first intervention, number and types of interventions, as well as date and causes for abandonment. Any surgical procedure, ligation or revision, was considered abandonment of the fistula and therefore not included in analysis, other than outcome of fistula function. Fistula function was evaluated in the charts up until January 2017. In our vascular practice, we evaluated our aAVFs with a duplex ultrasound performed within 4-6 weeks after creation, where fistula size and presence of stenotic lesions are assessed, and readiness for use is determined. Should the fistula be deemed inadequate due to small size, large tributaries, or areas of stenosis, an intervention was then performed in the form of balloon maturation or ligation vs embolization of collaterals. Fistula function was determined by successful hemodialysis sessions, as defined by dialysis nursing and nephrology staff. However, we now use flow volume measurements to evaluate our fistulas in our current practice, as well as near the end of the study period.
Functional fistula patency (FFP) was defined as the total time of functional fistula use for HD, including all interventions performed to maintain or reestablish patency, from the time of cannulation to the time of fistula abandonment, the end of the measurement period (January 1, 2017), or censorship (i.e. loss to follow up, death, kidney transplant) . The date recorded for loss to follow-up was the last office visit with the patient, while the date for kidney transplant was recorded as the date of surgery, and the date of death according to documentation of expiration in the patient’s medical chart.
The primary outcome measures of this study were defined as the duration of functional fistula use and the number of interventions after establishment of successful dialysis. We evaluated fistulas requiring interventions to aid in maturation as well as those not requiring assistance in maturation. However, interventions performed for the purpose of aiding in fistula maturation, prior to starting dialysis, were not included in the calculation of total number of interventions. In this way, we were able to analyze outcomes related to the implementation of multiple interventions in prolonging the functional lifespan of aAVFs. Furthermore, in order to evaluate the effect of more numerous interventions, we further subdivided the groups based on number of interventions: 2 or less and 3 or more. We chose 3 interventions as the cutoff for the group of more numerous interventions based on the KDOQI suggestion that having 2 angioplasty interventions within 3 months should prompt surgical revision and/or abandonment.
StataSE version 16 (StataCorp LLC, College Station, TX) was used for all analyzes. We calculated descriptive statistics for all variables, and computed p-values using the Student’s t-test and Chi-square test for differences between participants that had functional fistulas and those with abandoned fistulas. We ran similar analyzes to assess differences in patient characteristics and co-morbidities among patients with less than or equal to 2 re-interventions and patients with greater than or equal to 3 re-interventions. Various tests were also used to verify assumptions for our regression analyzes. We used the Kaplan-Meier survival analysis, with person-years as our measure of survival time, to determine the cumulative risk of aAVF abandonment over time. We performed these analyzes with both the full dataset, grouped by obesity status, and grouped by number of re-interventions (≤ 2 and ≥ 3). The log-rank test was used to assess the differences between the survival curves of these groups with a null hypothesis that there was no difference between the functions.
We performed univariate logistic regression with aAVF abandonment as the outcome variable to identify statistically significant covariates and/or confounders. We then used multivariable logistic regression to determine the odds of aAVF abandonment among relevant predictors identified in the prior step. We also performed negative binomial regression to determine relevant covariates and/or confounders for the total number of aAVF re-interventions. We chose this analysis because the outcome variable was a count variable, was over-dispersed, and had a large proportion of zeroes. After univariate analyzes, we ran multivariable negative binomial regression with zero inflation to determine the incidence rate ratio of the total number of re-interventions for specific predictors. We set our level of statistical significance a priori at α = 0.05 for all statistical significance testing.
This study was approved by the Biomedical Research Alliance of New York Institutional Review Board, protocol number 17-08-12-337. The requirement to obtain informed consent was waived.
Results
Between January 1, 2009 and December 31, 2014, 163 patients met criteria and underwent the creation of aAVFs. The average age of patients was 67 years old (SD = 15.03), and the majority were Caucasian (70.5%), male (N = 105, 64.4%), and with a history of hypertension (93.2%). Only 18 of 163 resulted in aAVF abandonment during their time in the study. However, of the 145 that had functional fistulas, 7 were lost to follow-up, 14 had kidney transplants, and 73 died prior to the end of the study period, January 1 2017, but all had functional fistulas up until these end points.
Median number of interventions was 1 with a range of 0-13 (or mean 1.53, SD = 2.11). The only variable that showed a statistically significant difference between functional fistulas and abandoned fistulas was obesity (p = 0.03). The type of fistula was of no impact (p = 0.77). Additional descriptive statistics of this sample are detailed in Table 1.
Descriptive Statistics for Patients That Had Autogenous Arteriovenous Fistulas (aAVF) Placed Between January 1, 2009 and December 31, 2014 at a Community Hospital in Northeastern United States.
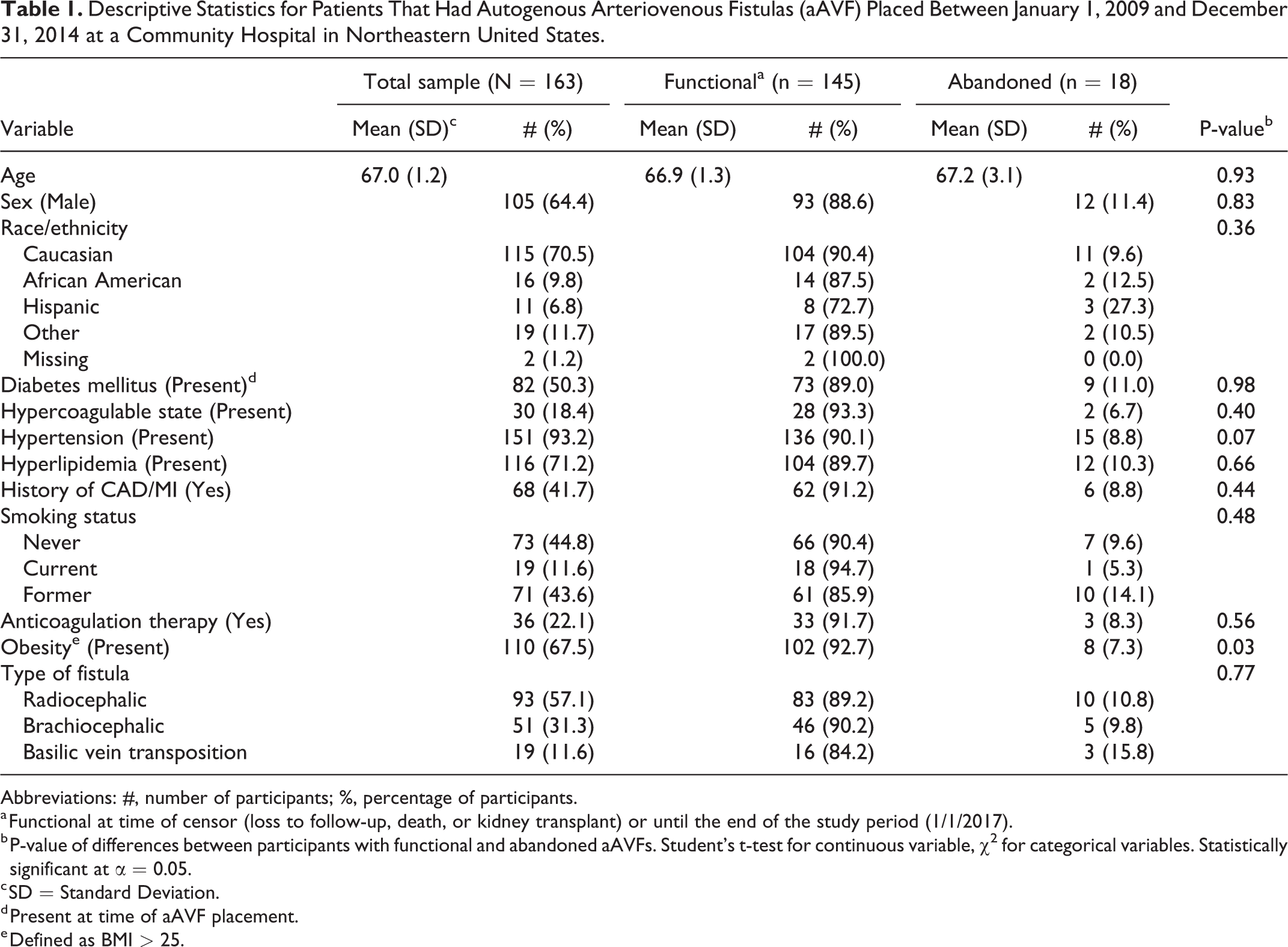
Abbreviations: #, number of participants; %, percentage of participants.
a Functional at time of censor (loss to follow-up, death, or kidney transplant) or until the end of the study period (1/1/2017).
b P-value of differences between participants with functional and abandoned aAVFs. Student’s t-test for continuous variable, χ2 for categorical variables. Statistically significant at α = 0.05.
c SD = Standard Deviation.
d Present at time of aAVF placement.
e Defined as BMI > 25.
Having a pre-dialysis intervention trended toward statistical significance for greater number of interventions (p = 0.061), but did not significantly affect the overall FFP (p = 0.956). Pre-dialysis interventions were not included in the total number of interventions. There was no significant difference between types of interventions, which included balloon angioplasty (PTA), stenting, and AngioJet thrombolysis, with respect to having less than 3 revisions or 3 or more revisions (p = 0.11). Stenting of aAVFs was not performed routinely in our vascular practice, and was reserved for cases where significant contrast extravasation was identified after angioplasty, indicating rupture, or if multiple repeat interventions were required at the cephalic arch. Median FFP was 2.92 years (range 0.098-6.88 years).
Of the 145 patients with functional fistulas, 12 patients (8.3%) thrombosed their fistula 1 or more times, but were successfully treated with endovascular intervention (PTA, stent, and/or thrombolysis), and these fistulas continued to remain patent for as many as 8 years afterward. Median FFP for the group of functional aAVFs was 3.18 years (range 0.01-7.01 years). Median number of interventions for this group was 1 (range of 0-13). Many of these patients continued to have functioning fistulas at the end of the study period, including the fistula having undergone 13 interventions (6.58 years), shown in Figure 1.
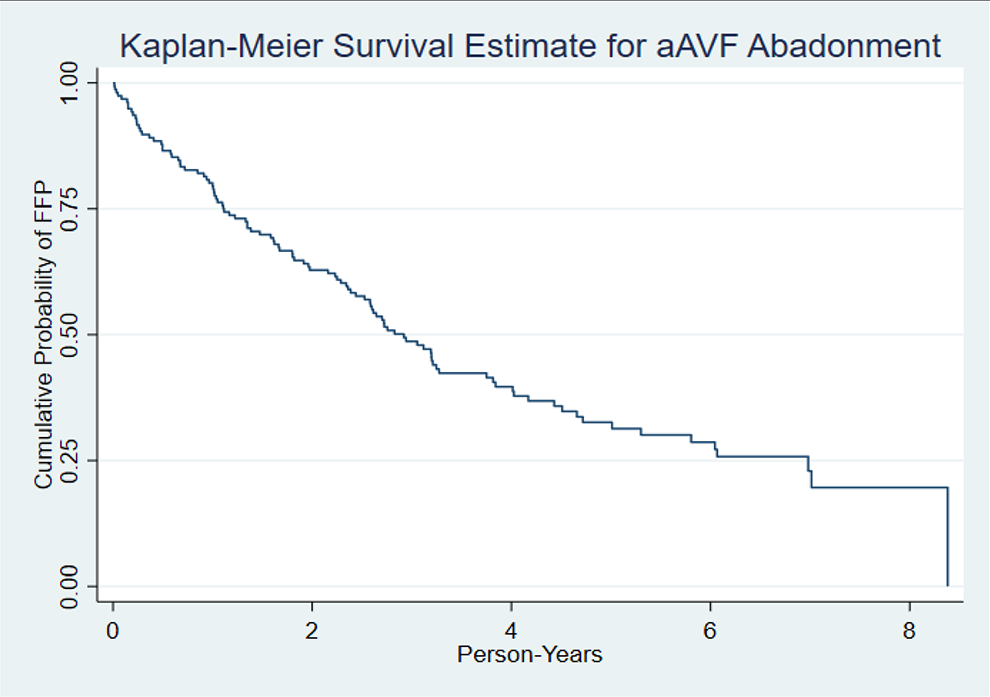
Kaplan-Meier survival curve for autogenous arteriovenous fistula (aAVF) Functional Fistula Patency (FFP) among patients at a community hospital in the Northeastern United States placed between January 1, 2009 and December 31, 2014, and followed until January 1, 2017.
The Kaplan-Meier survival analysis (Figure 1) demonstrated a fairly linear downward trend in cumulative risk for aAVF abandonment across person-years with a steeper decline within the first 2 years. This may be due to the number of deaths that occurred during that time. The mean number of person-days of FFP among patients who died was 653.3 (SD = 82.4), which is approximately 1.7 years. However, the mean number of person-days of FFP among those who did not die was 1320.6 (SD = 70.5), which is approximately 3.6 years. This difference was statistically significant using a Student’s t-test at α = 0.05, with a 2-tailed p-value of 0.001. The probability that an aAVF would remain functional reached 0.5 at approximately 3 person-years. The Kaplan-Meier survival analysis grouped by obesity status demonstrated a significant difference in aAVF survival estimates (log-rank test χ2(1) = 5.63, p = 0.02), as did the analysis grouped by total number of revisions (log-rank test χ2(1) = 4.90, p = 0.03). Patients that were not obese had a much steeper decline in the probability of fistula patency in the first 2 years compared to those who were obese (Figure 2).
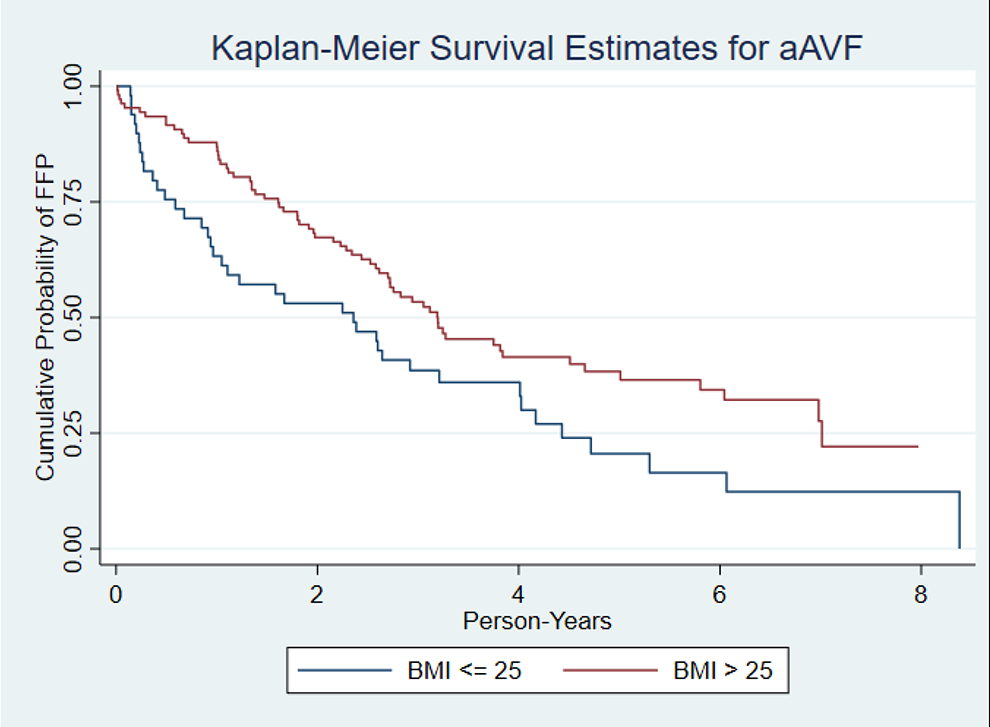
Kaplan-Meier survival curve for autogenous arteriovenous fistula (aAVF) Functional Fistula Patency (FFP) among patients with BMI ≤ 25 and BMI > 25 at a community hospital in the Northeastern United States placed between January 1, 2009 and December 31, 2014, and followed until January 1, 2017.
We verified that all assumptions for logistic regression were met and performed univariate analyzes with each covariate and the primary outcome (aAVF abandonment) to identify predictors to include in our model. We found only obesity was statistically significantly associated with aAVF abandonment (p = 0.04). For multivariable logistic regression, we found that after controlling for age, sex, race/ethnicity, and total number of revisions, the odds that a patient with an aAVF who was obese had the fistula abandoned was 0.32 (p = 0.04, 95% CI = 0.11, 0.92) times that of a person who was not obese, shown in Table 2. In other words, obesity was protective against fistula abandonment. We did not find that race/ethnicity was statistically significantly associated with abandonment, though it was found to be associated with the number of re-interventions.
Results of the Logistic Regression Analysis for the Abandonment of Autogenous Arteriovenous Fistulas (aAVFs) Among Patients With Newly Placed aAVFs Between January 1, 2009 and December 31, 2014 at a Community Hospital in the Northeastern United States (N = 163).
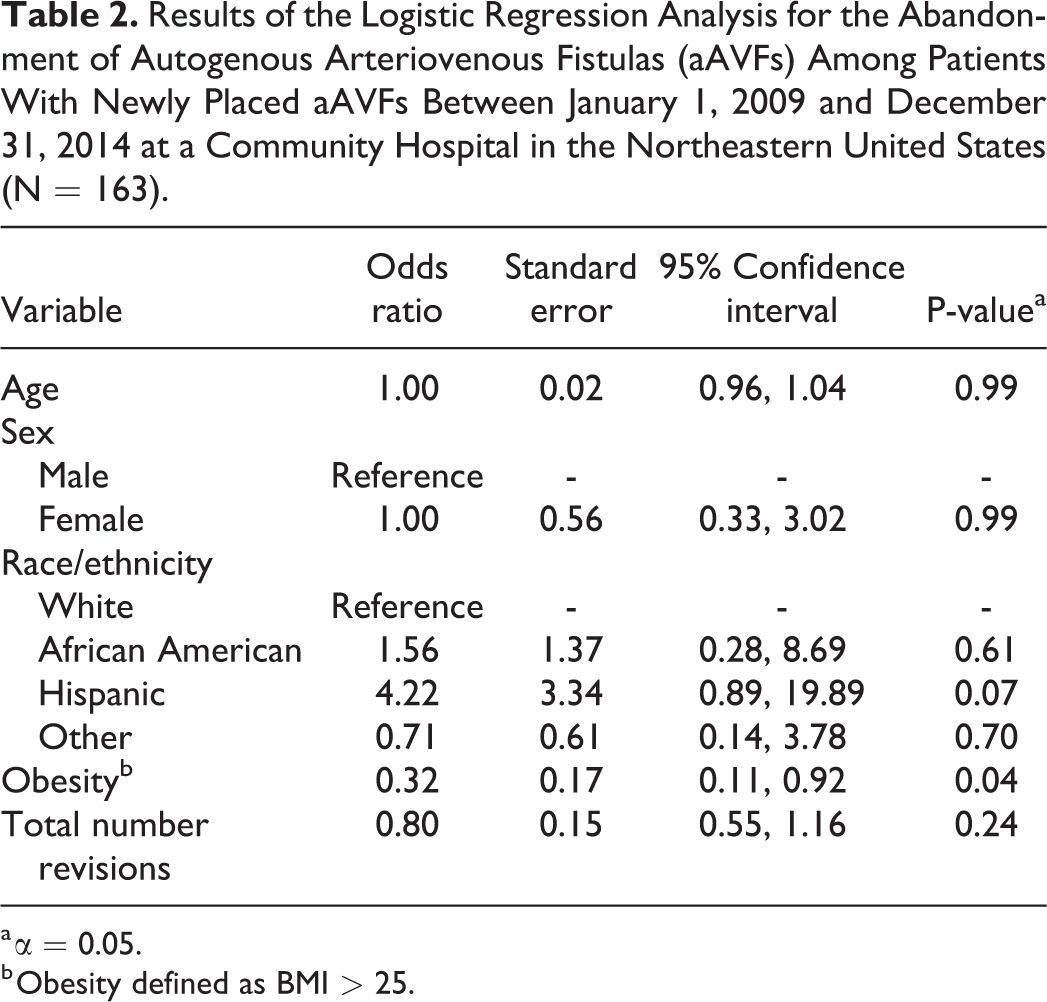
a α = 0.05.
b Obesity defined as BMI > 25.
Of the 18 patients with abandoned fistulas, the most common cause was thrombosis not amenable to endovascular repair (47.1%) and/or surgical revision, and the second most common was infection (23.5%). The median FFP in this group was only 0.91 years (range 0.03-5.30 years). FFP among patients with fistulas that were ultimately abandoned was significantly less than that of patients with functional fistulas (p < 0.0001). Median number of interventions was 0 (range of 0-5). The mean time to abandonment was 1.58 years (SD = 1.38). Of note, the decision to abandon these fistulas was made by the operating vascular surgeon’s assessment that salvage of a viable fistula was unlikely with either an endovascular or open surgical revision.
We found the only covariate that was statistically significantly associated with the total number of aAVF re-interventions when not controlling for any other variables was membership in the “other” race/ethnicity category (p = 0.006). The type of fistula, namely brachiocephalic, was borderline statistically associated with the total number of re-interventions when compared to radiocephalic (p = 0.059). These variables, along with the likely confounders age, sex, and aAVF abandonment, were included in the final negative binomial regression model (Table 3). When controlling for age, sex, aAVF abandonment, and type of fistula, the incidence rate for total number of re-interventions was 0.35 (p = 0.02, 95% CI = 0.15, 0.83) times that of Caucasian participants among those in the other race/ethnicity category. This was the only statistically significant predictor of total aAVF re-interventions and demonstrated a protective relationship when compared to participants in the Caucasian category.
Results of the Negative Binomial Regression Analysis With Zero Inflation for the Total Number of Autogenous Arteriovenous Fistulas (aAVFs) Re-Interventions Among Patients With Newly Placed aAVFs Between January 1, 2009 and December 31, 2014 at a Community Hospital in the Northeastern United States (N = 163).
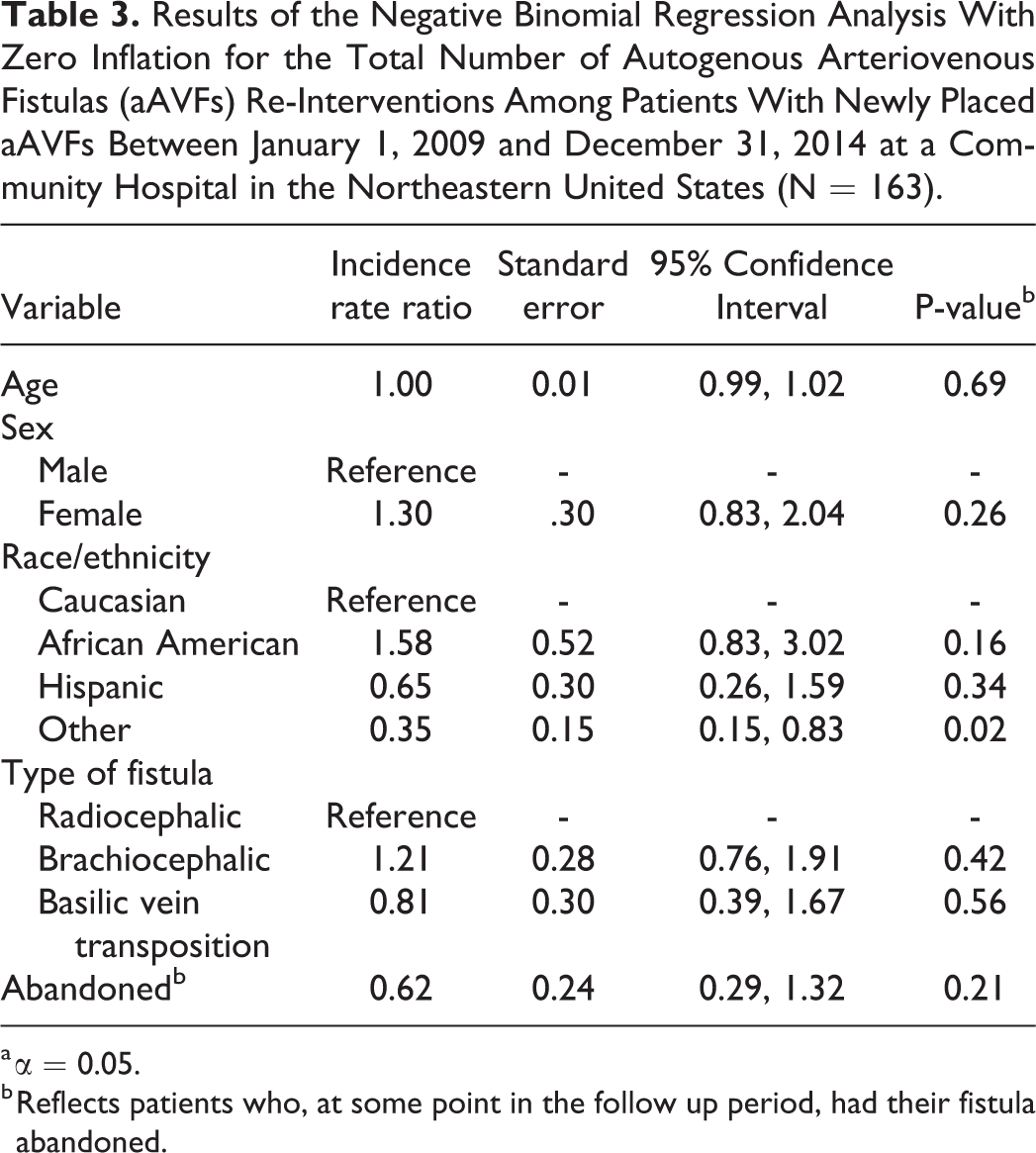
a α = 0.05.
b Reflects patients who, at some point in the follow up period, had their fistula abandoned.
We further evaluated the effect of more numerous interventions and divided our group into those having 2 or less and those with 3 or more (Table 4). While the average number of days between revisions appeared shorter, and thus more frequent, in the
Univariate Comparison of Patient Characteristics Between Patients With aAVFs Intervened on 2 or Fewer Times and Those With 3 or More Interventions (N = 163).
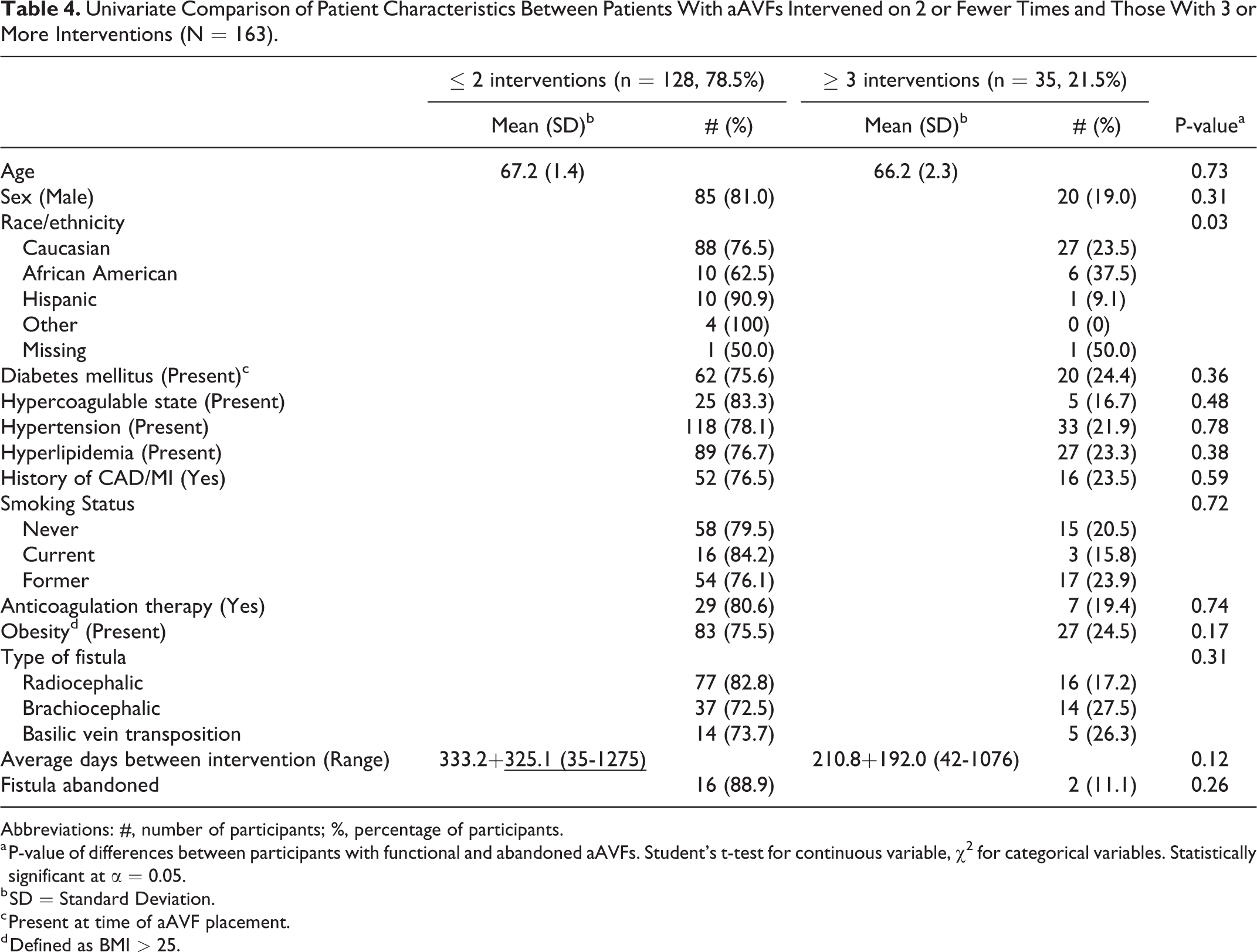
Abbreviations: #, number of participants; %, percentage of participants.
a P-value of differences between participants with functional and abandoned aAVFs. Student’s t-test for continuous variable, χ2 for categorical variables. Statistically significant at α = 0.05.
b SD = Standard Deviation.
c Present at time of aAVF placement.
d Defined as BMI > 25.
Discussion
Vascular access is an increasingly prevalent and continuously evolving issue in vascular surgery today. Autogenous access has proven superior to grafts in outcomes and overall patency.10-18 Gibson et al compared AVF patency and revision rates between autogenous, transposition, and prosthetic grafts, and demonstrated vein transpositions to have similar patency as aAVF but required more re-interventions, and aAVF to have superior patency to prosthetic grafts. 12
The previous KDOQI guidelines to address the management of malfunctioning aAVF recommended intervention if there was a stenosis >50% with clinical symptoms and surgical revision or fistula abandonment if more than 2 angioplasties are required within 3 months.11,19 It was also suggested that thrombosis of an aAVF is not only difficult to treat, but that outcomes are poor with both percutaneous and open surgical interventions. 11 The 2019 updated KDOQI guidelines are even less specific, and simply recommend surgical revision after endovascular failure, lesions not amenable to endovascular treatment, and situations where surgical outcomes are markedly better; however, there is still no clear criteria for when to abandon a dysfunctional fistula. 9 Likewise, and with even less clarity, the most recent (2008) SVS guidelines recommend only that intervention, by endovascular, open surgical or combined means, be performed to maintain or restore access patency. 10
Several published reports have evaluated secondary interventions and their effect on fistula patency.8,20-24 Bountouris et al examined repeated endovascular interventions performed on AVF over a 12-month period, and determined that they have similar durability, with a primary assisted patency of 85%, to that of primary patency. 21 Yet, in other studies, lower 1-year patency rates have been reported after repeated interventions. Biuckians reported a 63% functional patency, which was defined as “the interval from when the AVF was cannulated until abandonment or the time of measurement of patency, including the time after any intervention to maintain or reestablish function,” 20 and a 74.6% primary assisted patency. 8 Unfortunately, however, outcomes of repeated endovascular interventions on patency are often not specified or included in analysis, and when included, are often limited to no more than 3 interventions.8, 20-23 Still missing from the literature are clear guidelines with respect to the safety and/or patency of aAVF which have undergone repeated endovascular interventions. Nor are there recommendations as to whether there should be a maximum number of interventions or revisions performed on the malfunctioning aAVF prior to consideration of abandonment.10,11,14,17,19 Our findings suggest repeated and/or more frequent endovascular revisions may extend the FFP of aAVF, and possibly delay—or even prevent—abandonment.
Our study reports a median FFP for aAVFs as 3.18 years (range 0.01-7.01 years), with a median of 1 intervention (range of 0-13). One fistula has required 13 interventions and is still in use with a FFP of 6.58 years. Somewhat surprisingly, we did not always find that intervals between interventions consistently decreased with increasing numbers of interventions. This and other patients in our study who have long term functioning fistulas despite multiple interventions confirm for us our belief that there should be no limitation to the number of interventions performed. We would expect minimal risk associated with multiple interventions as there is usually no general anesthetic component required, and can be performed under minimal to no sedation. While this frequency is presently unknown with certainty, we have elected to follow KDOQI suggestions, which recommend revision or abandonment of aAVF which require more than 2 interventions within a 3-month period.4-6 Nevertheless, a relatively small percentage, 11%, of aAVFs in our study were abandoned, most commonly as a result of thrombosis. We also found obesity to be protective against fistula abandonment. In reviewing our data points, we were unable to determine the cause of this finding. The literature has established a clear association between obesity in dialysis patients and improved survival.25,26 This paradoxical association has multiple theories, such as a reduced concentration of inflammatory mediators and endotoxins (which have deleterious effects on the cardiovascular system) due to absorption by adipose tissue.25,26 We question if there is another obesity paradox at play with our finding of decreased abandonment in obese patients; future research is required to better examine this association. None of the fistulas in our study were abandoned because of an unacceptable rate of reintervention. Median FFP of abandoned aAVFs was 0.91 years (0.03-5.30 years), with interventions ranging from 0 to 5 in number. These results may indicate repeated and/or more frequent revisions do not negatively affect the FFP nor do they increase the overall risk for abandonment of aAVFs. Should these findings be corroborated in a larger prospective study, they could be applied to various clinically relevant scenarios, such as patients who are not transplant candidates, or have failed transplantation, young patients, or those with limited access options. Specifically, in these patients, who may require hemodialysis for many years, our small study shows some evidence that repeated attempts at preservation of autogenous access is worthwhile, safe, and not futile. A functioning hemodialysis access (HA) is a crucial lifeline for the majority of patients with ESRD. The essential challenge to the vascular surgeon treating these patients is to maintain the functionality of HA for as long as possible while navigating the fine balance between aggressive intervention and the risks to patient health that these interventions may incur. Through repeated interventions on aAVF, none of the patients in our study exhausted all hemodialysis access options prior to transplantation, death or loss to follow-up.
Given the retrospective nature of our study and small power, larger, prospective studies will be necessary to fully substantiate our findings.
Footnotes
Acknowledgments
Presented at: Eastern Vascular Society (EVS), Oral Presentation, October 2017, Savannah GA. Society for Vascular Surgery (SVS), Poster Presentation, May 2017, San Diego CA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.