
Abstract
Objective:
Aortic aneurysms and dissections are prevalent causes of morbidity and mortality. The management of aortic pathologies may be called into question in malpractice suits. Malpractice claims were analyzed to understand common reasons for litigation, medical specialties involved, patient injuries, and outcomes.
Methods:
Litigation cases in the Westlaw database from September 1st, 1987 to October 23 rd, 2019 were analyzed. Search terms included “aortic aneurysm” and “aortic dissection.” Data on plaintiff, defendant, litigation claims, patient injuries, misdiagnoses, and case outcomes were collected and compared for aortic aneurysms, aortic dissections, and overall cases.
Results:
A total of 346 cases were identified, 196 involving aortic aneurysms and 150 aortic dissections. Physician defendants were emergency medicine (29%), cardiology (20%), internal medicine (14%), radiology (11%), cardiothoracic (10%) and vascular surgery (10%). Litigation claims included “failure to diagnose and treat” (61%), “delayed diagnosis and treatment” (21%), “post-operative complications after open repair” (10%) and “negligent post-operative care” (10%). Patients with aneurysms presented with abdominal (63%) and back pain (37%), while dissections presented with chest pain (78%), abdominal pain (15%), and shortness of breath (14%). Misdiagnoses included gastrointestinal (12%), other cardiovascular (9%), and musculoskeletal conditions (9%), but many were not specified (58%). Overall, 83% of cases were wrongful death suits. Injuries included loss of consortium (23%), emotional distress (19%), and bleeding (17%). In 53% of the cases, the jury ruled in favor of the defendant. 25% of cases ruled for the plaintiff. 22% of cases resulted in a settlement. The mean rewarded for each case was $1,644,590.66 (SD: $5,939,134.58; Range: $17,500-$68,035,462).
Conclusion:
For aortic pathologies, post-operative complications were not prominent among the reasons why suits were brought forth. This suggests improvements in education across all involved medical specialties may allow for improved diagnostic accuracy and efficient treatment, which could then translate to a decrease in associated litigation cases.
Introduction
Aortic pathologies, including aneurysms and dissections, are prevalent causes of mortality in the United States (US). Abdominal aortic aneurysms (AAA) are the 14th leading cause of death in the United States 1 with ruptured AAA (rAAA) carrying an overall mortality rate of about 80%. 2 Of patients with rAAA who reach the hospital, approximately 50% do not survive open repair. 1 Survival for rAAA has improved for those undergoing endovascular repair with about 75-80% patient survival.3,4 Acute aortic dissections occur with an incidence of 10 cases per 100,000 per year. 5 For acute dissections, up to 21% of patients may die before hospital admission and mortality remains high if left untreated.6,7 Despite severity, prompt recognition and treatment of aortic aneurysms and dissections remains problematic, with delayed management resulting in worse patient outcomes.8-11
Given the incidence of injury and death, aneurysms and dissections are a source of malpractice lawsuits for multiple medical specialties. Malpractice cases function to determine if a physician deviated from the standard of care for a patient, and compensate for injury accordingly.12-14 The 4 legal elements that determine physician negligence are a professional duty owed to the patient, breach of such duty, an injury caused by the breach, and resulting damages to the patient. 15 For vascular surgeons, aortic interventions account for approximately 11% of procedures leading to litigations. 16 Previous reviews have focused on litigation in relation to various topics in vascular surgery17-20 and other areas of medicine,12,21 but malpractice claims in aortic aneurysms and dissections have not been extensively analyzed thus far.
This study aimed to evaluate litigation in relation to aortic aneurysms and aortic dissections. We sought to further understand the common specialties involved in malpractice lawsuits, presenting symptoms of patients, common misdiagnoses, patient injuries/death, surgical interventions, and financial outcomes of the cases.
Methods
The online legal database Westlaw (West Publishing, St Paul, MN, USA) that contains relevant details and outcomes on all malpractice cases settled within the United States legal system. The database was queried for all jury verdicts and settlements pertaining to aortic pathologies using the search terms “aortic aneurysm” and “aortic dissection” to identify relevant malpractice lawsuits. Westlaw is a proprietary database service that allows identification of specific terms from legal reports using natural language and Boolean search techniques. It is inclusive of all malpractice cases in the country and requires purchase to access the database. The Westlaw database provides a comprehensive case sample of all cases litigated on specific topics in medical malpractice. The Westlaw database only covers voluntarily reported verdicts from cases that went to trial or settlement negotiations. Cases settled out of court were obviously not available for inquiry. Each malpractice case provides a summary report of relevant information including, plaintiff, defendant, jurisdiction, expert witness, monetary outcome, and case details. Verdict reports are submitted voluntarily by attorneys or their staff. No personal or protected health information is included in the database or reports and thus institutional review board approval was not required. We chose Westlaw over LexisNexis or other databases, since it has been proven to provide reliable analysis in malpractice cases in various medical specialties via data generated from jury verdict reports,22-24 including obstetrics and otolaryngology.
Cases in the Westlaw database from September 1st, 1987 to October 23 rd, 2019 were included in analysis. Cases were screened for relevance by 3 reviewers independently and compared to confirm the lawsuits to be included in analysis. Relevant cases included those in which the allegation was negligence by a physician or hospital in the management of a patient presenting with a chief complaint secondary to an aortic aneurysm or aortic dissection and the subsequent management of that patient. Duplicate cases were excluded.
Data was compiled on the date of the injury, verdict date, and defendant, including defendant medical specialty. Data on the plaintiff was collected including demographics, presenting symptoms, surgical management if any, and if there was a misdiagnosis. Misdiagnoses were further categorized to include gastrointestinal (GI), other cardiovascular (CV), pulmonology, genitourinary (GU), infectious disease, musculoskeletal (MSK), neurological, and misdiagnosis not specified.
General categories were established to identify the claim for the case, including failure to diagnose and treat, delayed diagnosis and treatment, lack of informed consent, negligent surgery, intra-operative complications, post-operative complications, and negligent post-operative care. Patient injuries and death were also compiled. Loss of consortium (the deprivation of the benefits of a family relationship due to injuries caused by the defendant’s actions) was referenced frequently in the cases. Outcome of cases defined as ruling for defendant, plaintiff, or settlement were collected. The amount awarded to the defendant and jury fees for each case were recorded. Analysis of the number of malpractice cases per year was also performed.
All descriptive statistics, chi-square, and t-tests were performed using Microsoft Excel (version 16.4). All p-values are in reference to the comparison between aortic aneurysm and aortic dissection litigation cases. Given the deidentified nature of the dataset and the retrospective design, Institutional Review Board approval and informed consent were waived.
Results
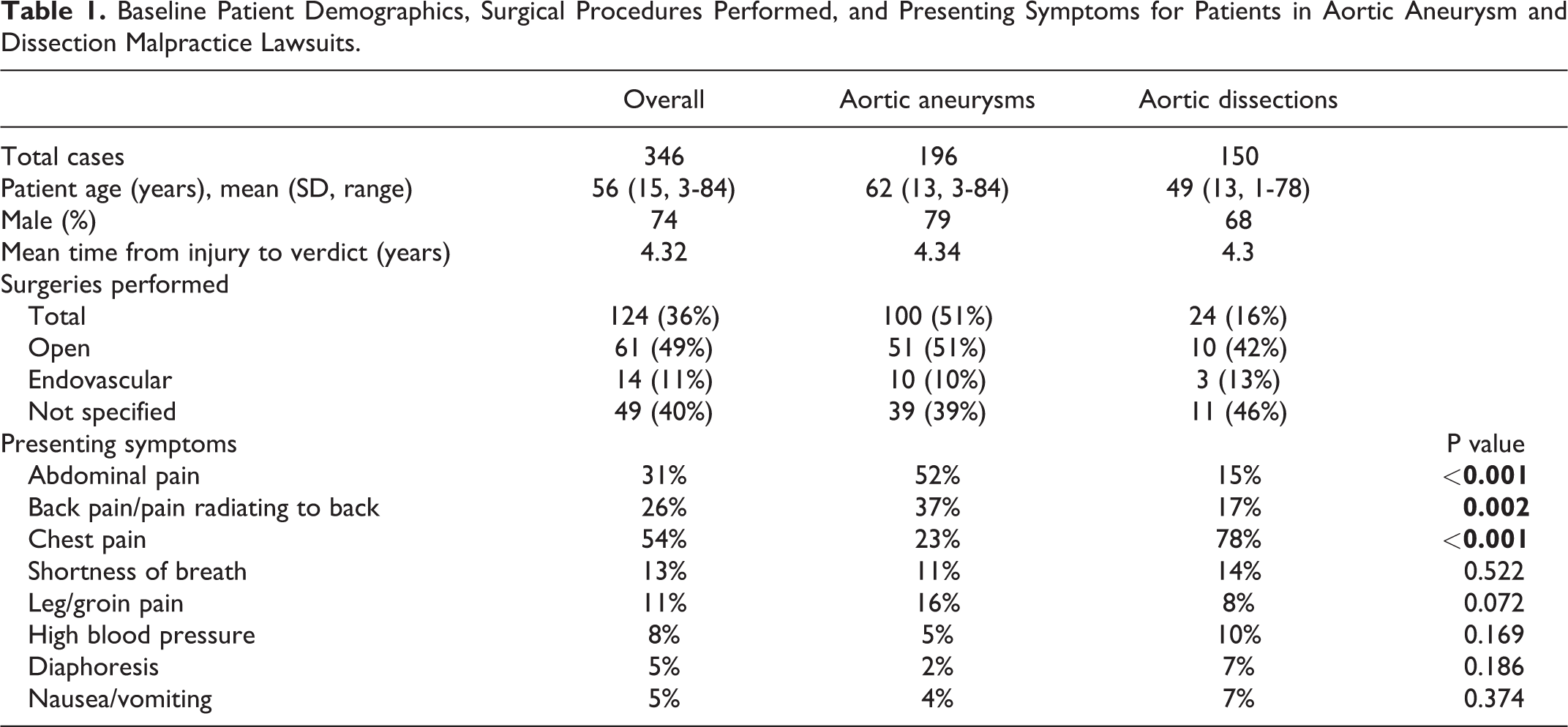
A total of 346 cases were identified, with 196 involving aortic aneurysms and 150 aortic dissections. Plaintiffs were predominantly male (74% overall) (Table 1). The average age of the patient was 56 years old, with dissection patients being younger than aneurysm patients [49 (SD 13) vs 62 (SD 13) years, p = <0.001]. Of all aneurysm cases, 24% were asymptomatic, 31% were symptomatic, and 45% were ruptured. The majority (75%) of dissection suits did not further describe the dissection anatomically. Of the 38 cases with this data, 31 were type A dissections (82%) and 7 were type B dissections (18%). The mean time from the date of injury to the verdict date was 4.32 years for all aortic malpractice lawsuits included in the study.
Baseline Patient Demographics, Surgical Procedures Performed, and Presenting Symptoms for Patients in Aortic Aneurysm and Dissection Malpractice Lawsuits.
Defendants included hospitals, physicians, or both. Overall, 187 cases (54%) listed the hospital as the defendant, 299 cases (86%) listed a physician and 55 (16%) included another party (e.g. nurses or paramedics) as the defendant. When physicians were included as defendants, 202 cases listed only 1 physician and 97 listed multiple physicians. Defendant specialty was compiled and stratified by pathology (Figure 1). The most frequently identified physician defendants were emergency medicine (29%), cardiology (20%), internal medicine (14%), radiology (11%), cardiothoracic surgery (10%) and vascular surgery (10%).
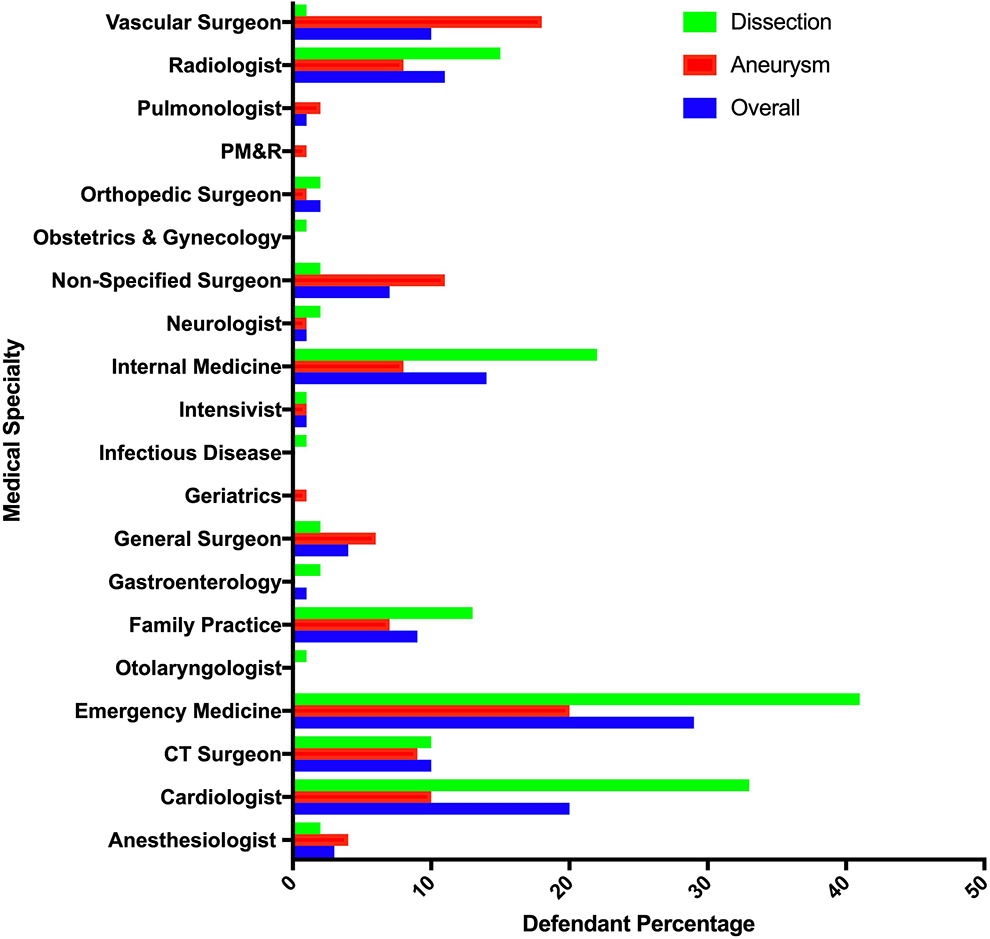
Physician defendant composition stratified by overall cases, aortic aneurysm, and aortic dissection cases.
Claims in each malpractice lawsuit were collected and also stratified by pathology (Figure 2). The majority of litigation suits claimed “failure to diagnose and treat” (61%), “delayed diagnosis and treatment” (21%), post-operative complications after open repair (10%), and negligent post-operative care (10%). Post-operative complications included arterial injuries, injuries to bowel, lower extremity ischemia, infection and rare complications due to negligent surgeries, including leaving a towel in the abdominal cavity. Negligent post-operative care included the immediate post-operative period where patient was not monitored properly by hospital staff, resulting in patient injury, or the failure of the physician to monitor for post-operative complications in the immediate and prolonged post-operative period. The claim of “failure to diagnose and treat” was more prevalent for aortic dissections than aortic aneurysms (73% vs. 52%, p =<0.001).
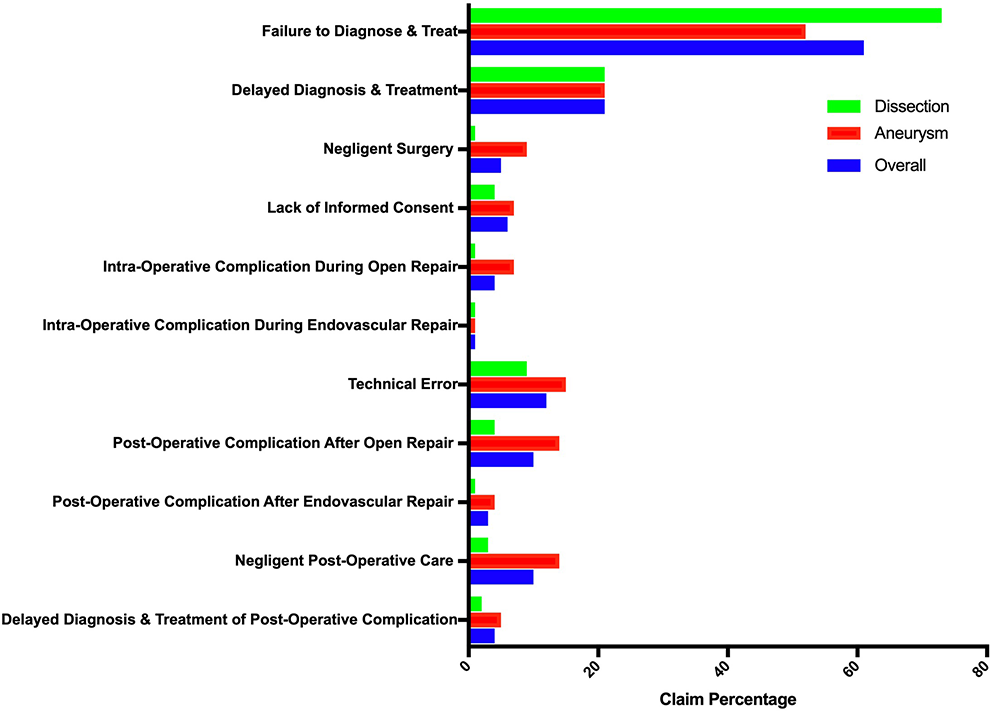
Percentage negligence claims for each litigation case stratified by overall cases, aortic aneurysm, and aortic dissection cases. Some cases may involve more than 1 negligence, so the values sum to over 100%.
Overall, 186 malpractice lawsuits described patient presenting symptoms, with 81 aneurysm and 105 dissection cases included (Table 1). The most common complaints overall were chest pain (54%) and abdominal pain (31%). The majority of patients with aneurysms presented with abdominal pain (52%) and back pain/pain radiating to the back (37%). Aortic dissection cases presented typically with chest pain (78%), abdominal pain (15%), and shortness of breath (14%). Rare complaints included lower limb ischemia (2%), arrhythmia (1%), and altered mental status (1%). Patient misdiagnoses are detailed in Table 2. Overall misdiagnoses in aortic cases included GI (12%), other CV conditions (9%), and MSK diagnoses (9%). Many misdiagnoses were not specified (58%) and few involved death prior to any diagnosis (1%).
Misdiagnoses and Patient Injuries Reported in Malpractice Lawsuits for Aortic Aneurysms and Aortic Dissections.
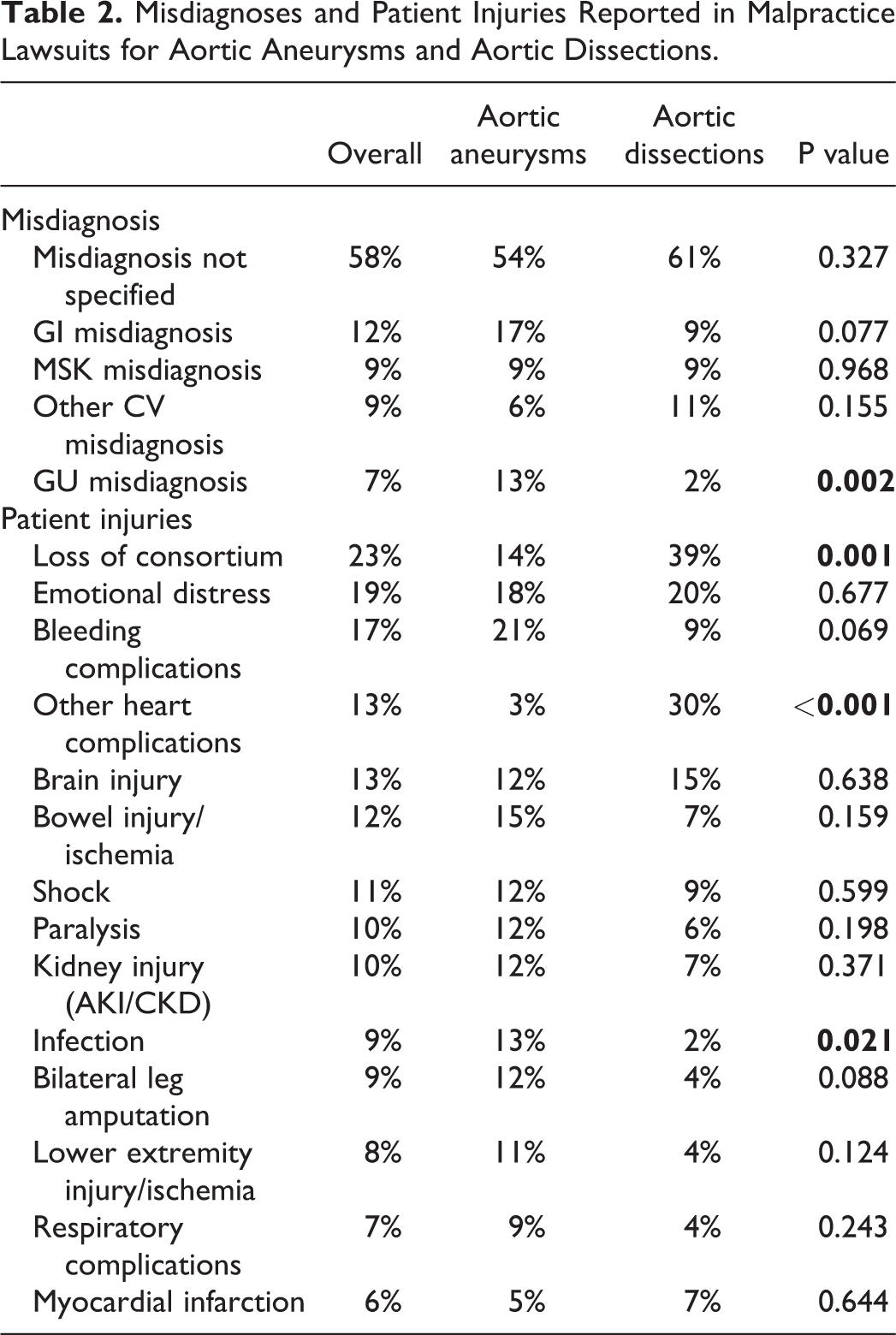
Overall, 36% of patients in the cases underwent surgery at the time of presentation or during the time period where a post-operative complication occurred as a result of the procedure −51% of aneurysm cases and 16% of dissections. A majority of litigation cases involved open surgery (49%) or those in which the type of surgery was not specified (40%) (Table 1). Patient death occurred in 83% of litigation cases, specifically 74% of aneurysm and 94% of dissection cases. The most common injuries reported were loss of consortium (23%), emotional distress (19%), and bleeding complications (17%) (Table 2).
Analysis of the number of malpractice cases over time displays a majority of lawsuits occurring in the early 2000’s (Figure 3). Most aortic litigation cases occurred in 2005 (23 cases), 2003 (17 cases), 2002 (17 cases) and 1997 (16 cases). Malpractice lawsuits were infrequent in the 1980s (1-4 cases) and ranged from 5-12 cases from 2010 to 2019.
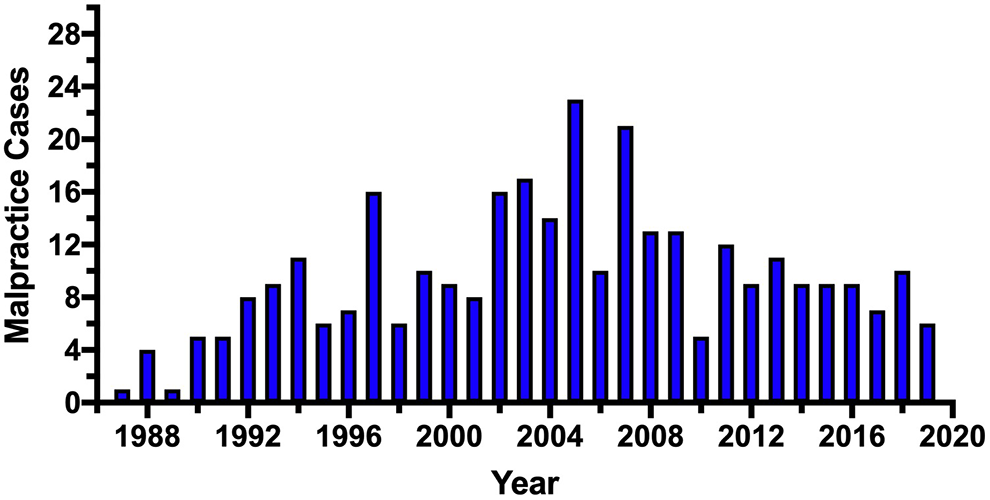
Number of malpractice cases per year for aortic aneurysm and aortic dissection litigation cases from 1987 to 2019.
Verdicts were found for the defendant in 53% of cases with 25% ruled in favor of plaintiff, and 22% went to settlement. For aneurysms, 48% ruled for defendant, 30% for plaintiff, and 22% settlement. For dissections, 59% ruled in favor of the defendant, 17% for plaintiff, and 24% went to settlement. The mean amount rewarded for each case overall was $1,644,590.66 (SD: $5,939,134.58; Range: $17,500-$68,035,462). The case resulting in $68,035,462 rewarded the plaintiff involved an open AAA repair, where the surgeon left the OR and the hospital prior to the completion of the case, where other hospital staff was left to close the abdomen. This resulted in bleeding complications and hypovolemic shock, where the patient coded and was placed on cardiopulmonary bypass. The surgeon was not immediately available to address these complications and returned to the hospital after the patient had coded. The mean amount rewarded for aneurysm cases was $1,795,018.65 (SD: $7,078,901.79; Range $17,500-$68,035,462). The mean amount awarded for dissection cases was $1,337,007.19 (SD: $1,505,899.63; Range: $96,000-$6,500,000).
Discussion
Investigation of malpractice litigation provides insight to the relevant issues in patient care faced by the medical community. The majority (82%) of malpractice lawsuits for aortic aneurysms and aortic dissections claimed “failure to diagnose and treat” and “delayed diagnosis and treatment.” These delays in diagnosis do not appear to be contributed to hospital transfers, but occurred primarily in the emergency department of the initial hospital or outpatient clinic that the patient first presented to with symptoms. These observed errors in diagnosis in malpractice cases are reflective of the past and current challenges of providing a timely diagnosis for aortic dissections25,26 and ruptured/symptomatic aneurysms27,28 upon presentation to the hospital.
Overall, only 346 malpractice cases proceeded to litigation over the 32 year span of this study. With approximately 16,000 AAA repairs occurring in the US annually 29 and approximately 2,000 new cases of aortic dissections annually, 30 this correlates to about 0.01% of AAA and aortic dissection cases resulting in malpractice trials. This a small fraction of litigation cases in comparison to the overall incidence of aortic pathologies in the United States. The highest amount of malpractice cases occurred in the early 2000’s, despite improvements and availability of imaging studies, including ultrasound duplex and computed tomography angiography (CTA).31-33 This correlates with a peak in overall malpractice lawsuits in the US in the early 2000’s, with approximately 20,000 cases in 2001 (Figure 4). 34 The number of malpractice litigation cases has consistently decreased since then.
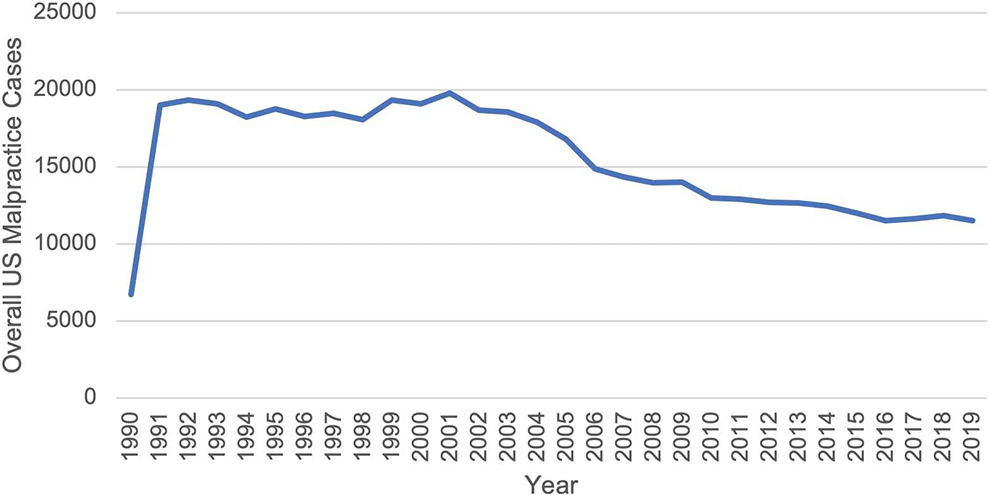
Number of malpractice cases per year for overall litigation cases in the United States from 1987 to 2019.
As reflected in aortic malpractice cases, many patients received a misdiagnosis at the time of presentation (Table 2) with a wide differential. This is likely secondary to the varying symptoms reported by patients suffering for aortic aneurysms and dissections (Table 1). It estimated that up to 1 third of patients suffering from aortic dissection 35 and 1 third to 1 half of all ruptured AAAs36,37 are initially misdiagnosed in the emergency room. GI diagnoses were the most common likely given the frequency of abdominal pain as the chief complaint. This is surprising, given the use of CT scans in the diagnosis of patients presenting with non-specific abdominal pain to the ED. Despite CT scan resulting in the correct clinical diagnosis up to 87% of the time of patients with non-traumatic abdominal pain in the emergency department, 38 it is currently utilized for only about 54% of patients presenting with these symptoms. 39 Increase utilization of CT scan in patients with abdominal pain and relevant risk factors could be 1 way to decrease the incidence of missed AAA and aortic dissections in the emergency department. As reflected with a higher prevalence of “other CV misdiagnosis” for aortic dissections, initial misdiagnosis of acute myocardial infarction in patients with dissections also remains a concern.26,35,40
It is not surprising that with the initial diagnosis as the major challenge in the management of these patients, emergency medicine providers were the most affected specialty for all aortic aneurysm and dissection malpractice lawsuits. Internal medicine, cardiology, and radiology were more likely to be involved in aortic dissection cases (Figure 1). This may reflect the need for a high index of suspicion to adequately establish a diagnosis of aortic dissection with advanced testing and imaging.11,41 Meanwhile, vascular surgeons and other non-specified surgeons were more likely to be involved in aneurysm cases. This highlights the importance of being vigilant for post-operative complications after aortic aneurysm repair.42-44
Failure to timely diagnose and treat patients with aortic aneurysms and aortic dissections is not only detrimental and potentially fatal to the patient, but also results in suffering for family members, as detailed by “emotional distress” and “loss of consortium” being prevalent reported injuries.
While most malpractice claims brought against US doctors and US hospitals are either found in favor for the defense or abandoned prior to settlement or adjudication45,46 this was not observed in our analysis of aortic litigation cases. This could be due to the severity of injury correlating with the likelihood of financial compensation47-49 and a high degree of injury and death observed in aortic aneurysm and dissection cases. Furthermore, given the large percentage of verdicts in favor of the plaintiff, large percentage of settlements, and substantial sums awarded, aortic malpractice lawsuits represent a substantial cost to the healthcare system in addition to the patient’s morbidity and mortality. Overall, 86% of aortic malpractice lawsuits involved the physician as a defendant. The physician’s name remaining in the lawsuit, even in cases where the hospital is included as a co-defendant, shows a significant level of responsibility being placed on the defendant physician in aortic malpractice cases.
These patterns observed in aortic malpractice lawsuits, are consistent with persistent difficulties in improving our ability to diagnose cardiovascular emergencies. 50 Coordinated efforts by multiple medical specialties may result in more effective identification and diagnosis of these pathologies. This includes multimodal assessment, imaging studies, and timely admission to the OR as required. 51 Improving education, specifically by addressing cognitive biases about aortic emergencies, into the curriculum of residency programs of all clinicians involved in the care of patients in the emergency room may represent 1 potential solution. 52 Recommended AAA screening protocols have been another solution to identify and monitor asymptomatic AAAs in high risk individuals, and ideally repair prior to rupture. 53
This study is limited in that only the Westlaw database was used. Additionally, details regarding individual medicolegal disputes were submitted by attorneys or staff without medical training. This could result in omission of significant medical details from the case. Additionally, since verdict reports are voluntarily submitted, it is possible that some cases that went to trial were not included in the database. Furthermore, many malpractice lawsuits are frequently resolved by arbitration and do not proceed to trial. Cases settled out of court were not available for inquiry. Thus, it is possible that our sample does not represent the whole scope of claims resulting in malpractice lawsuits for aortic aneurysm and dissections. This only represents a small portion of malpractice claims as jury verdict reporting services do not publish every decision. Despite its limitation in the number of cases recorded, this study provides a representative snapshot of the current legal environment. Given the greater than 40 year range of cases and the included cases level of detail, we feel confident this study is an accurate representation of the litigation involving aortic procedures. Finally, data is limited in the full analysis of misdiagnoses with multiple cases failing to specify the exact initial misdiagnosis that was given to the patient at the time of first presentation. Despite these limitations, we believe the cases provide a real-world sample, as prior studies have estimated that jury verdict reporters capture over 75% of cases and thus this study is a reflection of commonly encountered causes for malpractice litigation in the management of aneurysms and dissections 22 This work is hypothesis generating overall and highlights the need for further investigation in the field.
Conclusion
The majority of malpractice lawsuits of aortic aneurysms and aortic dissections were centered on claims of “failure to diagnose and treat” (61%), “delayed diagnosis and treatment” (21%), post-operative complications after open repair (10%), and negligent post-operative care (10%). Misdiagnoses commonly occurred and presenting symptoms varied among patients. In 47% of the cases, rulings were in favor of the plaintiff or settlement with an average reward of $1,644,590.66. The trends of malpractice cases involving aortic disease highlight ongoing difficulties in reducing diagnostic errors for these conditions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.