
Abstract
Several treatment options exist for acute intra-abdominal arterial thromboembolic events, including systemic thrombolytics, endovascular therapy, and less commonly surgery. A novel alternative treatment intervention for acute intra-abdominal arterial thrombus is the use of stent retriever (SR) devices, tools traditionally applied for treatment of acute vascular thrombosis in stroke patients. This brief report presents two cases of acute intra-abdominal arterial thrombosis successfully managed by deployment of SRs. Furthermore, it details the history, device mechanism, and design of SRs and describes cases in literature involving effective extracranial SR application.
Introduction
Acute arterial thromboembolic events are uncommon yet associated with high morbidity and mortality. The incidence of acute thromboembolic events involving the renal artery is .003%–.004% and .1% for acute mesenteric arteries. 1 These patients clinically present with nausea, vomiting, abdominal pain, and, in cases involving acute renal stenosis, with hypertension and hematuria. 2 A serious complication of acute arterial thromboembolic events is visceral infarct, making quick, appropriate management essential. The therapeutic window for renal infarct is variable and ranges from as little as hours to up to several days, 3 with better prognosis seen in patients demonstrating collateral reserve such as in patients with a history of chronic arterial stenosis. 4 Similarly, complete occlusion of the mesenteric arteries can cause irreversible ischemia in as little as 6 hours. 5 Treatment options include systemic thrombolytic, endovascular therapy, and less commonly surgery. 1 Specifically, interventional radiologists have previously implemented direct thrombolysis, aspiration, stenting, angioplasty, snaring, and rheolytic mechanical thrombectomy as a form of endovascular treatment. 6 Surgery is less common due to its higher morbidity and mortality but should be considered in patients with peritonitis or with evidence of infarcted bowel as it allows for direct bowel exploration and potential resection. 5
Innovative means of removing intra-abdominal arterial occlusions have included the off-label use of stent retrievers (SRs), endovascular tools traditionally used for management of intracranial vascular thrombosis in patients with acute strokes. This brief report presents the successful treatment of two cases of acute intra-abdominal arterial thrombosis—involving the renal artery and the superior mesenteric artery (SMA)—through the use of SR devices. SRs can serve as second-line tools for peripheral non-cerebrovascular thrombectomy as described in prior cases in the literature.
Case Reports
These single-institution case reports were exempted from approval by the institutional review board.
Case 1
An 83-year-old woman presented to the emergency department a few hours following sudden abdominal pain and vomiting. Her medical history included hypertension, hyperlipidemia, atrial fibrillation (off anticoagulation medication due to poor patient compliance), aortic stenosis status post prior aortic valvuloplasty, and mild pulmonary hypertension. The patient’s vital signs were solely notable for mildly elevated blood pressure, and labs results showed an elevation of creatinine to 1.1 from a baseline of .9. Routine venous phase CT abdomen and pelvis showed symmetric, normal-sized kidneys with lack of enhancement of a majority of the right kidney as well as abnormal enhancement of the mid to distal right renal artery, concerning for renal infarct, likely acute given the lack of significant right renal parenchymal volume loss. Figure 1. Given the acute presentation and concern for renal function compromise, a plan for endovascular thrombectomy (EVT) with interventional radiology was made, with interim initiation of heparin drip in order to prevent further clot formation. The patient was taken for EVT approximately 12 hours following diagnosis. A contrast-enhanced coronal CT abdomen image demonstrates right renal infarct and a filling defect in the right renal artery.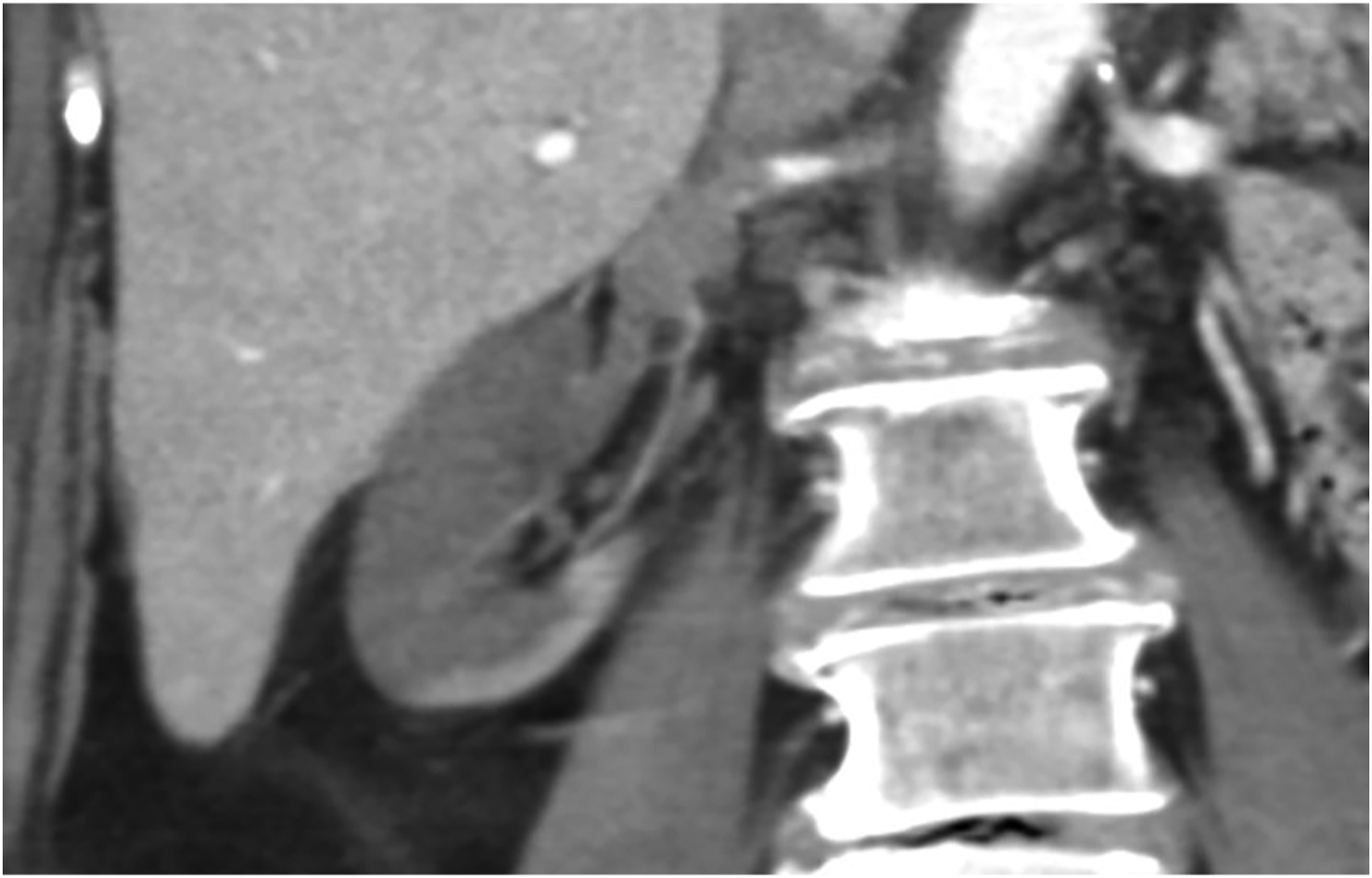
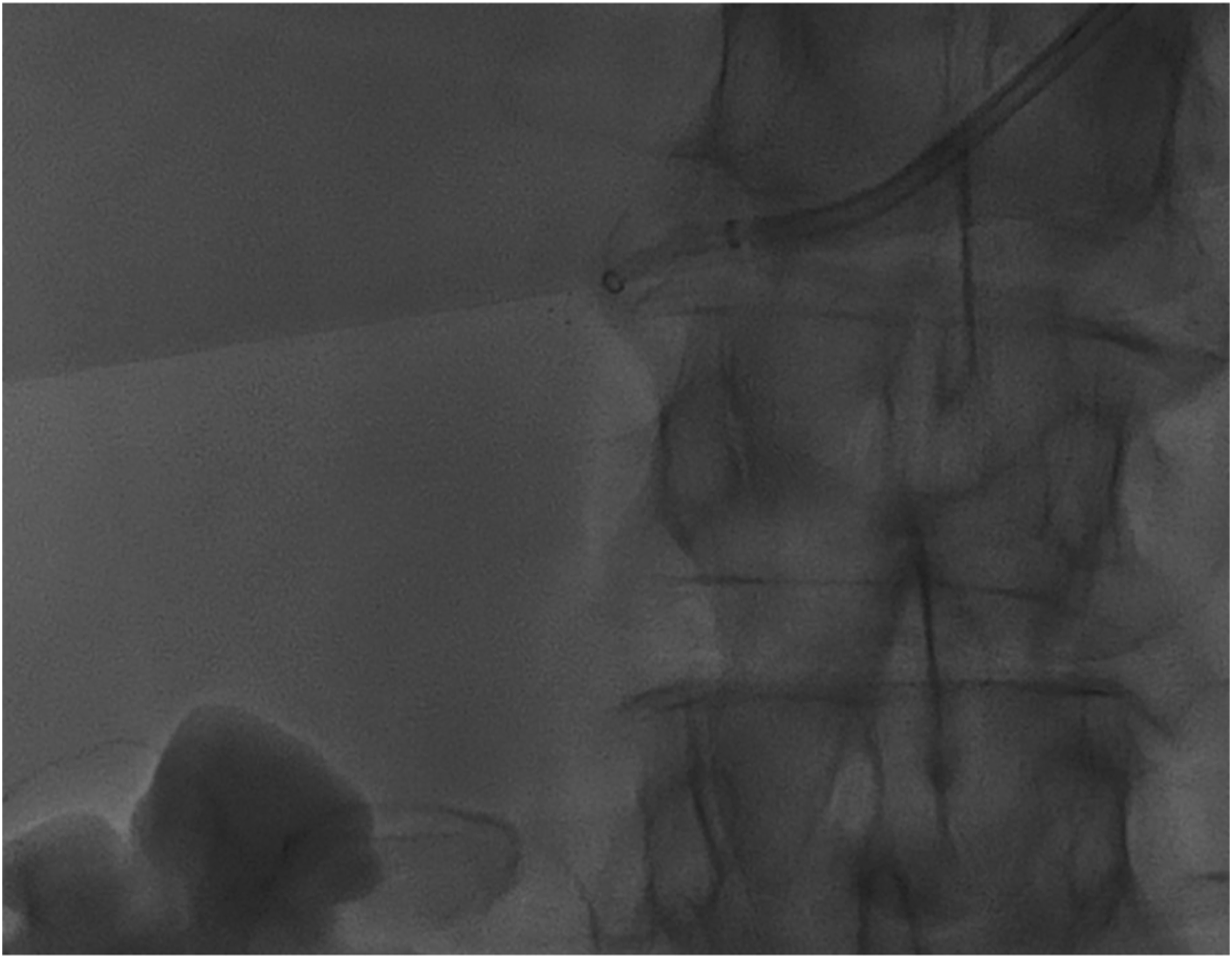
Vascular access was obtained using the left radial artery with a 5F Glidesheath (Terumo, Somerset, New Jersey). A .035 wire and 5F x 110 cm Sarah radial catheter (Terumo, Somerset, New Jersey) was positioned at the proximal right renal artery. An angiogram demonstrated a filling defect up to the level of the distal second order branches of the right renal artery. Figure 2. For increased stability and decreased risk of damaging the arterial lumen, an exchange was made for a 6F x 90 cm Pinnacle Destination guiding sheath (Terumo, Somerset, New Jersey) and 6F Sofia Glidecath (MicroVention, Aliso Viejo, California). The microwire and microcatheter system used were a .16 × 180 cm Fathom (Boston Scientific, Marlborough, Massachusetts) and Excelsior XT 27 (Stryker, Kalamazoo, Michigan) to access the thrombus proximally. Initial suction thrombectomy was performed. A 6 × 25 mm TrevoXP ProVue SR (Stryker, Kalamazoo, Michigan) was then deployed twice under manual aspiration. Figure 3. A repeat angiogram demonstrated a 50% reduction in the burden of renal thrombus. Additionally, there was evidence of a focal dissection for which a 5.5 × 15 mm RX Herculink stent (Abbott, Chicago, Illinois) was placed with successful reconstitution of flow on follow-up angiogram. Figure 4. She was discharged on anticoagulation medication. At 1-month follow-up, the patient denied abdominal pain and labs showed a normalized creatinine. No follow-up imaging was obtained. Angiography demonstrates acute right renal artery thrombosis with decreased distal renal perfusion. Angiography demonstrates use of the stent retriever to entrap the thrombus in the right renal artery. Angiography reconstitution of flow following endovascular thrombectomy and repair of right renal artery dissection using a Herculink stent.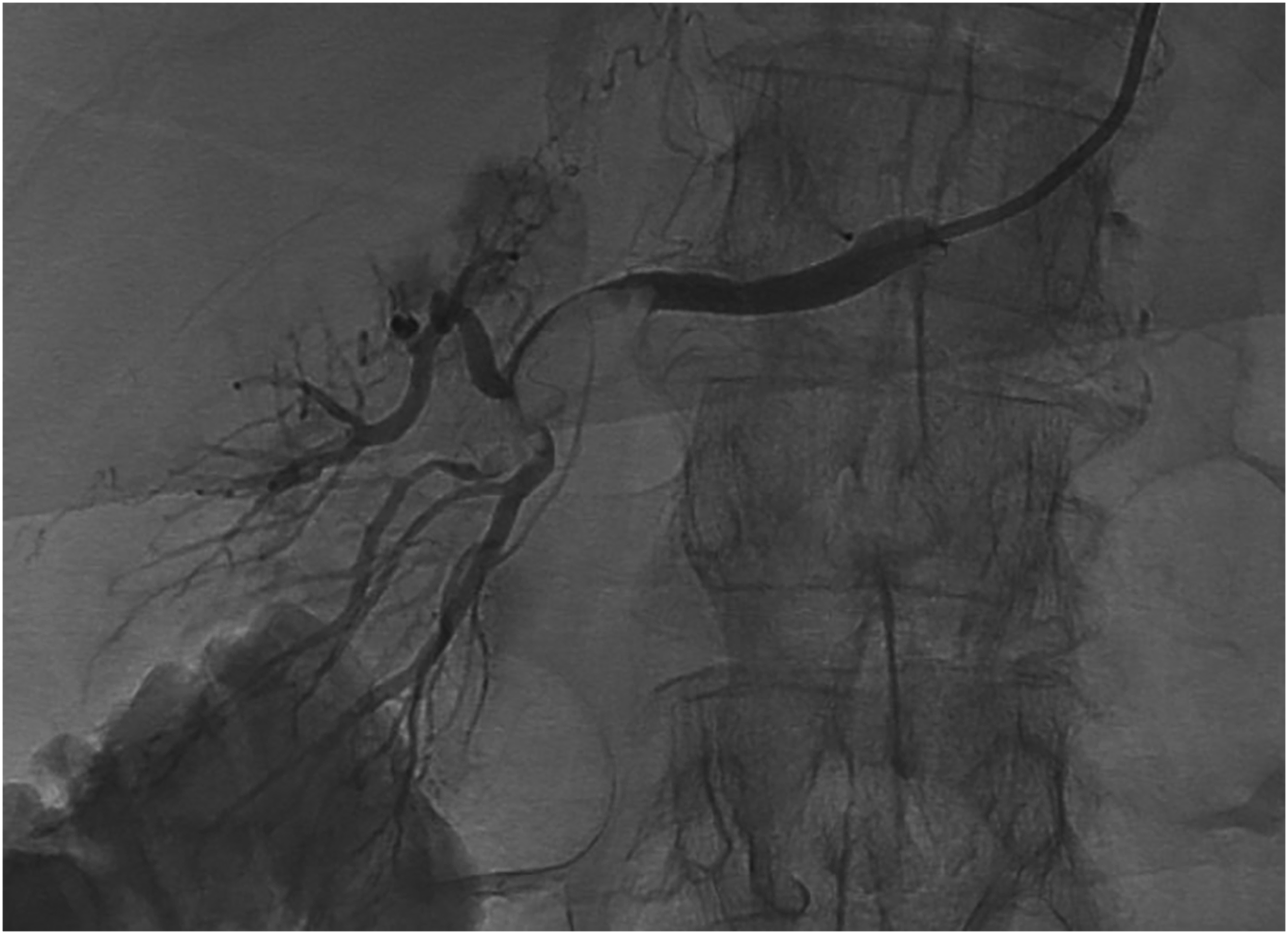

Case Report 2
A 64-year-old man with history of hypertension, hyperlipidemia, and myocardial infarct status post percutaneous coronary intervention (on baby aspirin and Brilinta) presented with acute vomiting and abdominal pain. On presentation, vital signs were unremarkable and creatinine elevated to 1.5 from baseline of 1.2. The patient did not exhibit intestinal ischemia symptoms such as hematochezia or peritonitis. Due to suspicion for chronic mesenteric ischemia, the patient underwent a CT angiogram which demonstrated possible stenosis of the mid-SMA. The patient was taken to the interventional suite approximately 30 hours after diagnosis for diagnostic angiography whereupon the patient developed acute SMA thrombus intraprocedurally.
Vascular access was obtained using the left radial artery with a 5F Glidesheath (Terumo, Somerset, New Jersey). The mesenteric arterial system was catheterized using a 6F JR4 guiding catheter. 50% stenosis was confirmed on intravascular ultrasound. However, diagnostic angiography demonstrated development of acute thrombus in the proximal SMA (1.0 cm from the ostium) as well as embolus in the right colic artery. Figure 5. Initial suction thrombectomy was unsuccessful. Intravascular direct thrombolysis was started using 10 mg of tPA and 7000 units of heparin. EVT was successfully accomplished using an Excelsior XT-27 .027 microcatheter (Stryker, Kalamazoo, Michigan) and a Trevo XP ProVue SR (Stryker, Kalamazoo, Michigan) with multiple passes. Figure 6. 1200 mcg of nitroglycerin were administered throughout the mechanical thrombectomy portion of the case. Balloon angioplasty of the proximal right colic artery at the level of a focal stenotic lesion and acute thrombus was performed using a 2 mm × 20 mm Maverick catheter (Boston Scientific, Marlborough, Massachusetts). Finally, three 7 mm RX Herculink stents (Abbott, Chicago, Illinois) were deployed across the stenotic lesion in the proximal SMA. Post-treatment angiography from the level of the SMA demonstrated no residual thrombus and focal areas of vasospasm in the distal mesenteric arterial tree. Figure 7. At 1-month follow-up, the patient denied any abdominal pain. Creatinine returned to baseline at 2 months post-procedure. No follow-up imaging was obtained. Angiography demonstrates acute mid-superior mesenteric artery thrombosis. Angiography demonstrates use of the stent retriever to entrap thrombus in the superior mesenteric artery. Angiography demonstrating restoration of flow in the superior mesenteric artery following endovascular thrombectomy and stenting.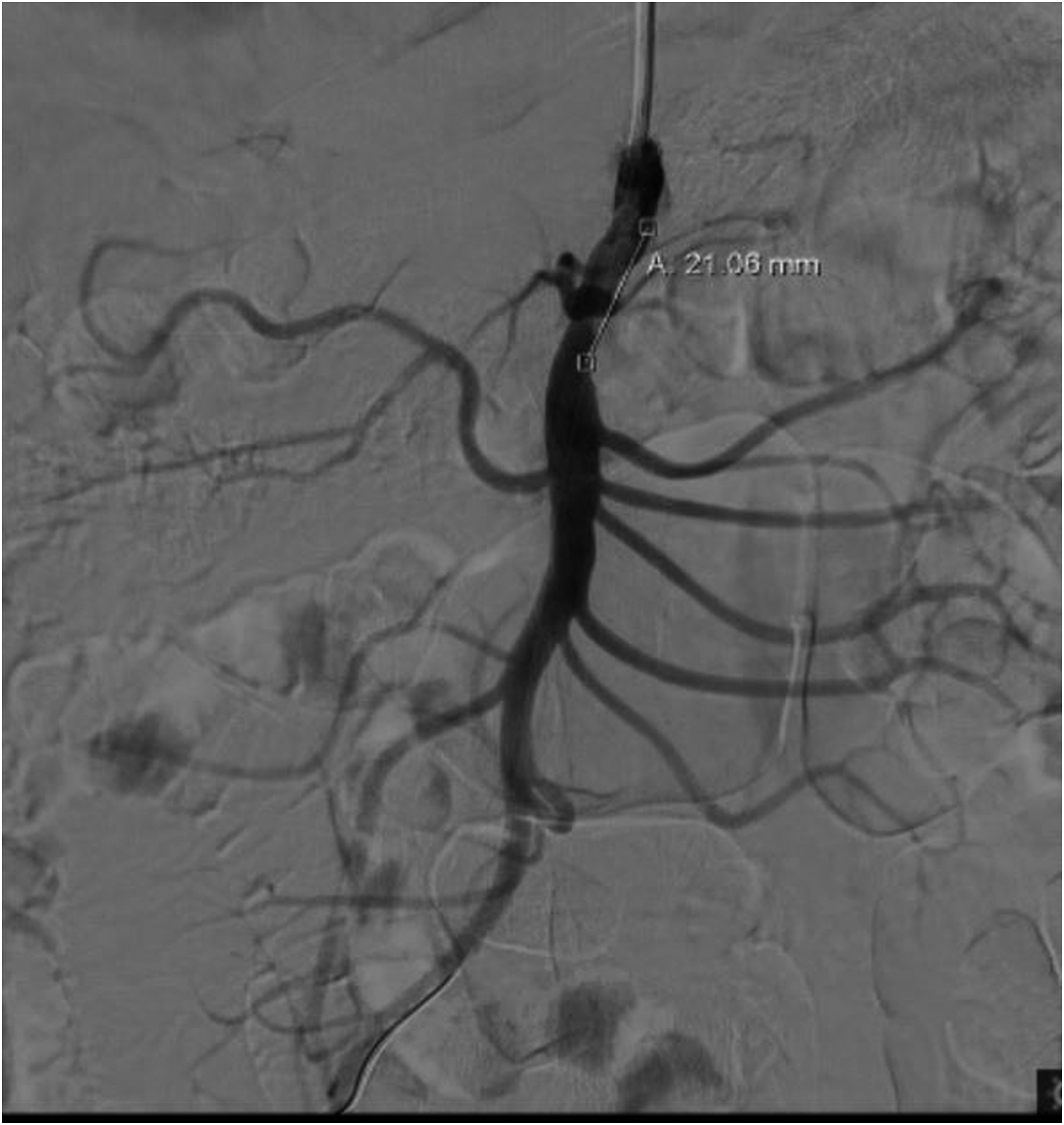


Discussion
The case reports presented suggest that it is practical to consider SRs as potential second-line interventional tools outside of the acute stroke setting, especially when dealing with small vessel therapy in nonsurgical candidates or in patients with high risk of bleeding. The proceduralists in these cases had limited experience with SR as non-neuroradiology interventionalists.
SR History, Technique, and Design
Following validation through several randomized controlled trials, EVT is now the standard of care for acute stroke due to large vessel occlusion with contact aspiration (CA) and SR as the two major EVT methods.7,8 SRs are self-expanding Nitinol wire microstents that deploy into occluding thrombi, enabling clot entrapment between the stent and vessel wall. 9 The technique includes placing a 6–8F guide catheter at target artery, using a 5–6F intermediate catheter to access thrombus proximally, guiding a microcatheter distal to the thrombus, deploying the SR across length of thrombus, and retracting the entrapped thrombus microcatheter system into the intermediate catheter. 7 SR diameters typically range between 4 and 6 mm with lengths from 15 to 30 mm, sizes that are optimized for mechanical thrombectomy within the intracranial internal carotid artery and M1 branch of the middle cerebral artery. The microcatheters usually have .021 to .027-inch inner diameters. 6 Complications of SR use include arterial perforation (.9–4.9%), intracerebral hemorrhage (3.6–9.3%), subarachnoid hemorrhage (.6–4.9%), arterial dissection (.6–3.9%), distal embolization (1–8.6%), vasospasm (3.9–23%), clot fragmentation (rare), and stenosis. 10
Multiple SR designs exist in the market and several experiments have tested the efficacy of thrombus removal based on different device components and techniques. For instance, a constant and greater SR radial force, longer SR length, and larger SR cells allow for better clot engagement and retrieval.9,11 However, with increasing SR device size and radial force, there exists a risk of vascular wall damage secondary to circumferential inflammation of the vessel intima and media following SR application. 12 Furthermore, segmented SR cells can help reduce the rate of SR collapse within tortuous vessels and in turn improve clot retrieval.11,13
Extracranial Use of SR
This brief report describes successful treatment and outcomes for acute arterial thromboembolism of the renal artery and the SMA by using SR devices. Clinical outcomes likely reflect quick revascularization following diagnosis, within 12 hours for the renal artery thrombosis case and immediately intraprocedurally for the SMA thrombosis case. Postprocedurally, it is important to closely monitor labs and vascular imaging, since irreversible ischemia and vascular reperfusion can lead to organ failure with poor prognosis. 14 To date, only one case in literature has described SR application for native renal arterial embolism management in a critically ill patient, using local anticoagulation, aspiration, and SR. 6 A cohort of 9 cases reported SR/CA/stent use for management of SMAthrombosis. 15 SR can ultimately serve as a backup option for acute intra-abdominal thrombectomy procedure when other forms of thrombolysis or thrombectomy fail, especially for smaller caliber vessels such as the renal and mesenteric arteries. Advantages of SR include removing the occluding clot intact, thus reducing the risk of distal embolization. Use of a balloon guide catheter to achieve flow arrest also reduces the risk of distal embolization. 8 Advantages specific to the Trevo XP include circumferential large cells, a soft tapered flexible distal tip for improved distal placement, full length radiopacity, and hydrophilic coating. 16 Drawbacks for using these SRs include small caliber size as well as device use comfort level for practitioners who do not often use this device. In patients with tortuous vessels, extensive calcified atherosclerosis, or long segment occlusion, EVT may not be feasible. 5
There have been other case reports and case series detailing the extracranial use of SRs in the literature. For example, extracranial application of SR includes a case series of 3 high-risk patients who failed conservative medical management for carotid artery thrombosis and who underwent successful recanalization using a combination of SR, aspiration, and distal emboshield filter. 17 Three cases involving acute coronary artery occlusion, one of which failed aspiration EVT and endovascular thrombolytics, used a combination of SR, angioplasty, and stenting.18-20 In a cohort of five infants with superior vena cava/brachiocephalic venous thrombosis following line placements, a combination of SR, aspiration, systemic thrombolysis, and angioplasty was successfully implemented without associated complications. 21 Additionally, a nonsurgical post-transplant patient who had acute hepatic artery thrombosis was successfully treated with SR, aspiration, and stenting. 22 SR was also applied in a patient with popliteal artery thrombosis after not responding to local thrombolysis and aspiration. 23 Finally, one case reported the used SR, aspiration, stenting, and local thrombolytics to treat an occluded renal artery chimney stent graft. 24
As suggested by the successful results of the cases presented above, use of SRs as an alternative thrombectomy device in the extracranial setting should be considered when traditional treatment methods fail.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
IRB Approval: These case reports do not meet the DHHS or FDA definition for human research; therefore, it is exempt from IRB review at the home institution. Informed consent has been obtained from the patient for publication of the case report and accompanying images.