
Abstract
Keywords
Introduction
Visceral arteries include the celiac axis and its branches, superior and inferior mesenteric arteries and the renal arteries. Reconstruction of these arteries is performed when they are significantly diseased causing end-organ symptoms. Reconstruction include endovascular procedures such as angioplasties with or without stent, surgical procedures, namely, thrombectomy or embolectomy in acute cases, endarterectomy with or without patch closure, bypass using synthetic conduits or vein graft, segmental reconstruction and re-implantation of the diseased artery. Historically, open bypass procedures have been preferred to endovascular procedures using various techniques. 1 The topic of interest in this review is the use of autologous vein graft (AVG) and synthetic graft (SG) in visceral arterial reconstruction (VAR) and their outcomes.
Among the vein grafts, autologous reversed saphenous vein graft is the commonest used conduit for arterial bypass. Synthetic grafts such as dacron, polytetrafluoroethylene, polyester and polyurethane grafts and homografts such as the Dardik umbilical vein graft or cryopreserved arterial graft have all been used in arterial bypass surgery. The hypogastric artery is also used occasionally. There are advantages and disadvantages with the use of AVG and SG. 2 Graft infection and stenosis secondary to intimal hyperplasia are the main concerns with SG. 2 Most authors report using SG except in patients with high risk of infection. Vein grafts have a propensity to dilate over time.3-5 There are reports of its occurrence in aorto-coronary grafts. However, the exact incidence is not clear with a wide range of incidence rates being reported.3,5 Neitzel et al. 3 have reported an incidence of 14%, and Dieteret et al. 5 have reported an incidence of 0.07%. Similar concerns have been expressed with visceral arterial bypass originating from the aorta to the target visceral vessel. Controversy in this aspect exists with no documented cumulative evidence available supporting the use of either conduit in VAR. Hence, a systematic review was undertaken to study the individual outcomes of AVG and SG in VAR originating from the aorta.
Methods
The methodology of the current review was according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 6 The study is registered with Centre for Reviews and Dissemination, University of York, PROSPERO 2017: CRD42017083572.
Inclusion and Exclusion Criteria
All studies in which patients undergoing visceral arterial bypass procedure utilizing AVG or SG as a primary intervention in chronic visceral ischaemia were included irrespective of study design. Studies were excluded if data of acute mesenteric ischaemia and chronic mesenteric ischaemia or autologous and SG could not be separated. We also excluded studies in which data of bypass procedures could not be separated from interventions such as angioplasty or stenting, endarterectomies with or without patch and re-implantation, re-interventions and combined aortic aneurysm repair with visceral artery reconstruction. Studies which included patients with Takayasu’s arteritis were also excluded so that outcomes due to the disease process will not affect the graft outcome. Non-English language articles when English translation was not available, case series of less than 10 cases and case reports were also excluded.
Outcome Measures
Outcome measures included primary patency, secondary patency, complications such as graft thrombosis, dilatation, infection, aneurysm (true and false/pseudo), anastomotic stenosis and all-cause mortality (30 day, 1 year and 5 years).
Search Methods for Identification of Studies
The electronic databases searched to identify potential studies were Ovid-Embase and PubMed Medline. No limits or filters were applied to any of the databases. The keywords used for the search were ‘Mesenteric vascular disease’, ‘acute mesenteric ischaemia’, ‘mesenteric artery, superior’, ‘mesenteric artery, inferior’, ‘celiac artery’, ‘renal artery’, ‘saphenous vein’ and ‘vein’. A detailed search strategy is included in Supplementary Materials 1. The reference lists of relevant articles were also checked to search for potential studies for inclusion.
Selection of Studies
With the specified search strategy, each database was explored by 2 authors (GG and RD) independently. The search results were merged to remove duplication. Title screening was done for all the articles obtained through initial hit. Articles were rejected on initial screen when the review authors determined from the title that they were not relevant. All titles of the relevant studies meeting the criteria to be included were screened for abstracts. If the abstract screen was found not of relevance to VAR, it was excluded. When a title or abstract screen was inconclusive to include or reject, full text was examined. Two review authors (GG and RD) independently assessed the studies for inclusion and resolved differences between their assessments by discussion and in consultation with a third review author (PD). In the case of duplicate publications and companion articles of a primary study, all available data were obtained for complete information. When multiple reports of the same study existed, the studies were linked together. A decision on which study should be included was based on the inclusion criteria. Figure 1 (PRISMA flow diagram) illustrates the selection process of studies included in the review where n represents the number of records. Preferred reporting items for systematic reviews and meta-analyses flow diagram.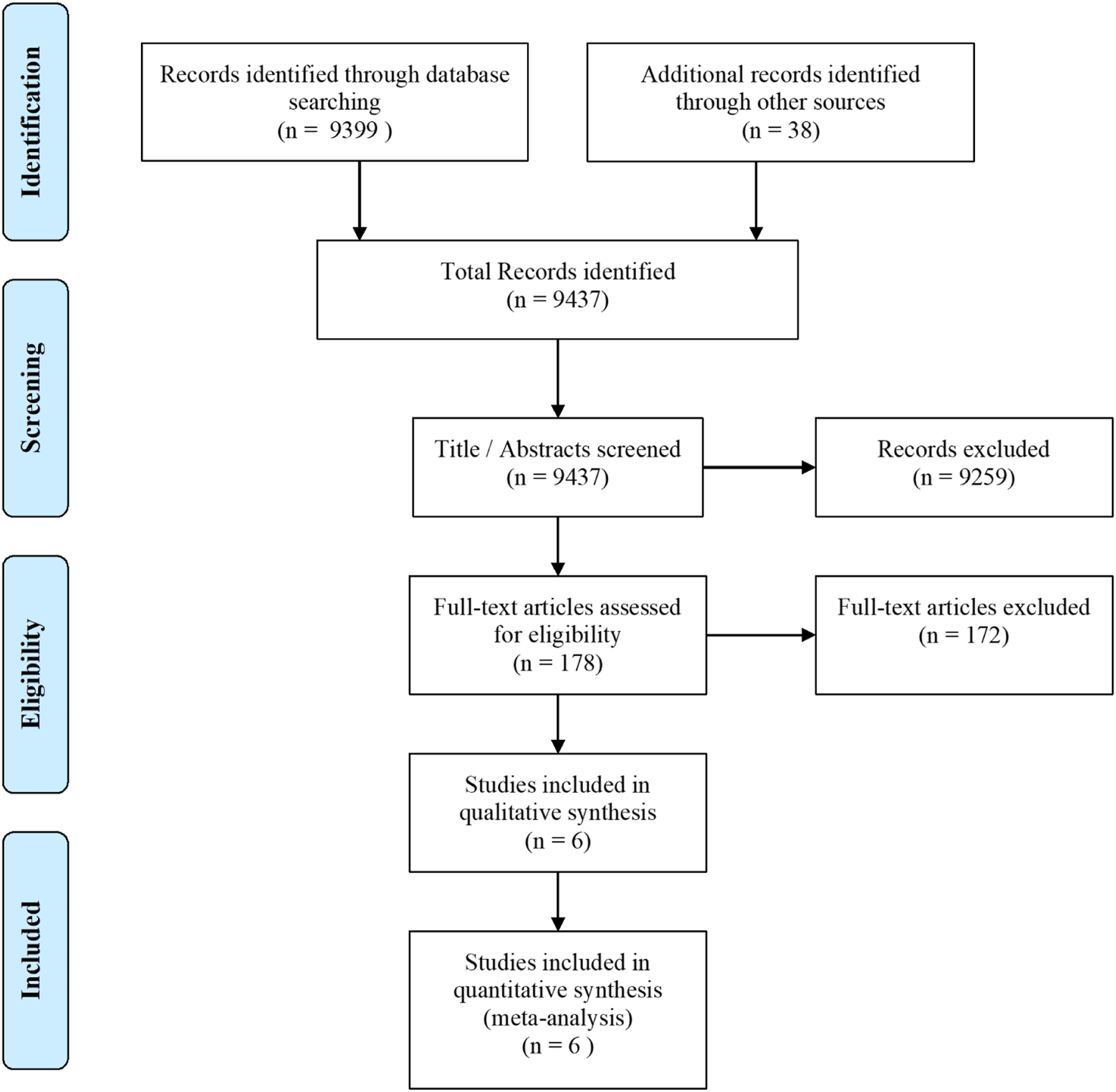
Data Extraction and Management
The data extraction form was constructed based on the review objectives. Two review authors (GG and RD) independently extracted data from included publications on to an Excel spreadsheet. Items under which data were extracted included – authors, institution, country, period of study, type of study, methods of patient selection, inclusion, exclusion, age (average, mean and range), gender, number of patients, statistical analysis, aetiology, comorbidities, type of interventions, number of vessels reconstructed, graft type, follow-up period, morbidity and mortality, patency rates, graft-related complications, conflict of interest and ethical approval. Efforts were taken to minimize bias by extracting data independently using piloted data extraction tool.
Assessment of Methodological Quality of Included Studies
All studies included were case series, and we used Joanna Briggs Institute critical appraisal checklist for case series. 7 The tool consists of 10 items and we have excluded studies that did not indicate a consecutive and complete inclusion of participants. Hence, 6 studies were included for the final analysis.
Data Analysis
Data were extracted for all the outcomes, and pooled proportion was estimated using the random effects model wherever appropriate. We reported pooled proportions with 95% confidence intervals (CIs), heterogeneity index (Q), degrees of freedom (df) and I2 statistic. We used ‘metaprop’ command for meta-analysis and confidence intervals were computed using score method. 8 Proportions are presented in a forest plot; however, all the results are displayed in percentages for ease of understanding. All the outcomes except mortality were analysed with the denominator being number of reconstructed vessels.
Results
Study Characteristics
Characteristics of Included Studies.
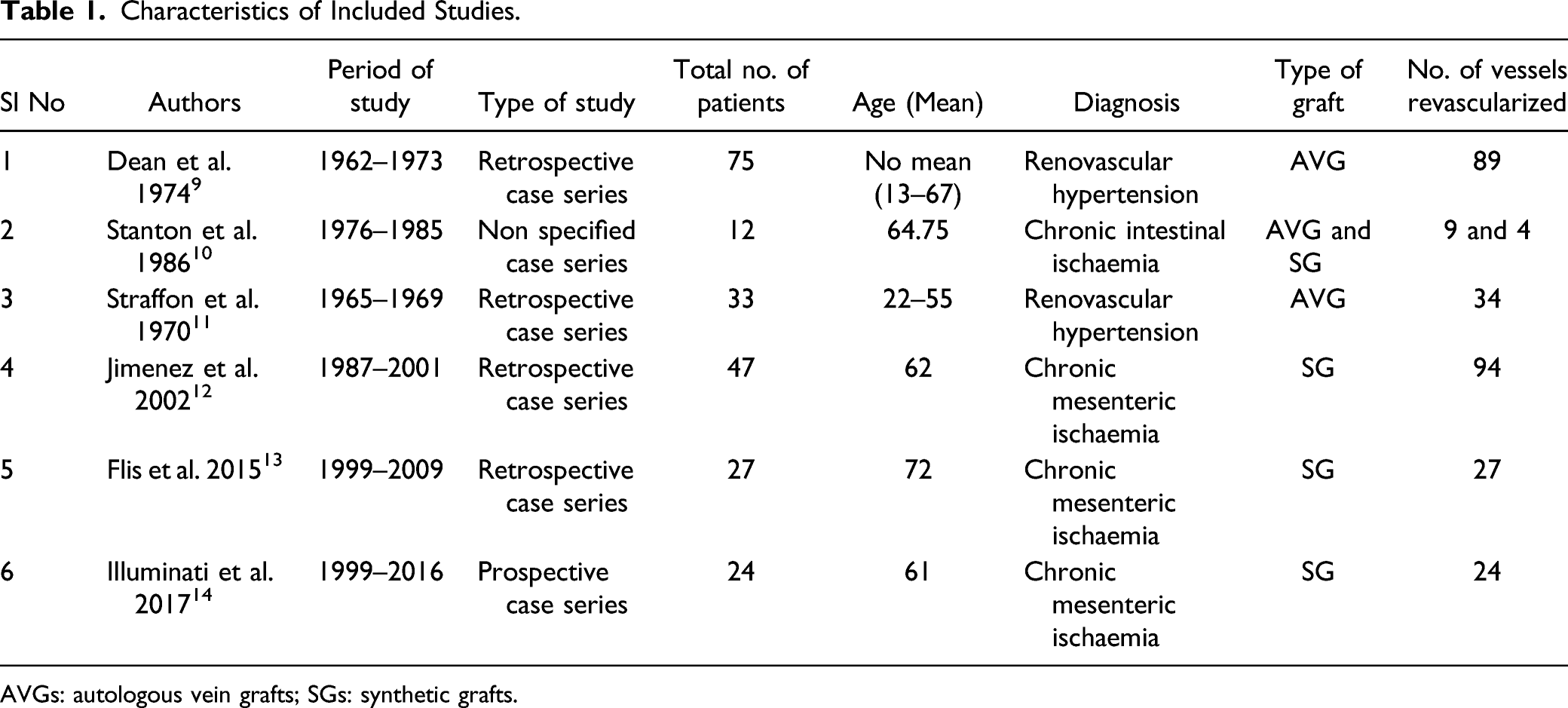
AVGs: autologous vein grafts; SGs: synthetic grafts.
Studies Reporting Outcomes for Vein Grafts
There were 3 studies, 2 mesenteric artery10,11 and 1 renal artery
9
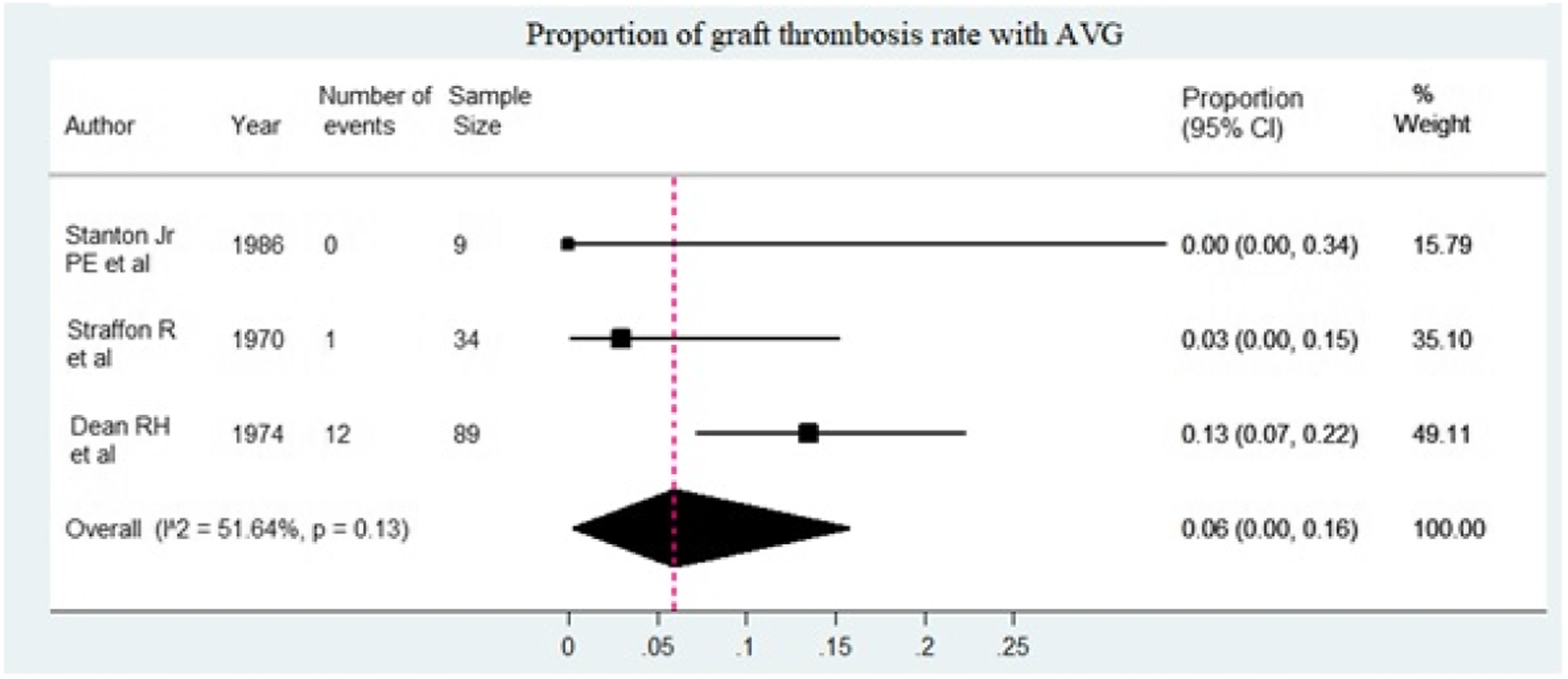
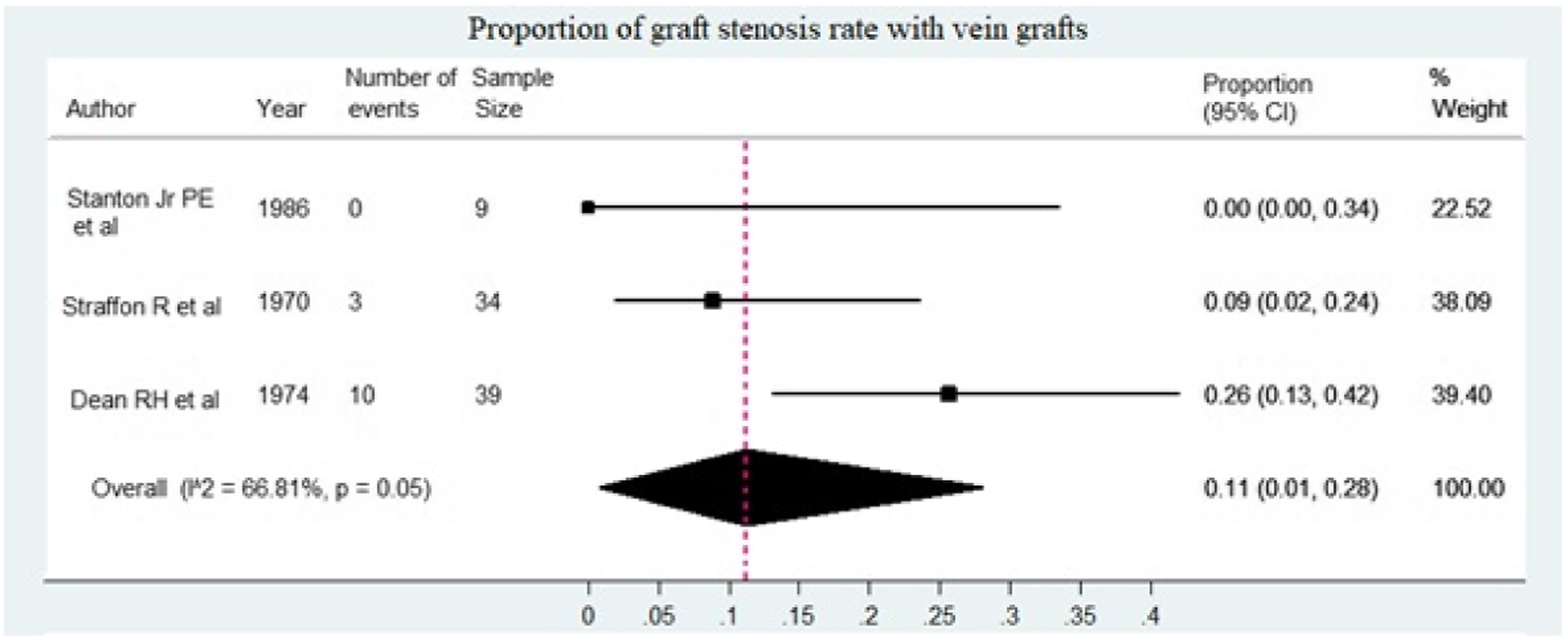
revascularization, in which vein grafts were used (117 patients and 132 vessels revascularized). Pooled primary patency rate at 1 year (n = 132) in the 3 studies was 87% (95% CI 71%, 97%) (Figure 2). Overall graft thrombosis rate (Figure 3) in the 3 studies (n = 132) was 6% (95% CI 0%, 16%) (Figure 3). Dean et al.
9
reported vein graft dilatation in 20.5% (17 to 47% dilatation in 8/39 bypass grafts 2 to 6 years after bypass and true aneurysmal dilatation of 87%−106% in 2 bypass grafts at 3 and 6 years in a subgroup of 29 patients. None of these dilatations or aneurysms progressed on further surveillance and did not need any intervention. Pooled stenosis rate at 1 year was 11% (95% CI 1%, 28%) (Figure 4). There were no deaths reported in the first 30 days after surgery in the Stanton et al.
10
and Straffon et al.
11
series and 3.2% in the Dean et al.
9
series amounting to a pooled 30-day mortality of 1% (95% CI 0%, 4%). Stanton et al.
10
and Straffon et al.
11
continued this trend at 1 year, having no mortalities. Stanton et al.
10
reported a mortality of 25% (2/8) at 5 years, all due to myocardial infarction (Table 2). There was no data on infection and pseudoaneurysm in any of the studies. One-year primary patency with autologous vein grafts. Graft thrombosis rate with autologous vein grafts. Graft stenosis rate with vein grafts. Mortality With Vein Grafts in Visceral Arterial Reconstruction.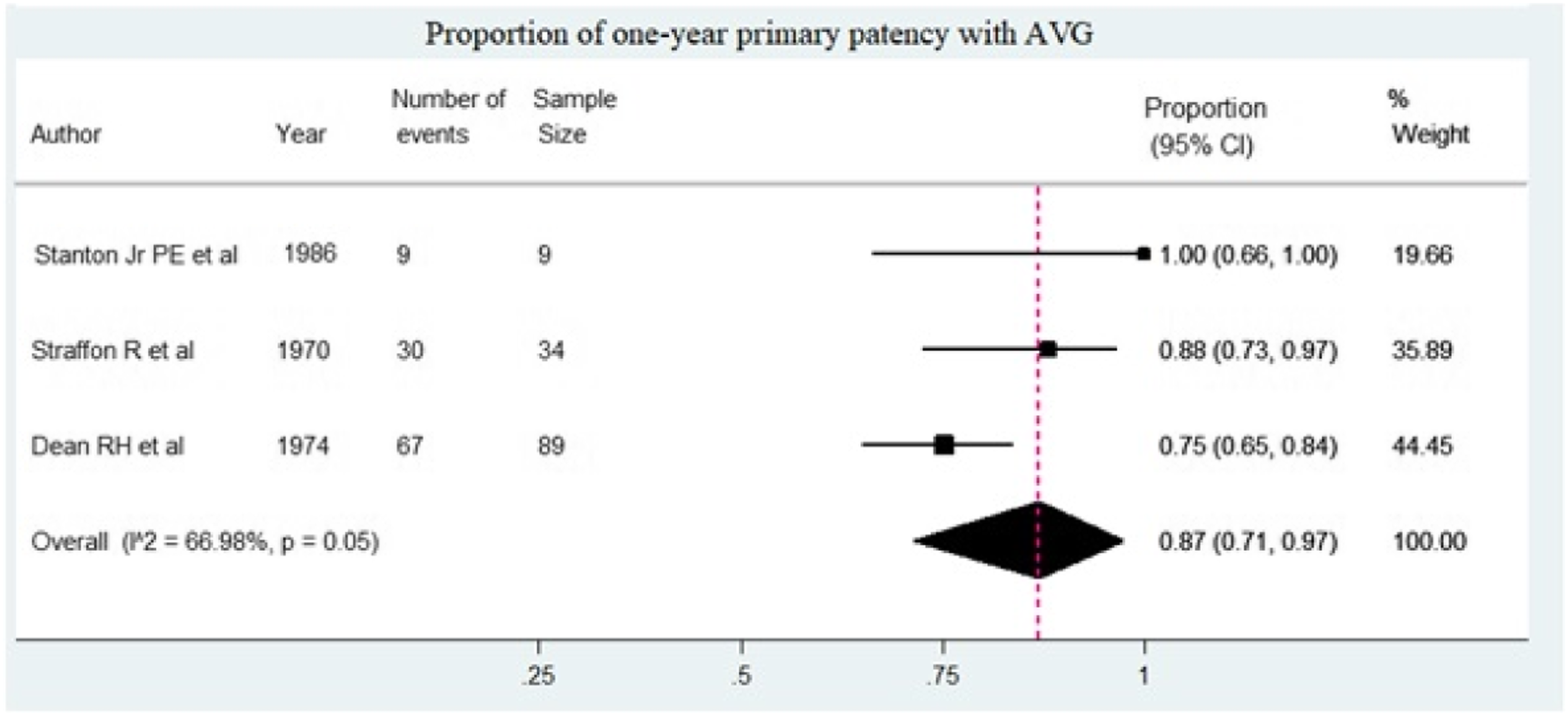

Studies Reporting Outcomes of Synthetic Grafts
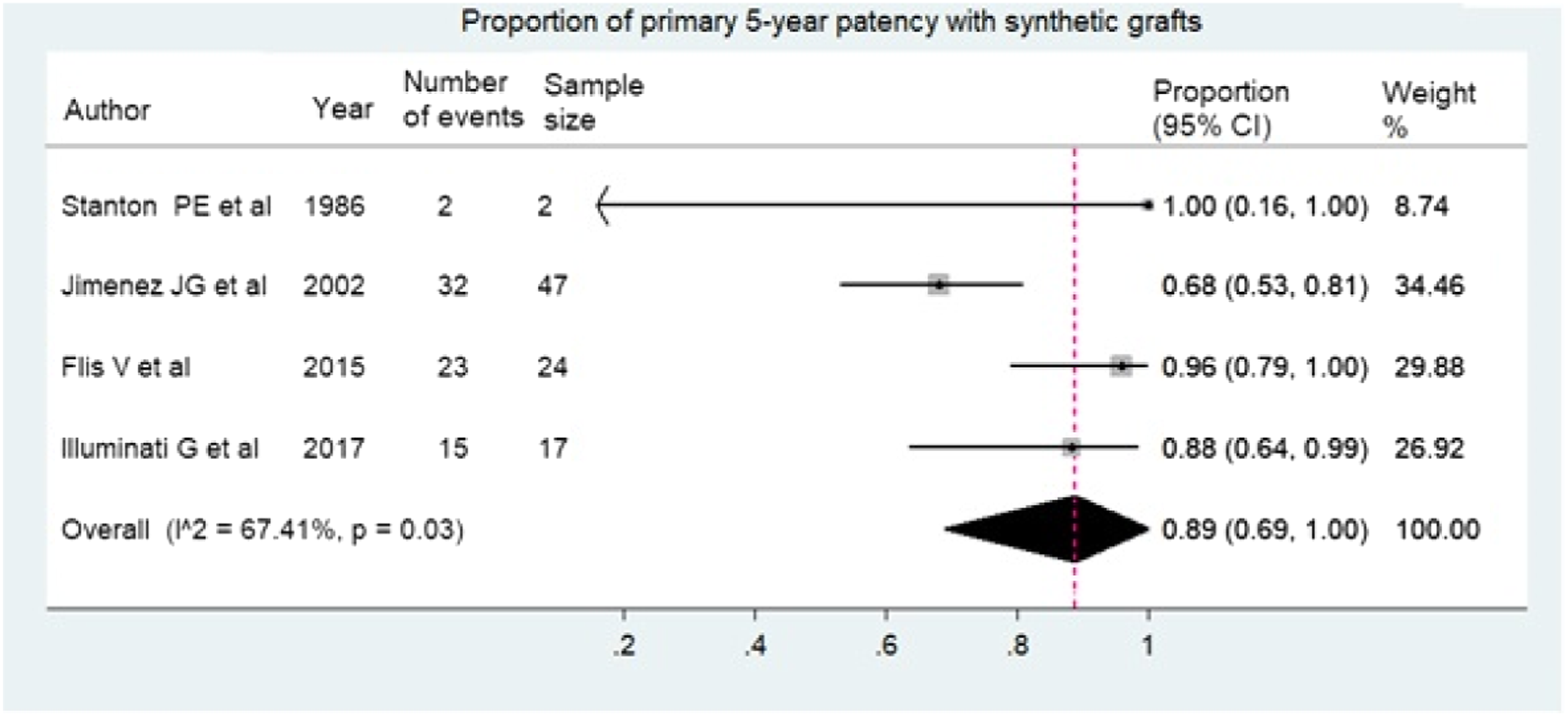
Four studies10,12-14 reported individual outcomes for SG (106 patients and 147 vessels revascularized) with a pooled primary patency at 1 year (Figure 5) of 100% (95% CI 99%, 100%). Pooled primary 5-year patency rate was 88% (95% CI 69%, 100%) (Figure 6). Jimenez et al.
12
reported 100% secondary patency in 7 out of 47 patients followed up at 5 years. Flis et al.
13
and Illuminati et al.
14
reported to have had no graft infection in their series. Overall pooled percentage of graft thrombosis and stenosis at 1 year was 0%. Of the 4 studies, Jiminez et al.
12
had 1 graft thrombosis at 20 months and 2 graft stenoses at 46 and 49 months. Illuminati et al.
14
reported graft thrombosis/occlusion in 2/24 patients at 22 and 52 months post revascularization. Jimenez et al.
12
reported a 0% incidence of true aneurysms in their series of 94 grafts. Overall pooled 30-day and 1-year mortality was 1% (95% CI 0%, 6%) and 7% (95% CI 0%, 20%), respectively (Table 3). The five-year mortality was 39% (95% CI 11%, 72%). There was no mention of graft dilatation or pseudoaneurysms in any of the 4 studies and so their occurrence or non-occurrence was not clear from the data. (Figure 5). Pooled primary patency rate at 1 year with synthetic grafts. Pooled primary 5-year patency with synthetic grafts. Mortality in Synthetic Grafts in Visceral Arterial Reconstruction. SG: synthetic graft.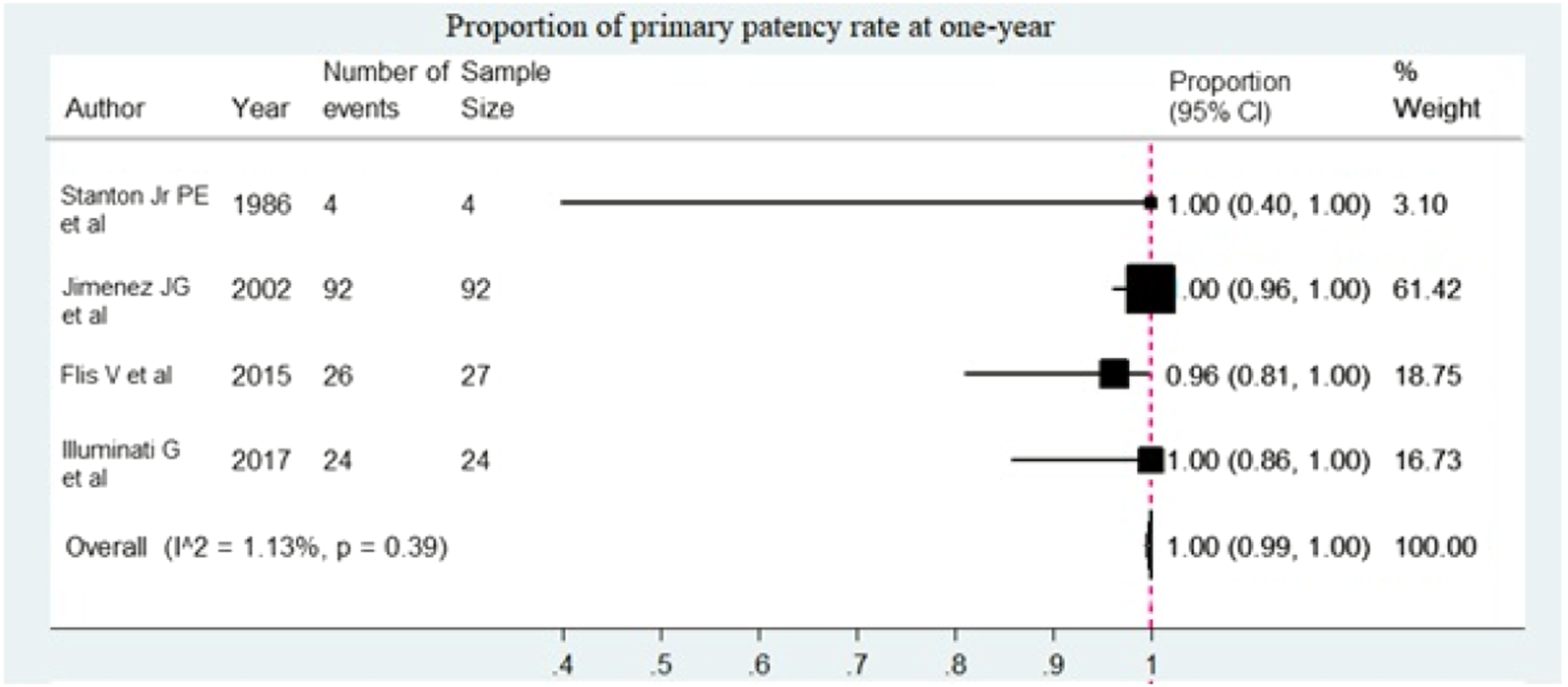

Discussion
In studies that had separate data for synthetic and autologous vein grafts, primary patency at 1 year seemed to be better with SGs compared to vein grafts, 100% vs 87%. The Stanton et al. 10 series was the only one which compared vein (n = 9) and SGs (n = 4), with a 100% patency at 1 year in both groups. Being a small case series, these results should be interpreted accordingly. Graft thrombosis and anastomotic stenosis were higher with vein grafts compared to SGs (6% vs 0% and 11% vs 0%, respectively). One would expect better outcomes with vein grafts if the outcomes reported with peripheral bypass procedures were to be compared. The lower patency rates with vein graft are noticeable within the first year of the procedure, suggesting a mechanical cause for the failing graft. The mesenteric bypass being a short bypass involving medium sized arteries, may not be comparable to the lower limb bypass procedures, possibly accounting for the better outcome with SG in the former. The stability offered by the SG placed in the abdomen compared to vein grafts, the latter being subject to acute angulation with changing positions of the abdominal viscera may be another factor for the better outcomes with SGs. Experimental studies have also suggested better outcomes of vein grafts when they are externally supported by either a stent or a tightly woven sheath of SG by preventing intermittent dilatation, lengthening of the graft, angulation and helical distortion 15 and prevent the development of intimal hyperplasia. 16 In renal artery revascularization, the right-sided bypasses had a tendency for late mid-graft stenosis in the vein grafts, which is attributed to the retrocaval routing of the graft 9 . There may be a case for anterior routing of the vein grafts to prevent this occurrence.
In the studies that included vein grafts,9-11 the 30-day mortality was 1% (Table 2) in a total of 125 patients. One-year mortality was reported only in 2 studies10,11 and was 0%. In the SG group, 30-day and 1-year mortality rate was 1% and 7%, respectively (Table 3). 5-year mortality reported by 2 authors in the vein graft group10,11 (n = 41) and 4 in the SG group10,12-14 (n = 61) was 1% and 39%, respectively. The mortality data should have included a uniform method of reporting cause of death as well as predictive preoperative morbidity and morbidity scores for correlation. Visceral artery disease-specific mortality was not extractable from any of the studies. There has been a high dropout rate from follow-up, which makes the interpretation erroneous.
The other complications, namely, graft infection, graft dilatation and aneurysmal dilatation were not reported in most studies. It is likely that these complications did not happen, but it is difficult to assume that it is the case as they have not been explicitly documented and hence not further analysed. Flis 13 specifically mentioned that they did not have any graft infection in their SG series. Graft dilatation, which is a concern with many experts in the field when vein graft is used, was reported by Feng et al. 17 (not included in this review) with an incidence of 5.13% (mild dilatation noted in 2 bypass grafts at 2 and 3 years) and by Dean et al. 9 with an incidence of 20.5% (17 to 47% dilatation noted at 2-6 years after bypass in 8 out of 39 grafts). Most of these were not true aneurysmal dilatations. Even when there was true aneurysmal dilatation of 87–106%, in the 2 patients in the Dean et al. 9 series, no intervention was deemed necessary as none of them progressed any further at later surveillance. However, with modern day surveillance and availability of endovascular treatment options, stenting the aneurysmal grafts would be an option. Although paediatric patients were not included in this review, it is highly likely that vein graft dilatation may be more of an issue in this group of patients in the long run. With the current availability of imaging facilities, a focused follow-up of these patients would give us useful information. There was a report of a nine-year-old boy who had an external iliac vein as a conduit for superior mesenteric artery bypass and ilio-hypogastric artery for renal artery bypass 18 in whom the hypogastric artery conduit underwent a 100% dilatation, and the saphenous vein graft underwent a 300% dilatation within 3 years.
Conclusions
Our analysis of the available data points towards better patency rates with SG compared to vein grafts, but more robust studies in terms of study design, data collection and analysis and long-term follow-up are required to emphatically state this conclusion. Mortality seemed to be higher in the SGs, but in the absence of prognostic and morbidity indices, we would not draw firm conclusions. Graft dilatation does occur with vein grafts. However, it seems from this review that intervention is not required as the dilatation does not progress indefinitely. With the present day imaging techniques and the ease of their availability, monitoring their progress is rather easy. In addition, interventional options are now advanced, and these dilated grafts can be easily treated with endovascular stents. Reporting standards for these studies need to be standardised for homogeneous data and a better understanding of the outcomes.
How This Review Will Affect Clinical Practice
With limited information available in the present literature, we cannot recommend on the type of graft to be used. However, it looks like the SG has better patency compared to vein grafts. We would continue to select the type of graft depending on the clinical condition of the patient, mainly the presence or absence of bowel necrosis. Graft dilatation is an issue that needs to be considered when vein graft is used in these patients. It is probably more common in the paediatric population where the graft has to remain in situ for longer periods and is subject to the growth of the child with changing haemodynamics.
Limitations and Strengths of the Review
The reporting standards of the outcomes included was haphazard as we could not extract data for vein and SG separately in many studies and hence were either excluded or the data limited to what was available. Studies with combined aortic aneurysm repair and mesenteric revascularization were excluded as the mortality with aneurysm would have skewed the outcomes. Some authors mentioned outcomes in their discussion and some in the results and some others only in their tables or abstracts. When studies had both vein grafts and SG in their series, we had to manually separate out the data where possible. There was a high rate of dropout of patients in the follow-up, making long-term results unreliable. We recommend uniform reporting of outcomes for these procedures in future publications. We have suggested a reporting protocol in the Supplementary Materials 2, which could be considered to create uniformity in reporting.
Future Research Recommendations
Focused prospective studies comparing SGs and AVGs with clearly separable and standardized outcome reporting at fixed intervals would shed more light on the concerns related to this topic. Paediatric patients undergoing VAR would be an interesting cohort to follow-up for graft dilatation and long-term outcomes specifically related to growth.
Recommendations for Future Practice and Policy
We have compiled a reporting protocol related to visceral artery reconstruction which is appended as Supplementary Materials 2.
Supplemental Material
sj-pdf-1-ves-10.1177_15385744211029112 – Supplemental Material for Outcomes of Visceral Arterial Reconstruction: A Systematic Review
Supplemental Material, sj-pdf-1-ves-10.1177_15385744211029112 for Outcomes of Visceral Arterial Reconstruction: A Systematic Review by Rovan Evan D’Souza, Girish Girish, Preethy D’Souza, Melissa Glenda Lewis and Vishnu Renjith in Vascular and Endovascular Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.