
Abstract
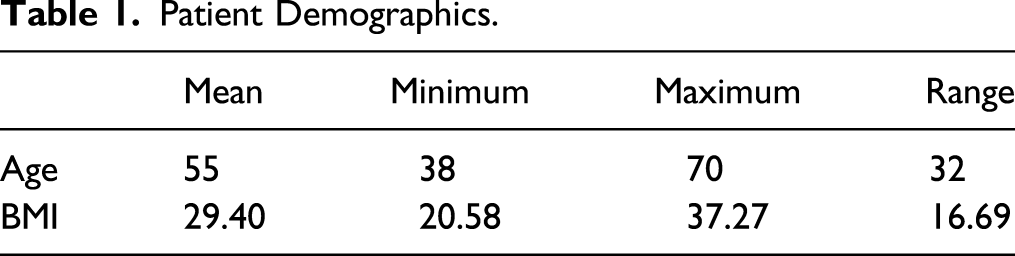
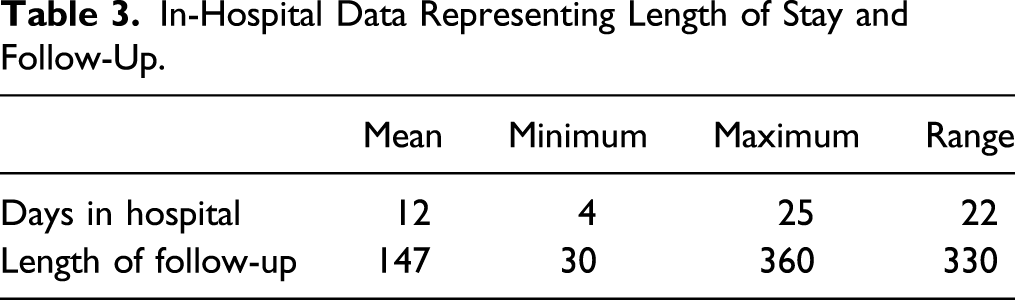
Introduction: Descending aortic complex atheromatous plaques can cause claudication, critical lower limb ischaemia (CLI), and are an independent risk factor for systemic embolization. Current practice involves dealing with most cases using endovascular techniques. However, open repair remains superior in terms of the patency rates and may be the only valid option in a subgroup of patients who are unsuitable for endovascular treatments. Most of the current data investigating open procedures are now historic. The aim of this study is to determine whether it is a feasible option in the current day practice. Patients and methods: Ten years data from 2010 to 2020 were collected retrospectively from the hospital records. Clinic letters, radiologic scans, operative records and discharge letters were reviewed. Death records were reviewed to identify patients who survived. Results: Ten cases were identified. The average age was 55 and the mean BMI was 29.4. The mean hospital stay in days was 12 (range: 4 to 22). The mean follow-up period was 147 days (range: 30 to 360 days). Four of the patients were TASC B, four were TASC C and two were TASC D. Two cases had to return to theatres. One patient had transient post-op AF and another had transient post-op ileus. One patient was readmitted within 30 days of discharge for urosepsis. All cases are alive to date except one case which only survived three years after procedure. Conclusion: AE is a procedure that should be considered in selected cases where endovascular approach is not feasible. There is a trend towards lower mortality than the historic data available in literature. Larger case series or registry data may be required to accurately estimate the current day mortality and morbidity figures.
What This Article Adds
Open revascularization through aortic endarterectomy (AE) for a selected group of patients with aortic occlusive disease (AOD) is a well-known operation. However, most of reported data in literature are historic now. With the current day advancement of surgical, anaesthetic and nursing care together with the more specialization, these old studies may not be able to reflect the current day practice in today’s world. This article will reflect the current day practice based on data from a UK high volume tertiary vascular centre experience in the last 10 years.
Introduction
Descending aortic complex atheromatous plaques are prevalent in the population aged 65 years and older with a prevalence rate approaching 12%. 1 In addition to causing claudication and critical lower limb ischaemia (CLI), the aortic plaques are an independent risk factor for systemic embolization 2 and can cause occlusions resulting in acute on chronic peripheral limb ischaemia.
The severity and thus the need for treatment is variable. It can be classified into five grades: grade I (no intimal thickening), grade II (intimal thickening 1–3.9 mm without atheroma), grade III (atheroma <4 mm), grade IV (intimal thickening or atheroma >4 mm) and grade V (any mobile or ulcerated atheroma). 2
Endovascular treatments (ETs) by angioplasty and stenting are now the mainstream treatment overtaking the open repair. The available data are largely based on studies that were conducted more than 20 years ago. These studies found less mortality and morbidity with endovascular treatments which lead to an almost universal approach of endovascular treatment first. However, the open surgery remains the more superior treatment modality in respect to the durability and the patency rates. Even with the advancement in the endovascular techniques and the development of new techniques such as Covered Endovascular Reconstruction of Aortic Bifurcation (CERAB), kissing stents and sub-intimal techniques, primary patency rates remain below those of the open surgery and sometimes requiring re-interventions to achieve secondary patency. 3 Moreover, some of the more complex cases with extensive disease that may not be amenable for endovascular interventions leaving the open approach as the only possible option.
With the current day advancement of surgical, anaesthetic and nursing care together with the specialization, these studies may not be able to reflect the current day practice. The aim of the study is to assess the feasibility of aortic endarterectomy (AE) by reporting on a UK high volume, tertiary vascular centre and its experience in the last 10 years.
Patients and Methods
Ten years data from 2010 to 2020 were collected retrospectively from the hospital records. Ten cases were identified from the hospital database of aortic operations. Clinic letters, radiologic scans, operative records and discharge letters were reviewed. Death records were reviewed to identify patients who survived.
Inclusions criteria included patients who had aortic, aorto-biliac or bi-iliac occlusive disease and undergone elective or emergency AE. All the patients were discussed in vascular MDT and had pre-operative fitness testing in the form of myocardial perfusion imaging test (MIBI) and pulmonary function testing and were deemed fit for open surgery.
Standard aortic endarterectomy extending down to the iliacs was performed through midline laparotomy. A tailored bovine batch cut to measurements was used in each case. The procedure was performed by two consultant surgeons and an anaesthetic team including a specialized consultant vascular anaesthetist.
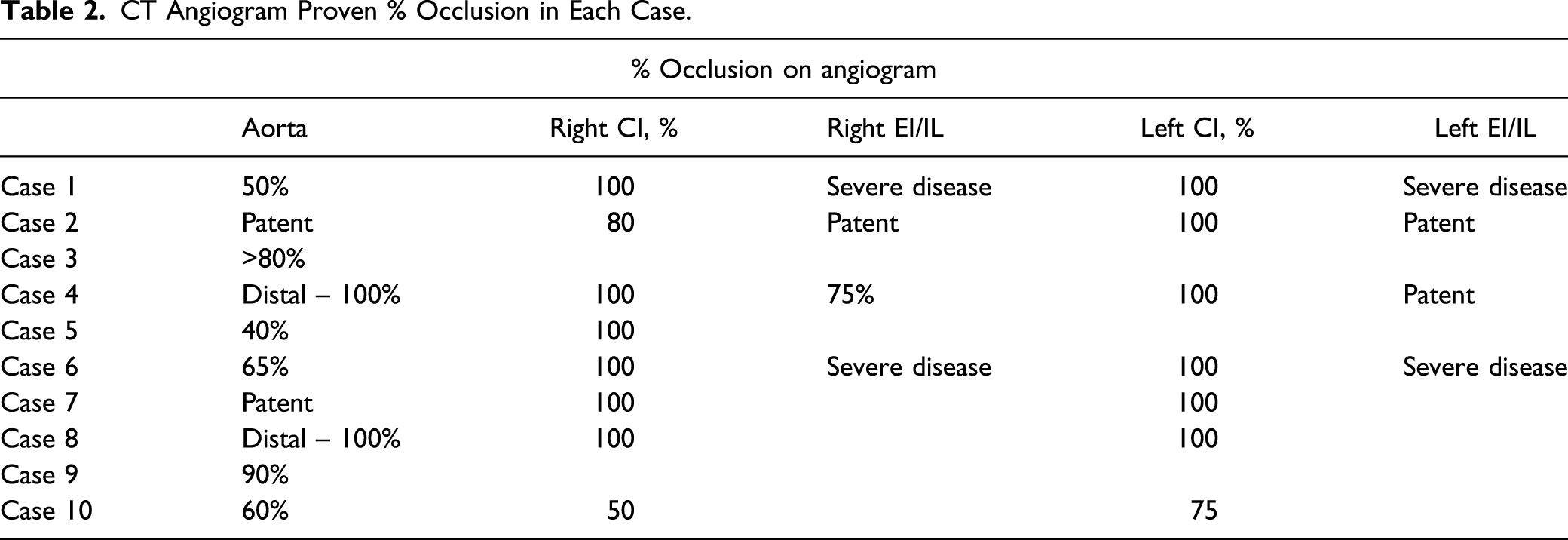
Pre-operative CT scans were looked at and the degrees of occlusion and TASC classifications were identified by two independent operators: a consultant vascular radiologist and a vascular surgeon separately.
The project was approved by the hospital audit department. A formal ethics approval was not required as the project only included retrospective data collection.
Results
Patient Demographics.
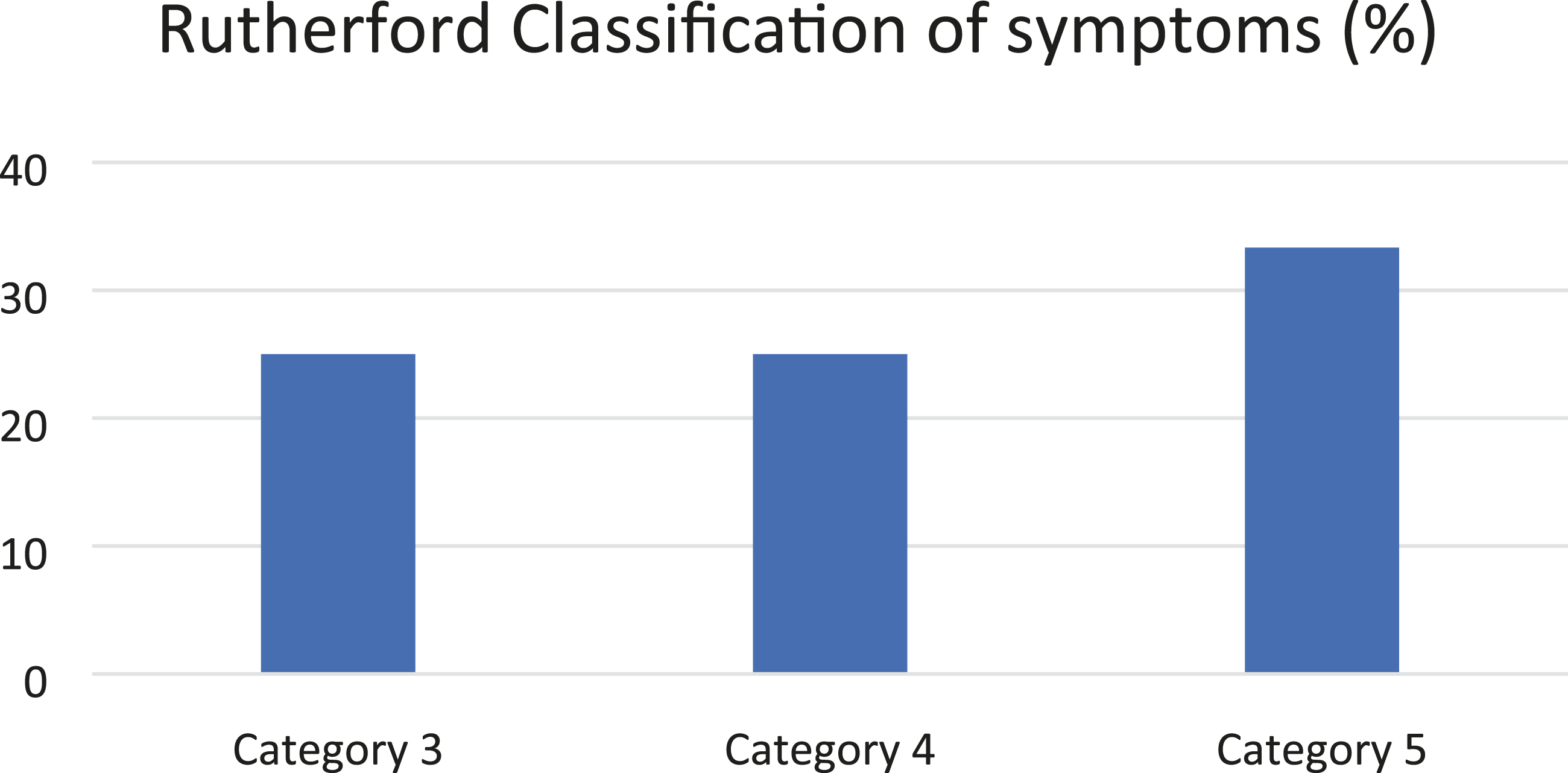
Rutherford classification of the patients’ symptoms by percentage.
The patients had a number of different comorbidities; main ones included hypertension, type 2 diabetes mellitus, ischaemic heart disease and hypercholesterolaemia. Five of the patients were hypertensive, four had ischaemic heart disease (IHD) and four were known diabetics. This is highlighted in Figure 2. Number of comorbidites.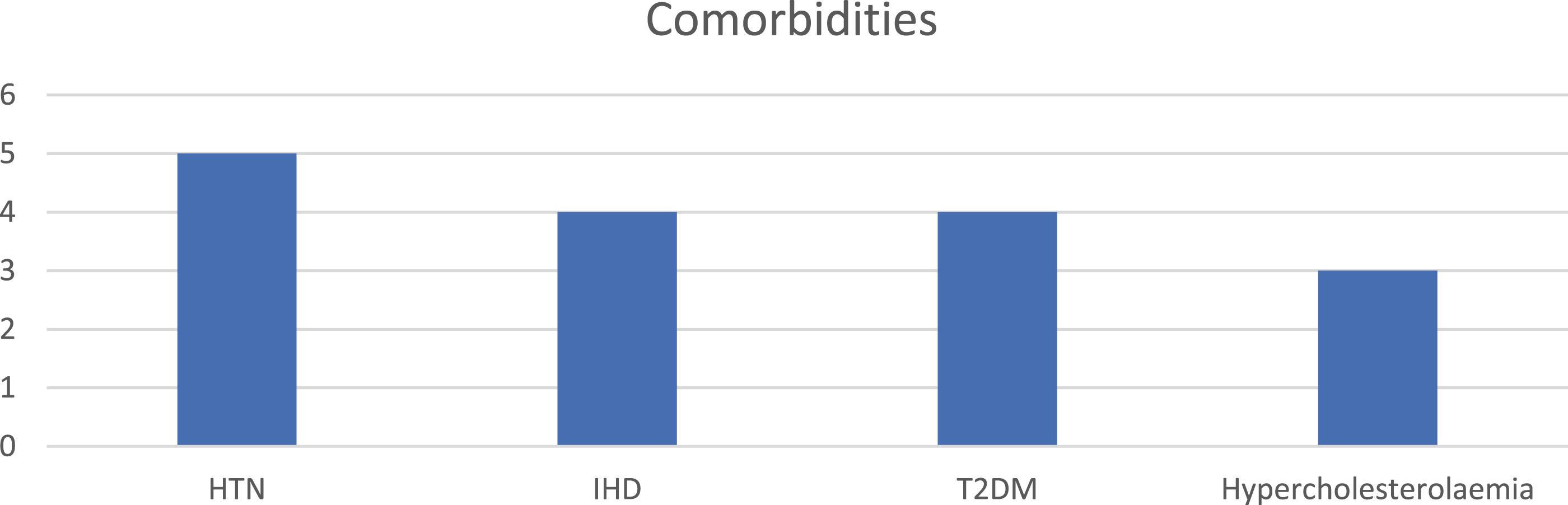
CT Angiogram Proven % Occlusion in Each Case.
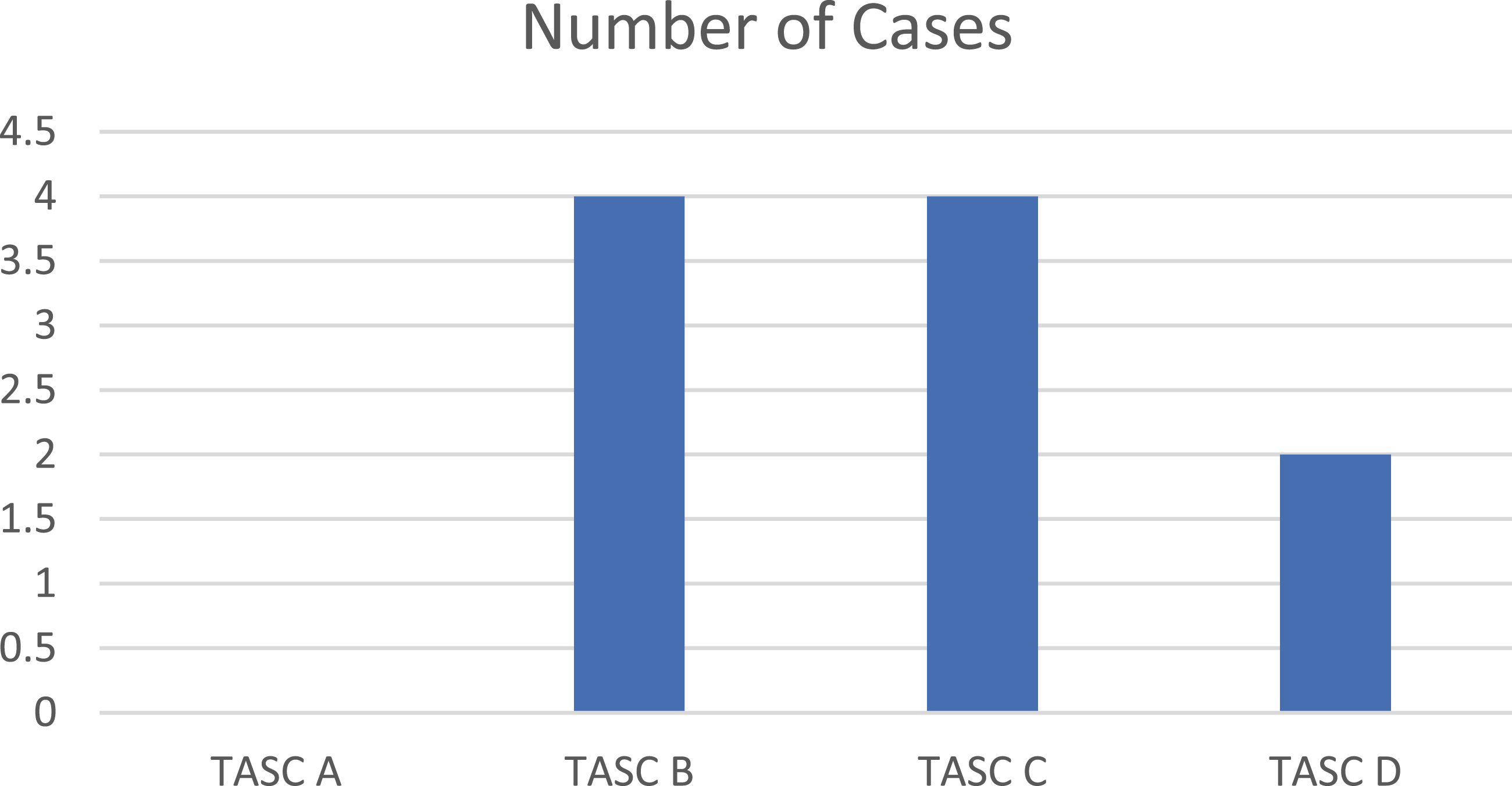
Number of cases of each category in the TASC classification.
In-Hospital Data Representing Length of Stay and Follow-Up.
All the cases were discussed in the vascular multi-disciplinary meeting (MDT) and the reasons for open procedure rather than ET varied from case to case. The reasons included acute on chronic emboli, failed previous angioplasty or occluded stents, risk of dislodging existing thrombus and MDT concluding that ET would be risky.
All cases are alive to date except one case which only survived 3 years after procedure; the cause of death was not recorded in the hospital system. Up to the end of the follow-up, all patients were major amputation free.
Two cases had to return to theatres. The first case returned to theatre for a re-exploration for suspected bowel ischaemia which was negative. The second case had to return for femoral embolectomy which was successful. One patient had transient post-op AF and another had transient post-op ileus. One patient was readmitted within 30 days of discharge for urosepsis.
Discussion
Endovascular treatments of aorto-iliac occlusive disease using angioplasty and kissing stents are widely used. However, the long-term patency rate is still inferior to surgery according to a recent systematic review with a primary patency rate of 69%. 4 A high re-intervention rate of 11% was also reported for the kissing stents. 5
Open surgical techniques include anatomical bypass grafting using aorto-bifemoral, aorto-iliac or extra-anatomic bypass grafting such as femoral-to-femoral, iliac-femoral or axillo-femoral bypasses. 6 Overtime, the popularity of aortic endarterectomy (AE) declined among the surgeons, mostly drifting towards the bypass procedures. 7
While all open procedures share a similar primary patency rates at 5-year follow-up (86 to 88%), EA carries the lowest burden in terms of mortality (2.7%) and morbidity (2.7% local complications and 12.5% systemic complications) when compared to the bypass procedures. 7 It has the advantages of being anatomical, maintaining flow into the iliac arteries and less use of artificial graft material which allows utilization in the infected fields as well as men who would like to preserve their sexual function after the procedure. EA does not require contra-lateral inflow and thus does not carry the risk of steel.
Despite these advantages, bypass remains more popular among current day surgeons in contrast to 50 years ago when the standard treatment of aorto-iliac occlusive disease was AE. That drift towards bypassing may have been because bypassing diseased iliacs were more feasible than performing an endarterectomy on them. 8 This in turn reduced the available cases for surgical training in AE procedures.
The use of artificial graft material during the bypass procedures carries an inherent risk of thrombosis and occlusion. The primary patency rates of bypass procedures are 86.2% at 5 years and 77.6% at 10 years. 9 On the contrary, AE is associated with a high primary patency rate (99% at 5 years and 96.5% at 9 years). 10 In our unit, 43 aorto-bifemoral bypass procedures were performed during the same time frame. Out of the 43 procedures, two patients had limb occlusions (4.6%) and three patients died translating to a 7.0% mortality rate. The main anatomical criteria for choice between the two procedures were the presence of infra-renal aortic disease extending to the CIA/EIA. While the data we have cannot reliably compare the two procedures, there is a trend towards better survival and patency in the AE group.
Although thinning the artery while doing AE theoretically increases the risk of aneurysm, the clinical data showed no association with aneurysmal formation. Bypass procedures were associated with a 5% aneurysmal formation while EA did not carry a risk as per a published case series of 205 patients followed up for 10 years. Graft infection rates were higher in bypass patients compared to EA patients in the same series. 8
In this series, bovine pericardial patch was used for closure. This was used to ensure a wide lumen is maintained during the repair. The bovine pericardial patch is proven to be of similar infection resistance to vein grafts. Arteriotomy repair in infected fields using the bovine pericardial patch has been reported with a 98% success rate after 2 years follow-up without evidence of recurrent infection or rupture. 11 Similarly, no infections were reported in the cases included in this study.
There was no mortality in the case series; this may not represent a true reflection of mortality as the case numbers were low. However, it still shows a general trend of decreased mortality. This trend may be because of two main reasons; the first reason is the presence of an experienced surgical team including a dedicated vascular anaesthetist, vascular scrub nurse, two operating vascular consultants and well trained post-operative surgical nurses who are experienced in post-op vascular patients care in our surgical high dependency unit (HDU) in which all the patients were admitted routinely, post-operatively except if they needed ITU admission. The second reason is the high flow rate. A total number of 296 elective open aortic aneurysm repairs were carried out in the unit over the last five years and a total of 53 open aortic revascularization procedures were performed over the last 10 years. Another limitation of the article is its nature as a retrospective case series.
Conclusion
AE is a procedure that should be considered in selected cases where endovascular approach is not feasible. There is a trend towards lower mortality than the historic data available in literature. Larger case series or registry data may be required to accurately estimate the current day mortality and morbidity figures.
Footnotes
Author Contributions
Ahmed ELshiekh: Data collection, writing, statistics and design.
Christy Varghese: Data collection, statistics and writing.
Tony Jaipersad: Design, writing and revision.
Arun Pherwani: Design and revision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.