
Abstract
Although there have been a few case reports of spontaneous rupture of pelvic veins, such as the iliac vein, to date, there have been no reports of spontaneous rupture of the ascending lumbar vein. Here, we report a case of spontaneous rupture of the ascending lumbar vein for the first time. A 66-year-old woman visited the emergency department due to the swelling of the left lower limb for 2 hours. After admission, the patient developed symptoms of pain in the left lumbar region, as well as symptoms of shock, such as increased heart rate and decreased blood pressure. During emergency venography, it was found that the ascending lumbar vein was ruptured, which was accompanied by the compression and occlusion of the iliac vein (May-Thurner syndrome). During the endovascular surgical treatment, a covered stent was placed in the iliac vein, and the occluded common iliac vein was treated with a bare stent. Immediately after the surgical procedure, the patient’s abdominal computed tomography examination showed the formation of a large retroperitoneal haematoma, and continuous routine blood parameter monitoring showed that haemoglobin was stable. Postoperative recovery was uneventful, and the patient was discharged on the ninth postoperative day.
Introduction
Spontaneous pelvic vein rupture is a rare but potentially fatal event. Many previous case studies have reported spontaneous iliac vein rupture. The rupture is more likely to occur in the left common iliac vein and external iliac vein. Most cases are accompanied by occlusion of the left common iliac vein, which is also known as May-Thurner syndrome (MTS). The ascending lumbar vein is the communicating vessel between the iliac vein and the lumbar vein. Under normal circumstances, the vein is slender. However, in some patients with MTS, the ascending lumbar vein can be enlarged compensatorily. The spontaneous rupture of the pelvic vein is difficult to correctly diagnose at an early stage. Patients often develop abdominal or back pain for unknown reasons and then the shock symptoms progress rapidly. Some patients have sudden lower limb swelling or movement disorder and lack specific clinical manifestations. Even if the patient presents to the emergency department (ED) promptly and undergoes a computed tomography (CT) examination of the pelvis and abdomen, most of the time it can only reveal a large retroperitoneal haematoma, and the specific bleeding site is difficult to identify by CT examination.
To date, there have been no reports of spontaneous rupture of the ascending lumbar vein. In this case report, we correctly diagnosed a case of spontaneous rupture of ascending lumbar vein through venography. After endovascular treatment, the patient’s bleeding was arrested, and her vital signs were gradually stabilised. A follow-up CT scan revealed that the retroperitoneal haematoma has decreased. The patient was discharged 9 days after the operation without any complications. The patient remained swelling-free of the left lower extremity, and the stent was still patent at 3-month follow-up.
Case Presentation
A 66-year-old female patient without prior underlying disease presented to the ED due to swelling of the left lower extremity. The patient had no abdominal pain or lumbar back pain at the time of the ED visit. Laboratory examination showed that the D-dimer was 12,363 ng/mL. The lower extremity venous duplex examination revealed that the blood flow of the popliteal-femoral vein was extremely slow, but no clear evidence of thrombosis, such as flocculent echoes in the vein, was found. The patient was diagnosed with suspected deep venous thrombosis of the lower extremity and was admitted to the Vascular Surgery Department by the emergency physician in consultation with the vascular surgeon.
Immediately after the admission, the patient developed mild lower abdominal pain and left lumbar pain, which was not considered in the initial diagnosis. As the routine treatment procedure in patients with deep venous thrombosis, we decided to perform emergency venography to determine whether the patient had deep venous thrombosis in the lower extremities.
After transfer to the operating room, the patient’s lower back pain was severely increased. The ECG monitoring showed that the patient’s heart rate gradually increased to approximately 100 beats/min compared with 70 beats/min at the time of admission, accompanied by a progressive blood pressure decline from 120/75 mmHg to approximately 80/50 mmHg, and the patient developed shock symptoms such as dampness and sweating throughout the body.
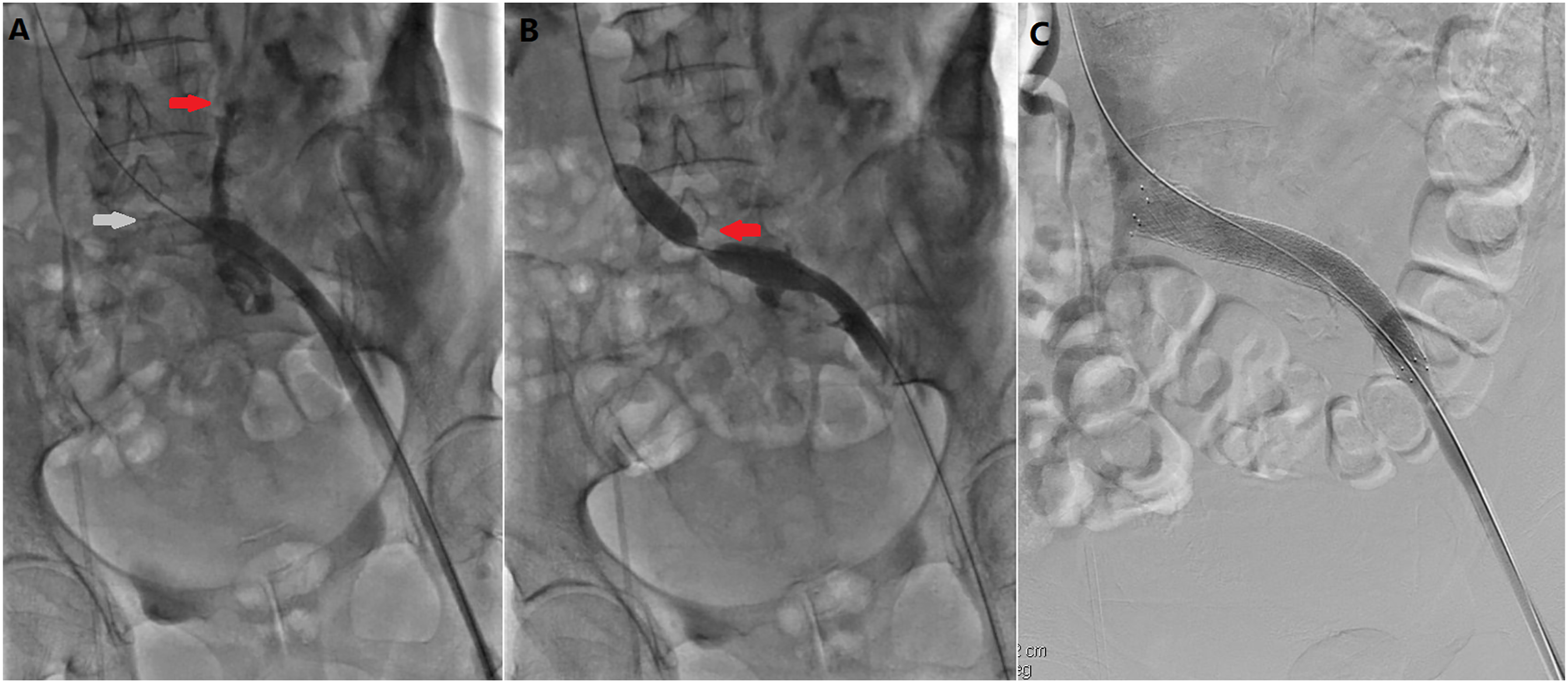
Ascending venography was performed through an indwelling needle in the dorsal vein of the foot. The venography images showed that the calf, popliteal and femoral veins of the patient were unobstructed, but the venous flow rate was slow. When the calf was squeezed to make the contrast agent flow to the iliac vein, there was surprisingly an obvious rupture point on the ascending lumbar vein with the severe extravasation of the contrast agent. The ascending lumbar vein was connected to the internal iliac vein, and the rupture site was approximately 5 cm away from its connection with the internal iliac vein (Figure 1). We also found a small amount of thrombosis in the patient’s iliac vein, and a small thrombus from the external iliac vein was observed floating into the retroperitoneal space through the rupture seen on the real-time images of the radiography (Supplementary Material Video 1). We immediately punctured the left femoral vein and confirmed the rupture of the ascending lumbar vein accompanied by occlusion of the left common iliac vein. There was no obvious venous thrombosis on imaging, such as filling defects in the iliac vein. Terumo Radifocus Glidewire (hydrophilic coated guidewire, .035 in × 260 cm; Terumo, Tokyo, Japan) was adopted to establish intravascular access through the left iliac vein occlusion. First, a balloon catheter (14 mm × 80 mm, Armada35, Abbott, Abbot Park, IL, USA) was used to expand the occluded left common iliac vein. After the venous flow was partially recovered, the angiogram showed that contrast agent overflow through the ruptured vein decreased. Since the venogram showed that the ascending lumbar vein communicated with the internal iliac vein, we then applied a covered stent (13 mm × 50 mm, Viabahn, WL Gore & Associates, Flagstaff, AZ, USA) to cover the area where the internal iliac vein merged into the iliac vein and then applied a bare metal stent (14 mm × 80 mm, SMART, Cordis, Miami, FL, USA) to cover the left common iliac vein and enter approximately 10 mm into the inferior vena cava without completely covering the right common iliac vein. A post-procedure angiogram showed that no contrast agent spilled through the vein rupture site and there was no endoleak. The common iliac vein was restored to patency with no residual stenosis (Figure 2). During the surgery, approximately 1000 mL of fluid and 3 µof suspended red blood cells were rapidly infused intravenously. The patient underwent a CT scan of the abdomen immediately after the surgery, and the examination demonstrated the formation of a large retroperitoneal haematoma (Figure 3). Antegrade venogram showing an obvious rupture point on the ascending lumbar vein with severe contrast agent extravasation. Endovascular surgical treatment procedure. (A) Rupture of the ascending lumbar vein accompanied by the occlusion of the left common iliac vein. (B) Balloon dilation with obvious wasting due to iliac venous compression. (C) Venogram showing no contrast agent extravasation or residual stenosis of the iliac vein lumen after stent implement. Computed tomography scan performed immediately after surgery revealing a large retroperitoneal haematoma extending to the level of the right kidney.

We closely monitored the patient’s routine blood parameters after the surgery. Although the patient still had persistent lower back pain symptoms, the ECG monitoring showed that the patient’s heart rate gradually recovered to approximately 70 beats/min, and the patient’s lower limb swelling was completely relieved. After 3 consecutive days of routine blood examinations, the patient’s haemoglobin stabilised at 90 g/L, and we started to give rivaroxaban for anticoagulation therapy. The patient underwent a CT scan again on the eighth day after surgery, and the results showed that the patient’s retroperitoneal haematoma was significantly reduced (Figure 4). The patient was discharged from the hospital on the ninth day after surgery, and the back pain on the left side completely disappeared. Computed tomography scan performed 8 days after surgery revealing a reduction of the retroperitoneal haematoma (A and B) perirenal haematoma mostly resolved at the level of the L1/2 vertebral body (C) retroperitoneal haematoma significantly regressed at the level of the S1 vertebral body.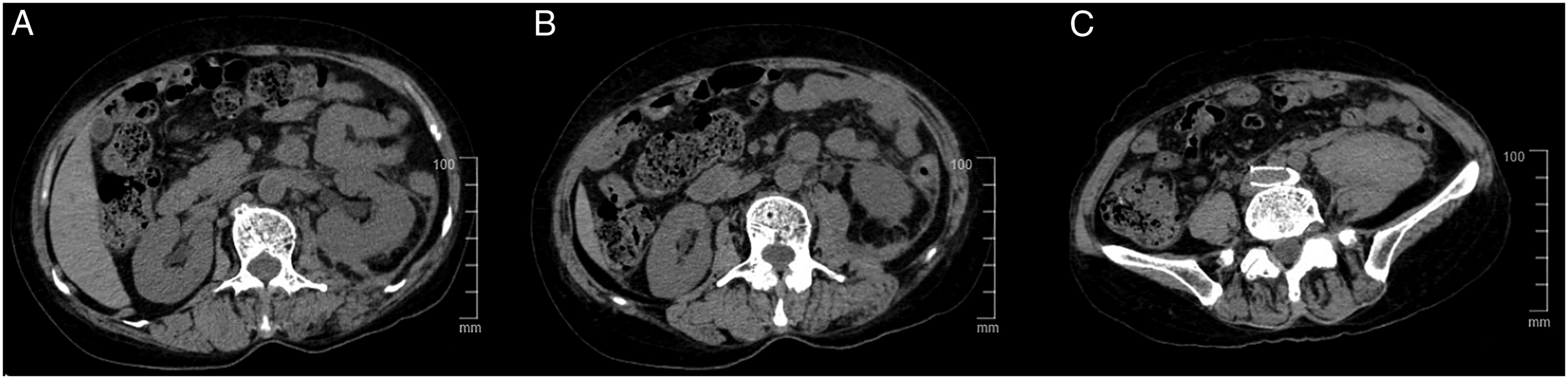
Three month later, the follow-up abdominal contrast-enhanced CT revealed complete regression of the retroperitoneal haematoma and patency of the iliac vein stent without significant stenosis (Figure 5). Contrast-enhanced computed tomography scan performed 3 months after surgery revealing complete regression of the retroperitoneal haematoma and patency of the iliac vein stent. (A) horizontal plane (B and C) coronal plane.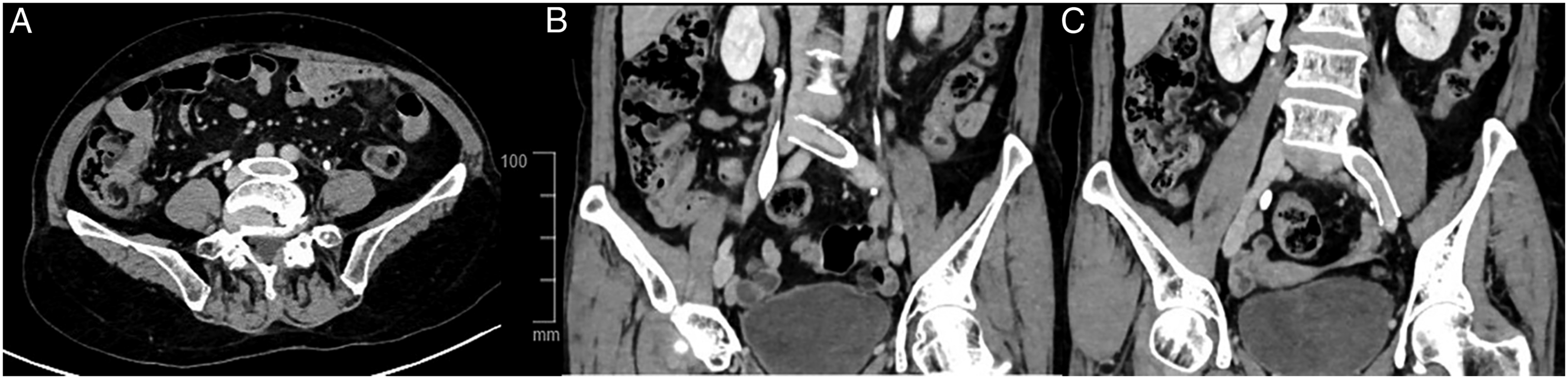
Informed consent was signed by the patient for publication of this case report and accompanying images.
Discussion
Spontaneous pelvic venous rupture is rare in clinical practice. Previous case studies reported more common uterine–ovarian venous rupture in pregnant women. Spontaneous rupture of the iliac vein has also been reported in some cases. Nevertheless, publications of this type of case are still very few. 1 The rupture of the utero-ovarian veins during pregnancy is mainly due to the varicose veins caused by the increase in pelvic pressure. In this present case, the patient was an elderly woman, and the characteristics of the condition were similar to the rupture of the iliac vein. 2 Spontaneous iliac vein rupture usually occurs in the left iliac vein in middle-aged and elderly women, but the aetiology is not fully understood. At present, the main causes are considered to be the following: (1) Increased vascular fragility: The level of hormones in middle-aged and elderly women decreases. Especially in perimenopausal and postmenopausal women, the level of oestrogen drops significantly, causing smooth muscle relaxation, softening of collagen fibres, decreased vein elasticity and increased vascular fragility, which makes the vein wall prone to rupture. (2) Elevated venous pressure: Elevated venous pressure is a direct cause of spontaneous venous wall rupture. Strenuous exercise, such as coughing and squatting, is a common cause, which can easily cause a sudden increase in intravenous pressure and cause venous wall rupture. (3) Anatomical factors: The right common iliac artery crosses the anterior wall of the starting end of the left common iliac vein, and the left common iliac vein is located between the spine and the right common iliac artery, so the pressure in the left iliac vein is relatively high. (4) Venous thrombosis: Sudden venous thrombosis leads to obstruction of the venous outflow, increased lumen pressure and venous rupture.
In this case, the ruptured lumbar ascending vein occurred. The ascending lumbar vein is a blood vessel that connects the iliac vein and the lumbar vein. It is relatively slender under normal circumstances, but when there is compression of the iliac vein, it can be enlarged compensatorily as an outflow channel to the pelvic and lower limb veins. It has been reported that stent placement in the ascending lumbar vein is effective in treating refractory chronic occlusion of the inferior vena cava to relieve venous hypertension in the lower extremities. 3 There is no valve in the ascending lumbar vein, and the vein wall is thin. It is prone to iatrogenic injury during spinal surgery, even leading to uncontrollable bleeding. Therefore, in order to reduce the possibility of such bleeding events, a venography of the area can be performed before surgery to provide the surgeon with information on the eventually increased risk. 4 In most cases, the ascending lumbar vein connects to the common iliac vein, and in some variants, it connects to the internal iliac vein. 5 We believe that the main cause of spontaneous rupture of the ascending lumbar vein in this patient was venous hypertension caused by iliac vein compression and compensatory thickening of the lumbar ascending vein. The patient’s initial symptom was lower extremity swelling, and acute iliac vein thrombosis may have occurred. From the angiogram, we also found that a small thrombus spilled through the site of the ruptured lumbar ascending vein. Sudden iliac venous thrombosis aggravated venous hypertension and resulted in the rupture of the patient’s chronic compensatory thickened lumbar ascending vein.
The clinical manifestations of spontaneous pelvic vein rupture are mainly persistent pain symptoms, which can progressively worsen. The pain is mostly located in the lower abdomen, waist or iliac fossa and may be accompanied by swelling of the affected limb, such as rapid bleeding or continuous bleeding, and may be accompanied by symptoms of shock. Due to the variety of clinical manifestations and lack of specificity, it is difficult to diagnose the condition at an early stage, and the mortality rate is high. The treatment methods reported in the literature are mainly open surgical repair, and there are few cases of successful endovascular surgical treatment.6,7 Moreover, in previous case reports, after the confirmation of the rupture of pelvic veins such as iliac veins, the surgeon often repaired the rupture by suturing and did not perform concurrent or staged venography to determine the presence of May-Thurner syndrome (MTS). We believe that venous hypertension caused by compression and stenosis of the iliac vein plays an important role in the pathogenesis of spontaneous pelvic vein rupture.
Conclusion
Venography can be employed to diagnose the spontaneous rupture of the pelvic vein early and quickly identify the location of the rupture. Endovascular surgical treatment is safe and reliable for emergency rescue and can effectively reduce the mortality rate and the incidence of complications. For the spontaneous rupture of the pelvic vein, attention should be given to the possibility of the iliac vein compression syndrome. If iliac vein compression is confirmed by venous angiography, stent implantation should be conducted to relieve the stenosis to alleviate venous hypertension. This also applies to the patients who have undergone open surgery without making an initial clear diagnosis. If spontaneous iliac veins and other pelvic vein ruptures are found during open surgery, in addition to suture and repair of the ruptured vein, concurrent or staged phlebography should be considered to determine whether the iliac vein is patent.
Footnotes
Statement of Patient’s Consent
Informed consent was signed by the patient for publication of this case report and accompanying images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.