
Abstract
Hybrid endograft combinations of two or more different types of covered stents are rarely reported to treat complex abdominal aortic aneurysm cases or primary and secondary endoleaks. Clinical and laboratory data regarding the clinical efficacy and mechanical stability of such combinations are lacking. Based on a recently published case report, we describe and comment on the hemodynamic profile of a representative simulated hybrid case of AFX and Nitinol-based proximal cuff and support the stability of this combination in non-angulated cases.
Keywords
We read with great interest the recent article by Smith and Farivar, describing the successful management of a failed endovascular aortic aneurysm repair by means of a hybrid combination of a Cook Zenith Fenestrated (ZFEN) device proximally and an AFX2 (Endologix, Inc, Irvine, CA, USA) bifurcate caudally, with the latter accommodating directly onto the flow divider of the previous bifurcated abdominal endograft. Efficient sealing and adequate overlap were achieved intraoperatively and during the following 1 year, although limited experimental and clinical data are available, as the Authors claim. 1 Based on this excellent technical conception, we find very useful to share our recently demonstrated experience regarding the hemodynamic profile of such hybrid solutions.
The combination of the AFX aortic stent-graft containing a chromium–cobaltium endoskeleton with a Nitinol-based Endurant (Medtronic, Inc., Santa Rosa, CA, USA) proximal aortic cuff has been scarcely described in the literature as a means of applying extra radial force to improve sealing in challenging infrarenal geometries of abdominal aortic aneurysms (AAA).2,3 Recently, we performed patient-specific computational fluid dynamics (CFD) simulations and calculated the displacement forces in 11 AAA cases treated either with AFX, Endurant, or the AFX–Endurant combination. 4 Our study showed that these forces were lower in the hybrid AFX–Nitinol-based aortic cuff cases with non-angulated necks compared to the classic AFX and Endurant groups. This held true both for the proximal cuff segment and the main body, as well as for the iliac limbs (outlet). Furthermore, the infrarenal angulation showed to attenuate this effect and to promote the classic AFX design.
The aforementioned geometrical pattern of the particular hybrid combination (i.e., AFX with Nitinol cuff in non-angulated necks) seems to have beneficial hemodynamic profile with respect to the magnitude and distribution of hemodynamic indices related to thrombosis induction, that is, RRT (relative residence time), OSI (oscillatory shear index), and time-averaged wall shear stress (TAWSS) (Figure 1). Indeed, the percentage of areas with high RRT over the entire endograft, the main body, and the right/left iliac limbs were 4.32%, 5.15%, 0.11%, and 1.64%, respectively, representing the lowest values comparing to the other cases of our study.
4
High values of TAWSS were represented only at a narrow band of the main body distally, whereas the central segment (area of interest for future adverse effects) showed very low values. Moreover, high (>.4) OSI values were limited only to the transition zone between the neck and the main body, the distal part of the iliac limbs, and the posterior surface of the main body, unlike the more extended distribution on the surface of the other endograft models. Contours of relative residence time (RRT; right), oscillatory shear index (OSI; middle), and time-averaged wall shear stress (TAWSS; left) on a computationally reconstructed 3D model comprising the AFX bifurcate and a Nitinol-based central cuff.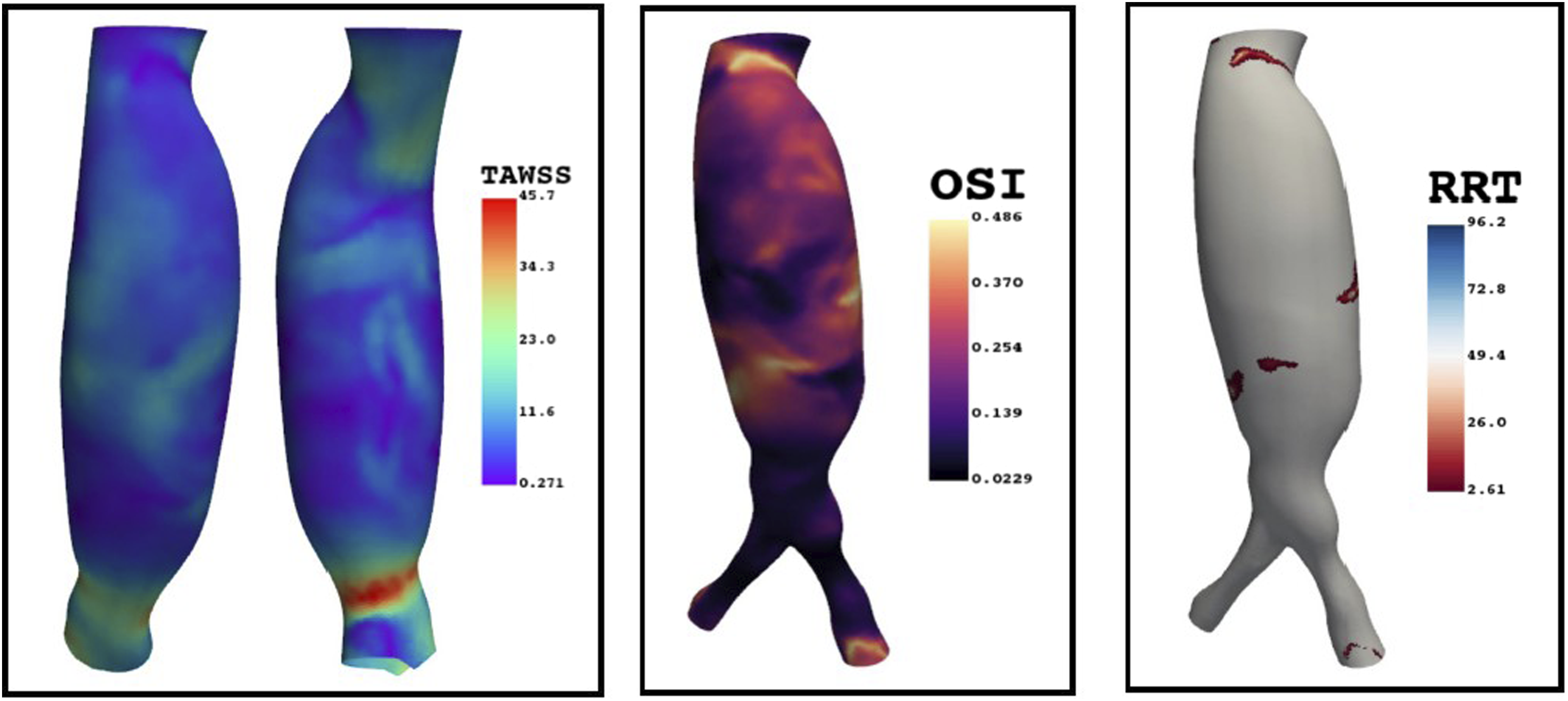
While theoretical concerns are raised with respect to the mechanical stability of the interface between the externally located chromium–cobaltium endoskeleton and the innerly placed Nitinol cuff exoskeleton as described in the literature so far, the presented combination in the case of Smith and Farivar places these structures vice versa, with these metallic skeletons separated by two fabric sheets (externally Dacron and internally PTFE), prohibiting any sliding and consequent instability between these metallic segments, especially with respect to the less stiff AFX.1,2,5
As can be also seen, the accommodation of the AFX onto the flow divider minimizes the splay and angulation of the iliac limbs which has been associated with significantly greater distraction forces in fenestrated stent-grafts. 6 Last, the selection of the Ovation limbs to complete distal relining takes advantage of the unique combination of flexibility, low profile, and high Nitinol density of this design. 7
To conclude, the particular hybrid treatment presented by the authors combines in a unique way material structures and geometrical configurations that suggest a mechanically and hemodynamically promising option to technical efficacy and durability of clinical success.
Footnotes
Acknowledgments
The numerical results of the presented case are part of a study approved by the Institutional Ethical-Scientific Committee of the University Hospital of Alexandroupolis (No. 18725/1934, 05-12-2016).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.