
Abstract
Vasculopathy of systemic sclerosis (SSc) is known to lead to severe limb ischemia and is often associated with macrovascular diseases. Revascularization of proximal macrovascular lesions that cause limb ischemia in patients with SSc has been recommended; however, it has rarely been reported for lesions below-the-elbow (BTE) involving the palmar artery. A 66-year-old female patient with SSc experienced critical hand ischemia (CHI) with gangrene of the left third finger that failed to respond to conventional pharmacological treatment. Angiography revealed total occlusion of the distal radial and ulnar arteries with a palmar artery lesion. Balloon angioplasty was performed for bilateral occlusive lesions around the wrist, which improved antegrade flow to the digital artery. Endovascular therapy may be a feasible option for BTE lesions involving palmar artery disease, presenting with CHI in SSc, when conventional conservative treatments fail.
Introduction
Systemic sclerosis (SSc) is a connective tissue disease characterized by tissue fibrosis and microvascular abnormalities. Raynaud’s phenomenon and digital ulcers (DUs) are known clinical manifestations of SSc-related vasculopathy. 1 Recently, several studies have demonstrated that macrovascular diseases are common in patients with SSc associated with severe limb ischemia.2,3 Moreover, the UK Scleroderma Study Group recommends that any contributory cause to critical digital ischemia should be treated promptly, such as management of proximal large vessel diseases with angioplasty. 2
Herein, we report a case of endovascular therapy (EVT) for total occlusion resulting in a below-the-elbow (BTE) lesion, including a palmar artery lesion in a patient with critical hand ischemia (CHI) associated with SSc.
Case Presentation
A 66-year-old female with SSc had experienced Raynaud’s phenomenon and a small DU due to cold exposure, which improved with conservative management and wound care. However, she had ischemic pain and a refractory DU in the third finger of the left hand, regardless of cold exposure. The wound worsened and progressed to necrosis despite conservative pharmacotherapy, including vasodilators, bosentan, and wound care for 3 months (Figures 1(A) and 1(B)). As further complications of anti-phospholipid syndrome were identified, anticoagulation therapy was initiated; however, the gangrene did not improve. The skin perfusion pressure (SPP) value of the left hand was 22 mmHg and 19 mmHg for the palm and back, respectively. Furthermore, angiography revealed total occlusion of the left distal radial artery (RA) and ulnar artery (UA), including the palmar arch (Figure 1(C)). We attempted endovascular angioplasty for the BTE lesions that failed to respond to conventional treatment, in order to salvage the upper limb. Findings of the left hand and diagnostic angiography. (A, B): Gangrene of the left third finger. (C): Distal radial artery and ulnar artery occlusion in angiography.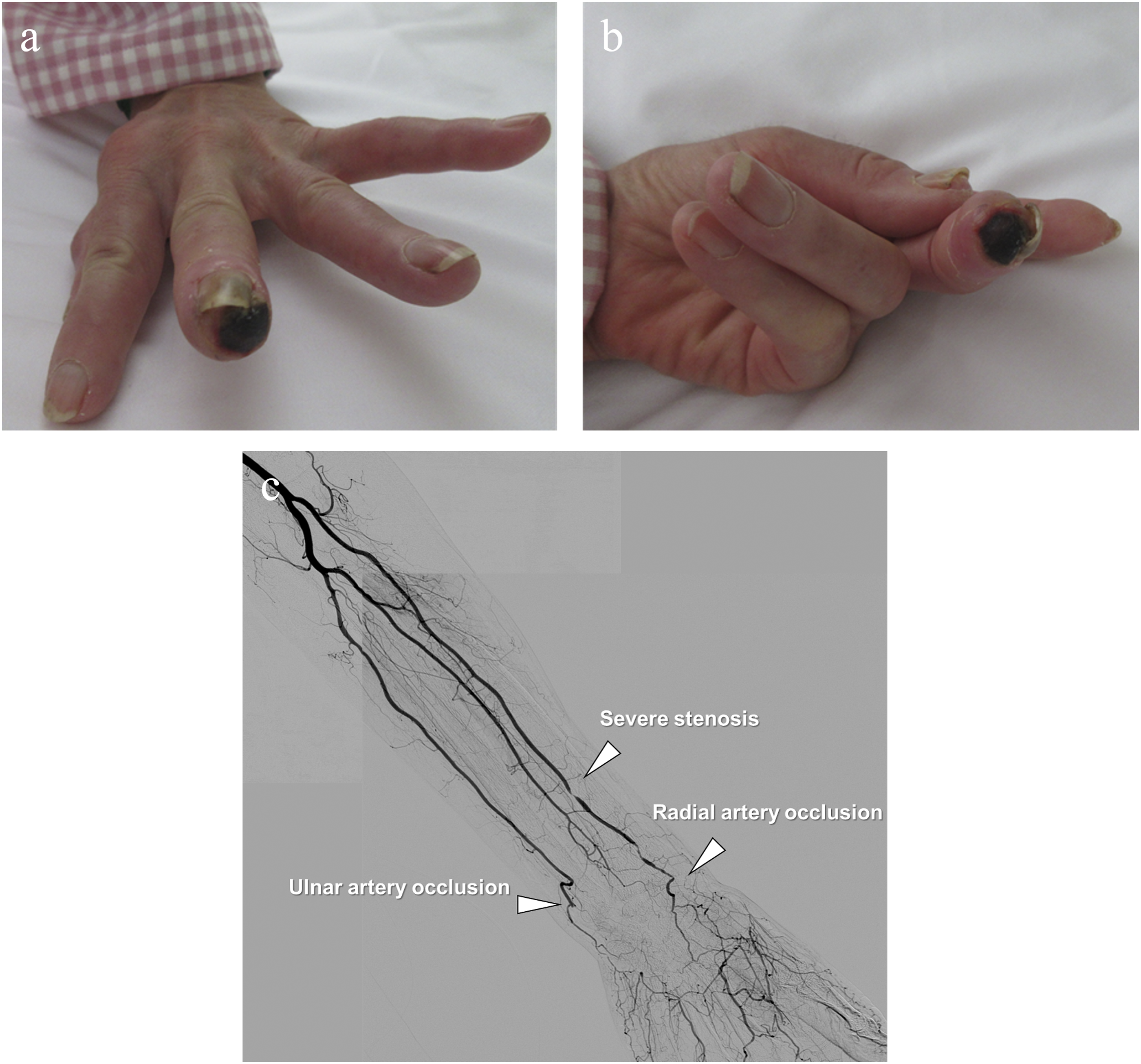
The 5-Fr Glidesheath slender (Terumo. Corp., Tokyo, Japan) was inserted ipsilaterally via the left brachial artery. First, a .014” hydrophilic guidewire with a 3 g tip load (Asahi Intecc, Nagoya, Japan) was advanced successfully with a microcatheter (Tokai Medical Products, Aichi, Japan) support through the UA to the palmar artery (Figures 2(A) and 2(B)). Similarly, the hydrophilic guidewire was progressed to the occluded lesion in the RA; however, it could not pass into the palmar artery (Figure 2(C)). Although the tip load of the guidewires was stepped up to 12 g, the guidewires were advanced into the subintimal space, and the antegrade approach failed. Therefore, we attempted a retrograde approach through the palmar arch. The hydrophilic guidewire was advanced to the RA via the palmar arch with a microcatheter support; however, it progressed into the subintimal space. Intravascular ultrasound confirmed that the antegrade and retrograde guidewires were close to each other in the subintimal space around the total occlusion lesion; therefore, the retrograde guidewire was able to enter the true lumen of the RA after antegrade 2 mm balloon inflation and deflation using the reverse controlled antegrade and retrograde subintimal tracking (CART) technique (Figure 2(D)). Thereafter, a 2 mm balloon was dilated from the occluded RA and UA to the palmar artery (Figures 2(E) and 2(F)). Final angiography showed optimal direct antegrade flow to the finger (Figure 2(G)). The ischemic pain improved after revascularization, and the SPP value increased significantly (palm/back; 60/62 mmHg). The gangrene of the third finger gradually healed over 2 months, and follow-up with ultrasonography revealed restenosis of the ulnar artery but patency of radial artery (Figure 2(H)). Endovascular procedure and findings of the left hand after revascularization. (A): Initial angiography. (B): Tip contrast injection via a microcatheter after penetrating the ulnar artery occlusion lesion. (C): An antegrade wiring to the radial artery occlusion failed. (D): Reverse controlled antegrade and retrograde subintimal tracking technique. (E, F): 2 mm balloon dilation at the ulnar and radial artery occlusion sites. (G): Optimal results on final angiography. (H): Progression of healing after 2 months.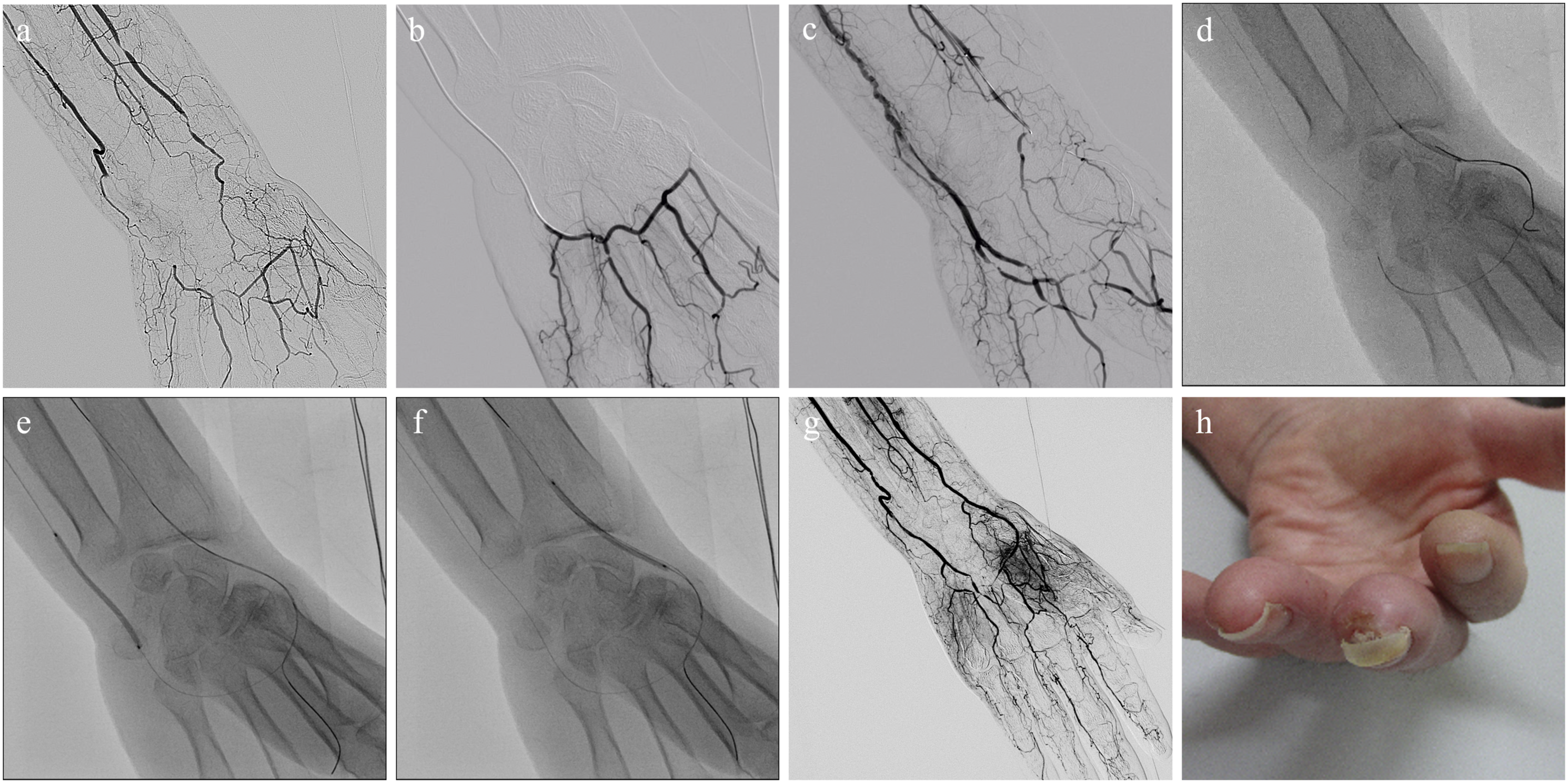
Discussion
SSc-related vasculopathy has structural (intimal hyperplasia and intravascular micro-thrombus) and functional (abnormal vascular contraction) effects on blood vessels, resulting in limb ischemia. The European League against Rheumatism recommends pharmacotherapy for DU in patients with SSc, including intravenous iloprost, PDE-5 inhibitors, and bosentan. 1 Although treatments may effectively improve functional abnormalities of the microvasculature, they have a limited effect on macrovascular diseases, which cause reduction of in-flow. All interventions, including revascularization, for treatable causes contributing to ischemia should be considered in patients with CHI associated with SSc. 2 Although there have been case reports of EVT for proximal large vessel lesions, 4 EVT for distal macrovascular lesions, especially those around the wrist, has been rarely reported.
This report describes a rare case of technically and clinically successful revascularization in a BTE lesion with total occlusion from the distal RA and UA to the palmar artery in a patient with SSc. Endovascular therapy for BTE lesions in patients with CHI associated with atherosclerosis has been reported as a feasible treatment option for revascularization5-8; therefore, endovascular intervention for BTE lesions in patients with CHI associated with SSc might be considered as a treatment option. An antegrade approach should be attempted first in BTE interventions, but a retrograde approach via the palmar arch may be useful as an alternative if this attempt fails.9-11 This retrograde revascularization technique may improve the technical success rate of EVT for BTE lesions; however, it has a potential risk of palmar artery injury. Therefore, the retrograde procedure should involve the use of low-profile devices and be considered only when the conventional antegrade approach fails. In addition, the reverse CART technique, in which a retrograde wire crosses the subintimal space after balloon dilation with an antegrade balloon, might potentially reduce excessive manipulation of retrograde guidewires. 12 This technique has become the dominant retrograde wire crossing technique in the coronary intervention of CTO lesions and may be applicable to CTO lesions in peripheral arteries. 13
Whether a single vessel or multiple vessels intervention in the below-the-knee lesion is the optimal endpoint in chronic limb-threatening ischemia (CLTI) patients is still controversial.14,15 Asian multidisciplinary consensus statement of CLTI management suggested that the goal of intervention for symptomatic isolated infrapopliteal artery diseases should be established at least 1 straight-line flow to the foot. 16 In addition, if technically feasible, a strategy to reconstruct as many arteries as possible is practical because this strategy can certainly provide robust blood flow to a severely ischemic foot and may enhance wound healing. In this CHI case, we decided to revascularize as many vessels as possible in the first session in order to obtain sufficient blood flow to improve rest pain and promote wound healing. Without excessive wire manipulation, the retrograde wire progressed to the proximity of the antegrade wire in the subintimal space and successfully entered the true lumen using the CART technique. However, if there is excessive resistance of wiring, it is also important to complete the procedure by establishing a one straight-line flow to hand at the first EVT session in consideration of the palmar arch injury. Moreover, in the specific subset of SSc, we need to pay attention to vasospasm. It is necessary to clarify whether the angiographic stenosis is an organic lesion, vasospasm, or iatrogenic injury, and avoid unnecessary balloon dilation. Therefore, it is also important to use vasodilators as appropriate during the procedure.
These endovascular techniques could improve the technical success rate and are therefore applicable to SSc patients with BTE lesions. We believe that EVT for BTE lesions may be one of the feasible options of multidisciplinary approaches for CHI in patients with SSc.
Conclusions
Severe upper limb ischemia associated with SSc may involve macrovascular diseases. EVT may be a feasible option for the treatment of BTE lesions involving the palmar artery, presenting with CHI in SSc, when conventional conservative treatments fail.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Informed consent has been obtained from the patient for publication of the case report and accompanying images.