
Abstract
Main Text
Background
Post-dissection aneurysm (PDA) is a serious problem seen in some patients who have survived an aortic dissection. It results in the need for extensive aortic repair 1 or an aneurysm rupture. 2 Various endovascular options have been reported to deal with PDA, including the use of fenestrated/branched devices,3,4 candy plug technique, 5 knickerbocker technique, etc. 6 Closing all communicating channels between true and false lumens is an alternative treatment option particularly in countries where fenestrated/branched devices and other endovascular options are not available. 7 However, if arterial flow remains in the false lumen after all channels are closed, possible treatment options are limited. This case report describes a technique whereby the dissection flap is penetrated in order to embolize the residual arterial flow in the aortic false lumen.
Case Presentation
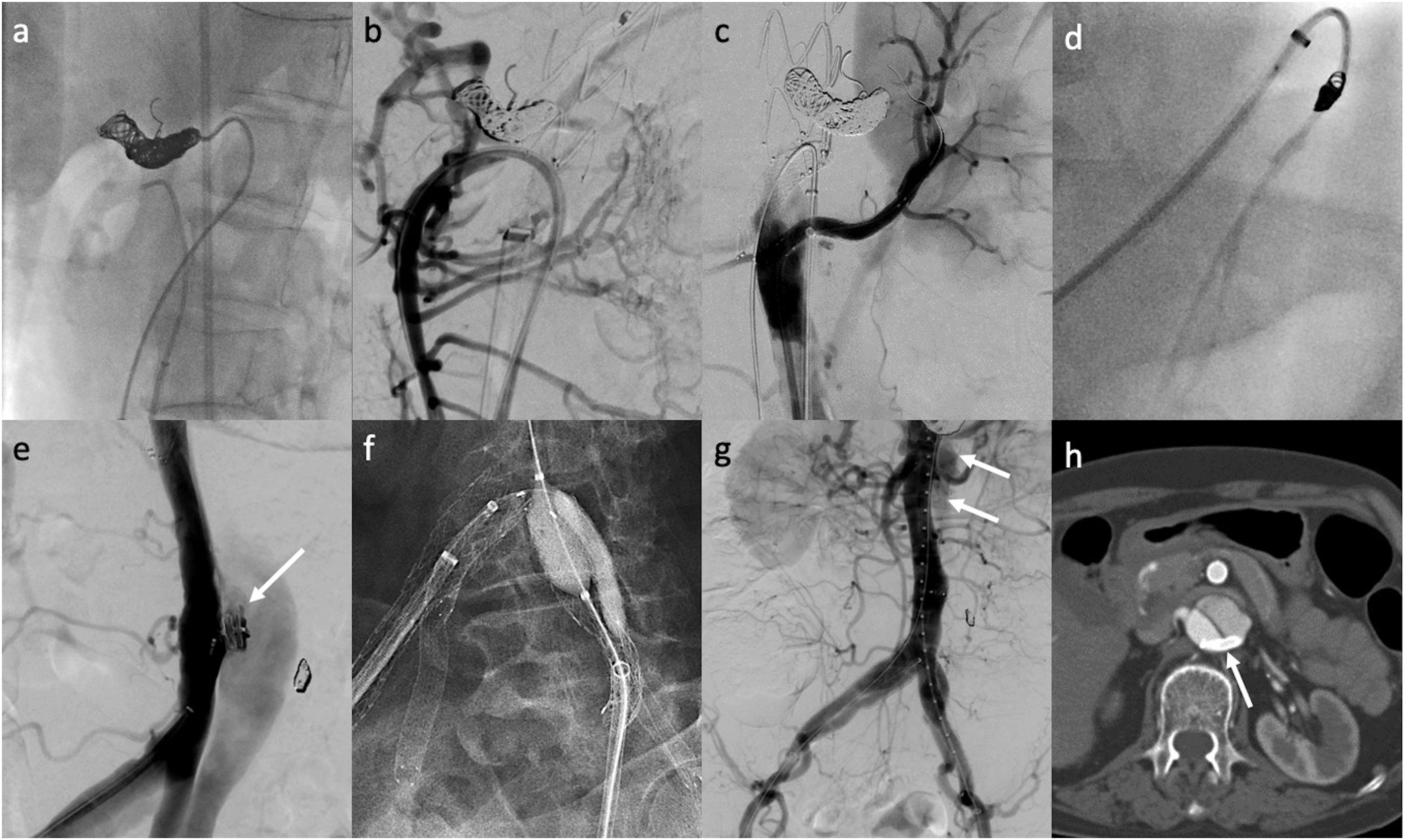
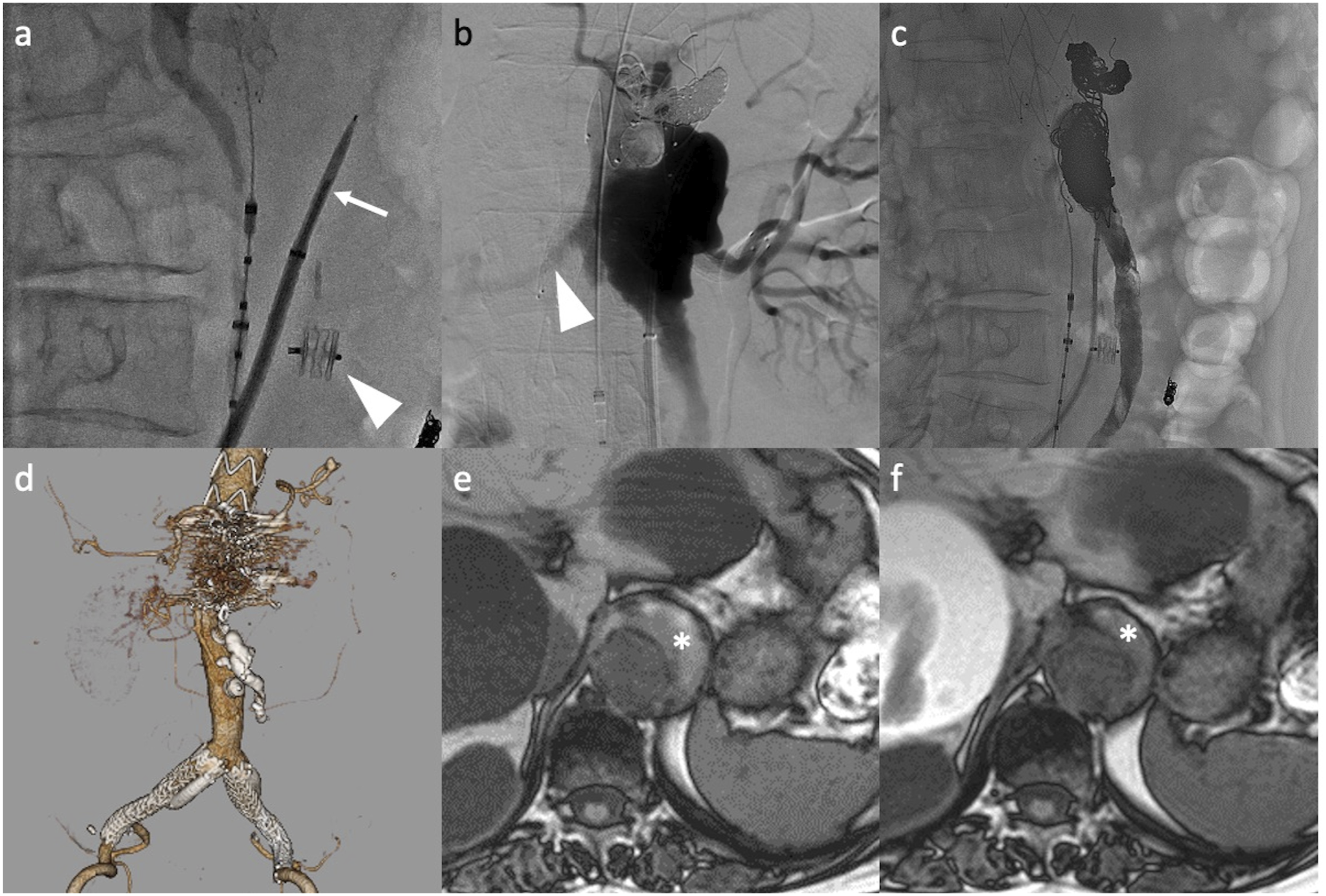
The case was a 64-year-old female who developed a Stanford type A acute aortic dissection (Figure 1). The aortic dissection extended down to bilateral common iliac arteries (CIA). Replacement of the ascending aorta and aortic arch with frozen elephant trunk technique was performed, and the patient discharged uneventfully. There was a residual false lumen flow in the descending thoracic and abdominal aorta. Twenty months later, the patient complained of sudden back pain and was transferred to our hospital. A CT demonstrated another new dissection at the distal edge of the open stent, the cause of which was considered to be stent graft–induced new entry tear. Additionally, the aortic false lumen that had remained since the onset of the type A aortic dissection enlarged during the observation period. An endovascular procedure was planned to exclude the aortic false lumen. Since fenestrated/branched devices were not available in Japan, it was planned to close all channels between the true and false lumen (Figure 2). The superior mesenteric artery originated from the true lumen but had a stenosis at the ostium, which was treated with stent placement (Epic vascular stent 10 mm–6 cm, Boston Scientific, MA, USA). The celiac trunk, 2 left renal arteries, and the inferior mesenteric artery (IMA) originated from the false lumen. To prevent a type II endoleak, embolization of the celiac trunk and the IMA was performed via the false lumen. Before the embolization of the celiac trunk, CT images were evaluated to see the collateral networks between SMA and the celiac trunk. The pancreatic arcade connected the branch of the celiac trunk and that of SMA. Furthermore, there was a replaced right hepatic artery originating from SMA which could work as another collateral network feeding the celiac trunk via an intrahepatic anastomosis. The main entry at the distal end of the open stent in the descending thoracic aorta and the detached ostium of the celiac trunk on the dissected membrane was occluded by deployment of stent grafts (32-28-178 mm and 28-201 mm, TX-alpha, COOK Medical, Bloomington, IL, USA). The detached ostium of the IMA on the dissected membrane was occluded by a 10 mm vascular plug (Amplatzer Vascular Plug II, Abbott Laboratories, IL, USA). To preserve left kidney flow, a VIABAHN stent graft (5x50 mm, W.L. Gore and Associates, Inc, AZ, USA) was deployed, bridging the true lumen and left renal artery via the detached renal artery ostium at the dissected flap. Re-entries at the bilateral iliac bifurcations were occluded with parallel endografting where an Excluder limb (12 mm-10 cm, W.L. Gore and Associates, Inc, AZ, USA) was deployed from the CIA to the external iliac artery (EIA) and a VIABAHN stent graft (8x100 mm) from the CIA to the internal iliac artery (IIA) was placed. Despite the procedure, the false lumen continued to expand with the residual flow at the visceral segment. The origin responsible for the flow was considered to be the detached ostium of either the left or right accessory renal artery; however, this was not able to be confirmed. A cannulation into the detached ostium was also impossible. To obtain access into the false lumen, penetration of the dissected flap was obtained using a trans-septal needle (BM C RF generator needle, Baylis Medical Company Inc, Mississauga, Canada) above the IMA level (Figure 3). For safety, the direction and exact location of the tip of the needle was monitored by intravascular ultrasound (Visions PV .035, Philips, Amsterdam, Netherlands) positioned in the true lumen. Following the successful penetration, a 6F Destination sheath (Terumo, Tokyo, Japan) was advanced into the false lumen. Angiography at the false lumen visualized the patent left accessory renal artery, right inferior phrenic artery, and the true lumen through the unidentified hole. To promote the thrombosis of the false lumen, embolization of the false lumen and a branch was performed. Embolization of the left accessory renal artery was performed using a coil (Target XXL 8 mm–40 cm, Stryker, MI, USA). Embolization of the unthrombosed space of the false lumen was subsequently performed by coils (Interlock-35 Coil Fibered IDC Occlusion, Boston Scientific, MA, USA), which were used as a scaffold for the liquid embolic agent to prevent nontarget embolization, and then, a mixture of Lipiodol (Guerbet, Villepinte, France) and NBCA (B. Braun, Melsungen, Germany) with a ratio of 4:1 was injected to fill the space. After the embolization, an angiogram at the false lumen confirmed the significant reduction of leakage into the true lumen. The access site on the dissected membrane created by the septal needle was closed by a 10 mm vascular plug (Amplatzer Vascular Plug II, Abbott Laboratories, IL, USA). After the embolization, no adverse event such as visceral or spinal cord ischemia was observed. The size of the aorta decreased from 46 to 41 mm at 12 months, with shrinkage of the false lumen after the procedure. CT at the onset of the Stanford type A acute aortic dissection (a)-(d) and 2 years after surgery with frozen elephant technique (e)-(h). (c): the arrow shows the celiac trunk originating from the false lumen, (f): the arrow shows new entry tear at the distal end of the open stent, (g): the arrow shows the expanding false lumen at the origin of the celiac trunk. Procedure detail. (a): coil embolization of the celiac trunk, (b): stenting of the SMA, (c): stent graft placement from the true lumen into the left renal artery which originated from the false lumen, (d): coil embolization of the IMA, (e): closure of the detached hole of the IMA on the dissected membrane using a vascular plug (arrow), (f): stent graft placement in a parallel fashion from the CIA to the EIA and the IIA bilaterally, (g): residual flow in the false lumen (arrows), (h): residual flow in the false lumen, the arrow indicates the stent graft deployed from true lumen to left renal artery. CIA, common iliac artery; EIA, external iliac artery; IIA, internal iliac artery; IMA, inferior mesenteric artery; SMA, superior mesenteric artery. False lumen embolization. (a): penetration of the dissected membrane by a needle (arrow) under IVUS guidance, the arrowhead shows a vascular plug placed at the detached hole of the IMA on the dissected membrane, (b): angiogram at the false lumen, the arrowhead shows the visualized right accessory renal artery via an unidentified hole on the dissected membrane, (c): after embolization of the false lumen by coils and glue, (d): contrast enhanced CT after false lumen embolization shows no apparent enhancement in the false lumen, (e): trans axial image of MRI before false lumen (asterisk) embolization, (f): trans axial image of MRI after false lumen embolization shows shrinkage of the false lumen (asterisk). IMA, inferior mesenteric artery; IVUS, intravascular ultrasound; MRI, magnetic resonance imaging.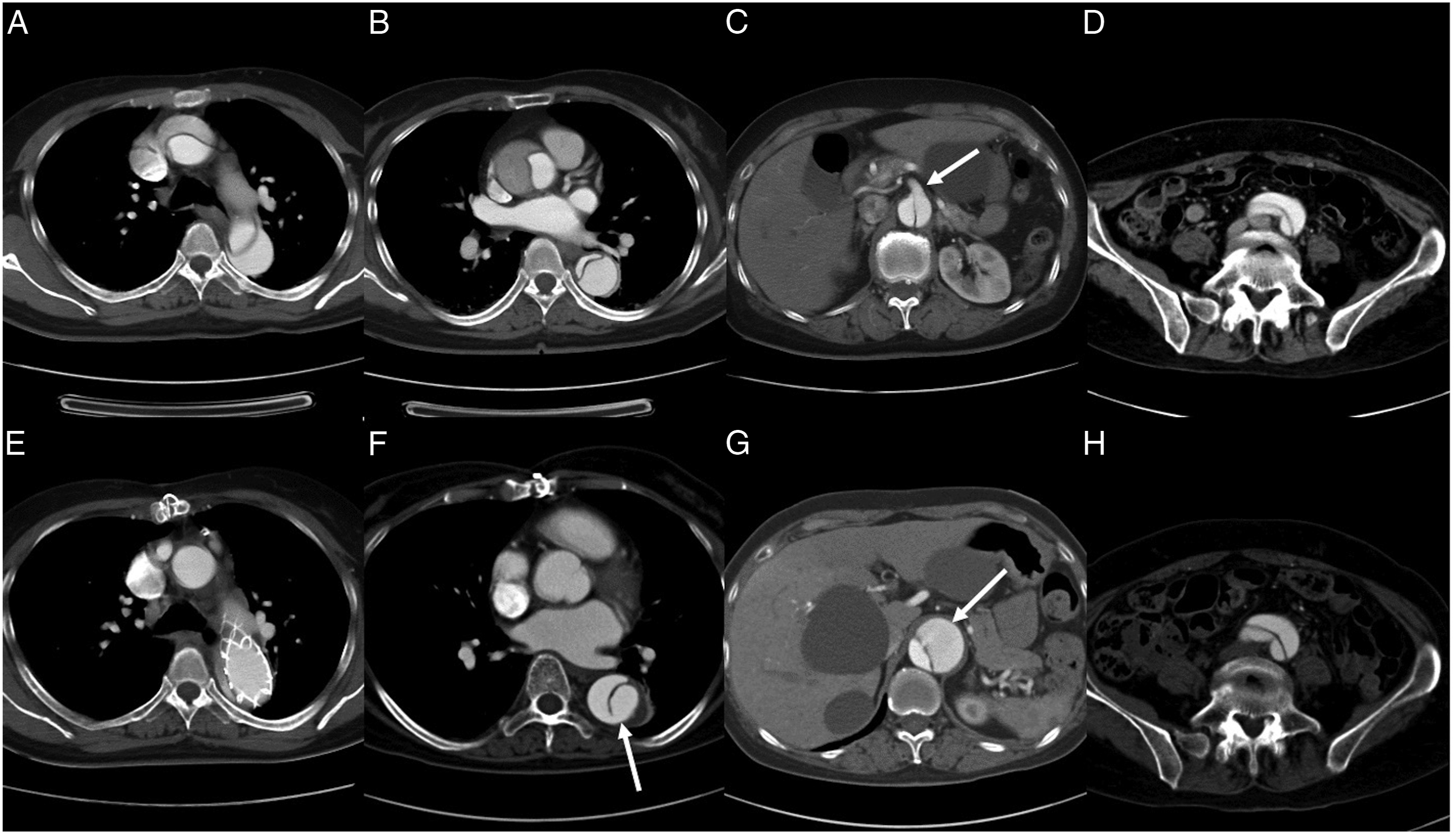
Discussion
Patency of the aortic false lumen has been reported to be a strong prognostic factor for aortic dissection.8,9 To promote thrombosis of aortic false lumens in cases of PDA, complete exclusion of the false lumen has been attempted using various methods. Fenestrated/branched devices have offered favorable outcomes3,4; however, the devices have been available in a limited number of countries. The candy plug technique is another option; however, it only excludes false lumens located in the thoracic aorta. 5 Closing all communicating channels between true and false lumens using aortic stent grafts, vascular plugs, and the use of bridging covered stents has been reported to be an alternative useful measure to achieve false lumen thrombosis in the abdominal aorta in countries where fenestrated/branched grafts are not available. 7 In the article, total complete false lumen thrombosis was obtained in 67% of the patients after the procedures. However, if arterial flow remains in the false lumen after closing all the channels, it is hard to resolve due to the difficulty in regaining access into the false lumen. In the present case, there was a residual flow in the false lumen at a visceral segment after closing all channels between true and false lumen. The possible communicating hole was thought to be either at the detached ostium of the left or right accessory renal artery. The location of the hole was not able to be identified, and therefore the hole was difficult to cannulate. Percutaneous direct puncture of the false lumen could be an option for approaching false lumens; however, bowel, ureter, and small vessels existing nearby puncture routes can be obstacles for this option. On the other hand, the penetration of the dissected membrane as is presented in this case is a simple, easy, and reliable measure to obtain access into the false lumen without risk of injuring the surrounding structures and organs. After embolizing the false lumen, the hole in the dissected membrane created by the needle and sheath insertion was easily closed by deploying a vascular plug. This method could be an access of choice in cases where other approaches are unfeasible.
Conclusions
An expanding aortic false lumen in a case of chronic aortic dissection, despite attempts to close communicating channels between the true and false lumen, was successfully managed by embolization of the aortic false lumen with coils and glue. Under the circumstances, direct penetration of the dissected membrane was a safe and useful measure to regain access to the aortic false lumen.
Footnotes
Authors’ Note
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.