
Abstract
Venous thromboembolism from a “thrombotic storm”–like syndrome is a major cause of morbidity and mortality in patients with active or “recovered” COVID-19. Patients should be risk-stratified, optimally by a pulmonary embolism (PE) response team (PERT), and considered for escalation of care if found with intermediate or high-risk PE. We present a series of patients with COVID-19-associated PE and thrombotic storm with D-dimer >10 000 ng/mL who underwent successful mechanical thrombectomy for intermediate to high-risk PE. All patients had immediate improvement in hemodynamics and large amounts of thrombi were retrieved.
Keywords
Venous thromboembolism from a “thrombotic storm”–like syndrome is a major cause of morbidity and mortality in patients with active or “recovered” COVID-19. 1 There are little data on the epidemiology, pathophysiology, management, or outcomes of pulmonary embolism (PE) associated with COVID-19. Chest computed tomography angiography (CTA) should be pursued in all COVID-19 patients with hemodynamic instability (tachycardia/hypotension), elevated serum troponin levels, or right heart strain on point-of-care echocardiography. Patients should be risk-stratified, optimally by a pulmonary embolism response team (PERT), and considered for escalation of care if found with intermediate or high-risk PE based on the simplified Pulmonary Embolism Severity Index (sPESI). 2 Mechanical thrombectomy using the large-bore FlowTriever catheter (Inari Medical, Irvine, CA) has emerged as a successful endovascular approach to aspirate thrombus from the pulmonary arteries (PAs) without requiring thrombolytic therapies.3,4 We present a series of patients with COVID-19-associated PE and thrombotic storm with D-dimer >10 000 ng/mL who underwent successful mechanical thrombectomy for intermediate to high-risk PE.
Patient 1. A 48-year-old morbidly obese man presented for sudden-onset dyspnea and palpitations. He was diagnosed with COVID-19 3 weeks prior. He initially required 2 L oxygen via nasal cannula to maintain oxygen saturation >90%. Serum troponin I was 0.07 ng/mL. sPESI score was 2. Chest CTA showed bilateral PE at the right main PA and at the left proximal lobar PAs extending into the left main PA, with a right ventricle to left ventricle (RV:LV) ratio of 1.5 (Figures 1A1–1A2). PERT team consensus was escalation with catheter-directed thrombectomy. Pulmonary angiography showed occluded right and left main PAs (Figures 1B1–1B2). Suction mechanical thrombectomy through a 24 F FlowTriever catheter led to successful flow restoration (Figures 1C1–1C2) and immediate PA systolic pressure improvement from 96 mmHg to 38 mmHg. “Lollipopping” of the thrombus from the left PA on the end of the catheter occurred (arrows), which was withdrawn to the ileo-femoral segment (Figure 1D1). A FlowTriever Disc was deployed in the suprarenal inferior vena cava with successful ileo-femoral clot aspiration utilizing the 24 F FlowTriever catheter (Figures 1E1–1E2). He had immediate symptom improvement, was weaned to room air, and was discharged home 2 days later. A1–A2, Chest CTA showing bilateral thrombi in the right main PA and the left proximal lobar PAs, with an RV:LV ratio of 1.5. B1–B2, Pulmonary angiography showed occluded right and left main PAs. C1–C2 Successful flow restoration after suction mechanical thrombectomy. D1, Thrombus “lollipopping” on the end of the catheter (arrow). E1–E2, Recovered thrombi. LV: left ventricle; PA: pulmonary artery; RV: right ventricle.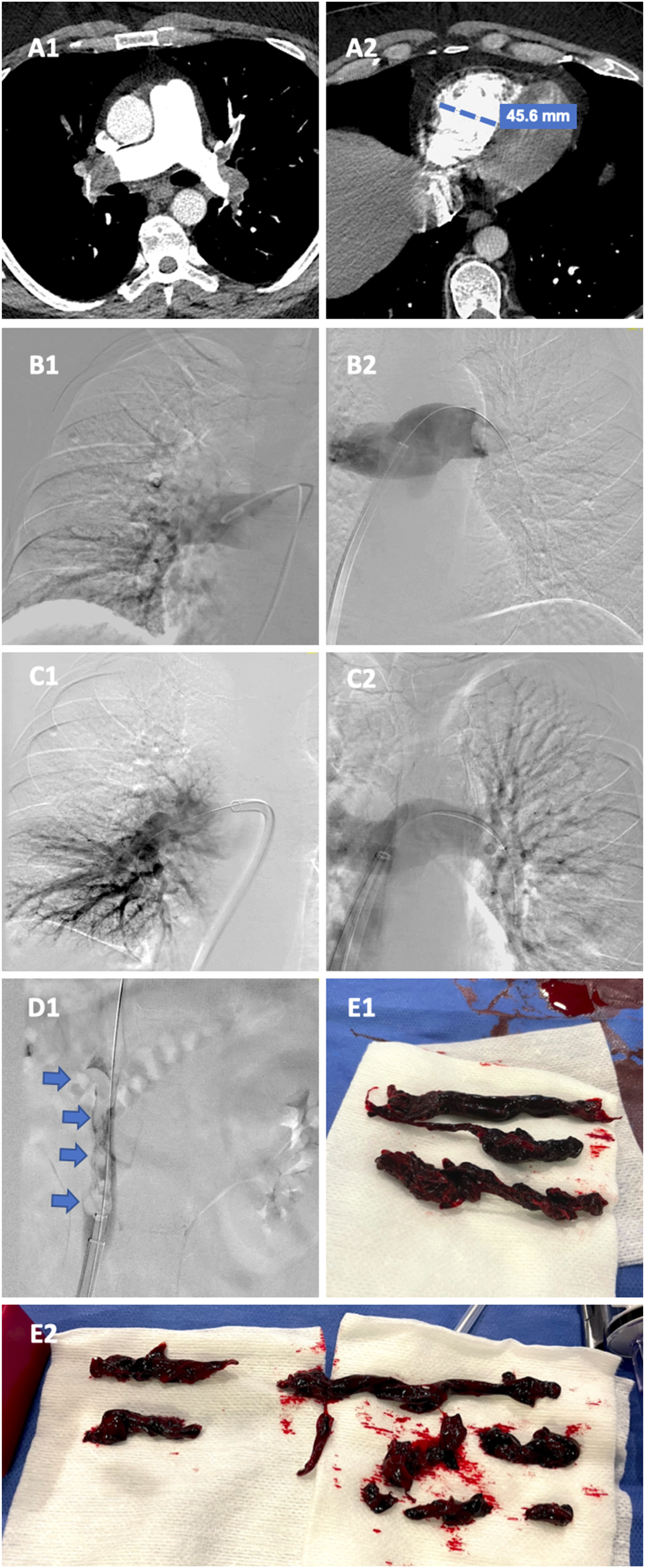
Patient 2. A 55-year-old morbidly obese woman presented for dyspnea. She was found COVID-19 positive. She was hypoxemic on admission with oxygen saturation as low as 83% on room air. Serum troponin I was 8.57 ng/mL. sPESI score was 3. Chest CTA showed saddle embolism; embolic involvement of all pulmonary lobes, with an RV:LV ratio of 2.1; flattening of the interventricular septum (IVS); and significant distension of the right cardiac chambers (Figures 2A1–2A2). PERT team consensus was escalation with catheter-directed thrombectomy. Pulmonary angiography showed occlusion of the right descending branch, near-occlusion of the left descending branch, and extensive PE in the right main, middle, and upper branches A1–A2, Chest CTA showing saddle embolism with an RV:LV ratio of 2.1. B1–B2, Pulmonary angiography showing occlusion of the right descending branch, near-occlusion of the left descending branch, and extensive thrombus in the right main, middle, and upper branches, and the left main and upper branches. C1–C2, Restoration of flow to the right lower and middle lobes, improved perfusion to the left lower lobe. D1, Recovered thrombi. CTA: computed tomography angiography; LV: left ventricle; RV: right ventricle.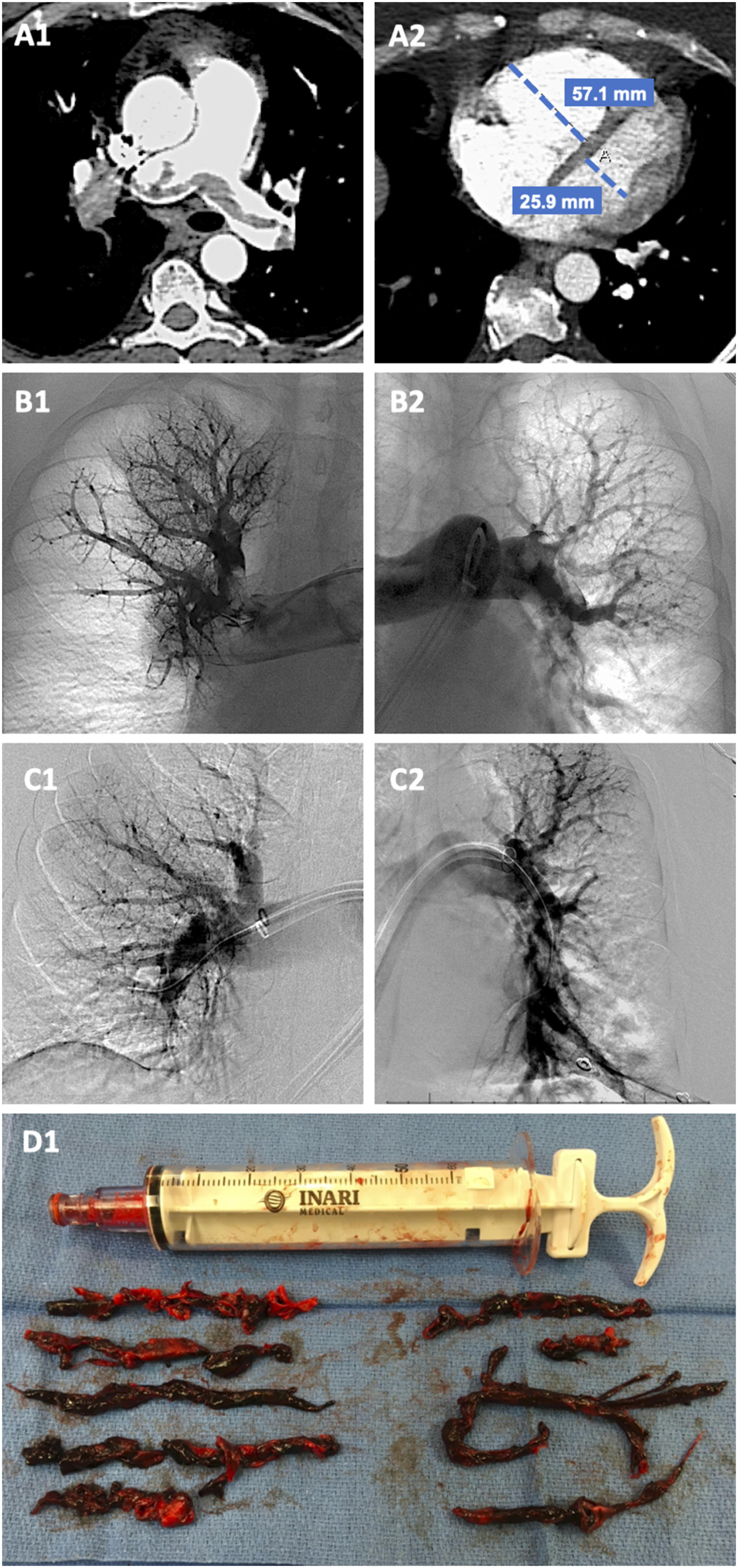
Patient 3. A 20-year-old woman athlete with a history of COVID-19 7 months prior presented for dyspnea. Her vitals, including oxygen saturation, were normal on admission. She never required hospitalization for COVID-19 and had not received treatment with glucocorticoids or anticoagulation. Serum troponin was negative. sPESI score was 1. Chest CTA showed multiple large PE in the bilateral PAs extending into the segmental and subsegmental branches, with an RV:LV ratio 1, and flattening of IVS (Figures 3A1–3A2). PERT team recommendation was to pursue thrombectomy. Pulmonary angiography was consistent with the CTA findings (Figures 3B1–3B2). A 24 F FlowTriever catheter was used for repeated suction thrombectomy, with interval resolution of thrombus burden, improved perfusion to both lungs (Figures 3C1–3C2), improvement in PA systolic pressure from 18 mmHg to 15 mmHg, and a large amount of mixed acute and chronic clot retrieved (Figure 3D1). She was discharged home 2 days after the intervention. A1–A2, Chest CTA showing multiple large thrombi in the bilateral PAs extending into the segmental and subsegmental branches, RV:LV ratio 1. B1–B2, Pulmonary angiography consistent with CTA findings. C1–C2, Improved perfusion to both lungs following suction mechanical thrombectomy. D1, Recovered thrombi. CTA: computed tomography angiography; LV:left ventricle; PA: pulmonary artery; RV: right ventricle.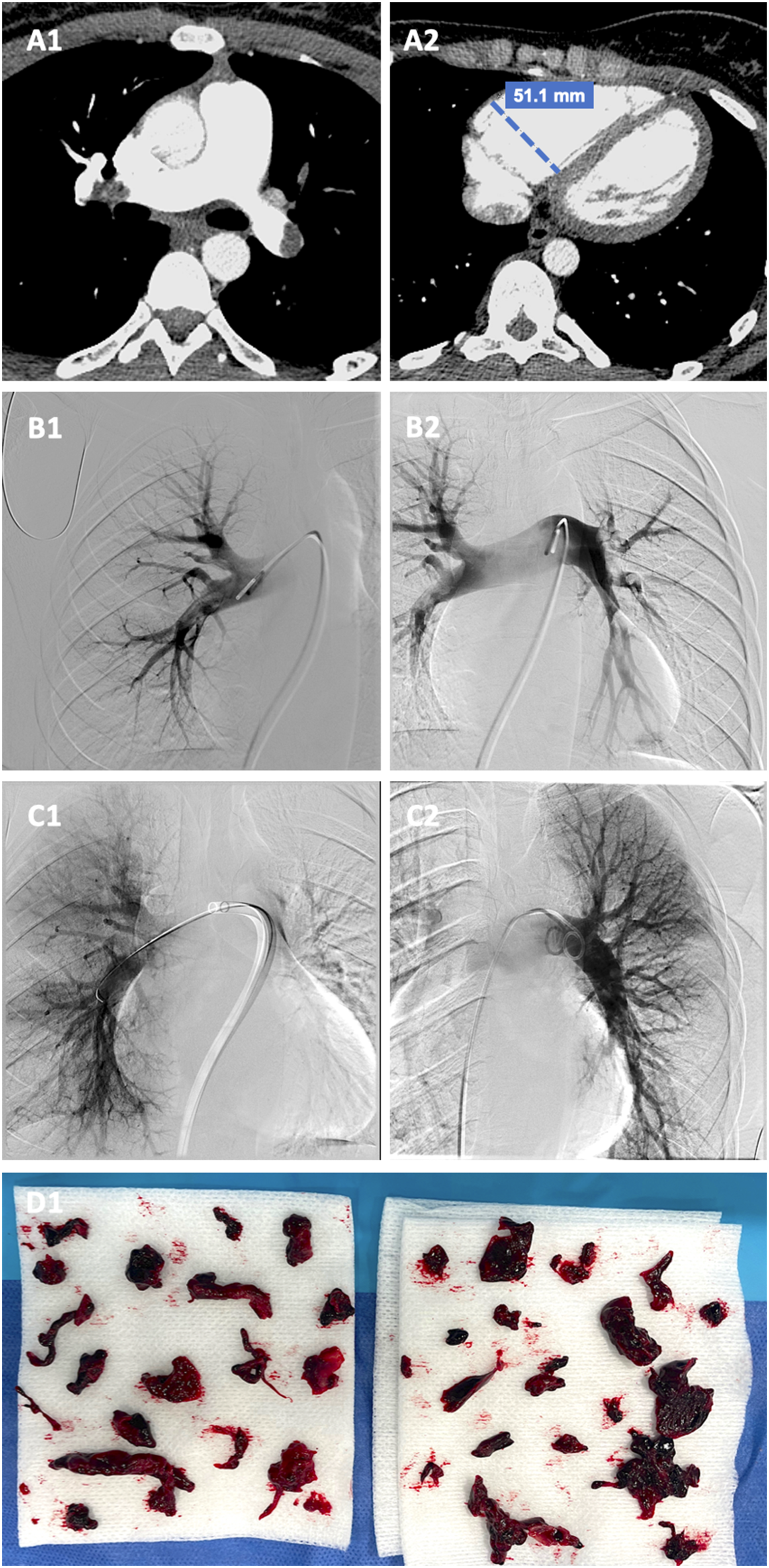
Patient 4. A 77-year-old man presented for dyspnea worsening for the past 2 days. He was diagnosed with COVID-19 3 weeks prior, but his dyspnea was different compared to his previous presentation. Serum troponin I was 0.8 ng/mL. sPESI score was 4. Chest CTA showed extensive bilateral PE with near-occlusion of the distal left main PA, distal right main PA thrombus (arrows), and an RV:LV ratio of 2.9 (Figures 4A1–4A3). PERT team consensus was escalation with catheter-directed thrombectomy. Pulmonary angiography showed saddle embolus with near-complete occlusion of the distal left main PA (Figure 4B1), distal right main PA thrombus, and filling defects extending into bilateral lobar, segmental, and subsegmental branches of all lobes. A 24 F FlowTriever catheter was advanced. Three rounds of suction mechanical thrombectomy were performed, leading to minimal residual thrombus burden (Figures 4C1–4C2), immediate improvement in PA systolic pressure from 44 mmHg to 30 mmHg, and significant thrombus retrieved (Figure 4D1). He was transferred to a regular medical floor 3 days after the procedure and discharged home 2 days after the transfer. A1–A3, Chest CTA showing extensive bilateral thrombi with near-occlusion of the distal left main PA, distal right main PA thrombus (arrows), and an RV:LV ratio of 2.9. B1, Pulmonary angiography showing addle embolus with near-complete occlusion of the distal left main PA. C1–C2, Minimal residual thrombus burden after suctioning mechanical thrombectomy. D1, Retrieved thrombus. CTA: computed tomography angiography; LV: left ventricle; PA: pulmonary artery; RV: right ventricle.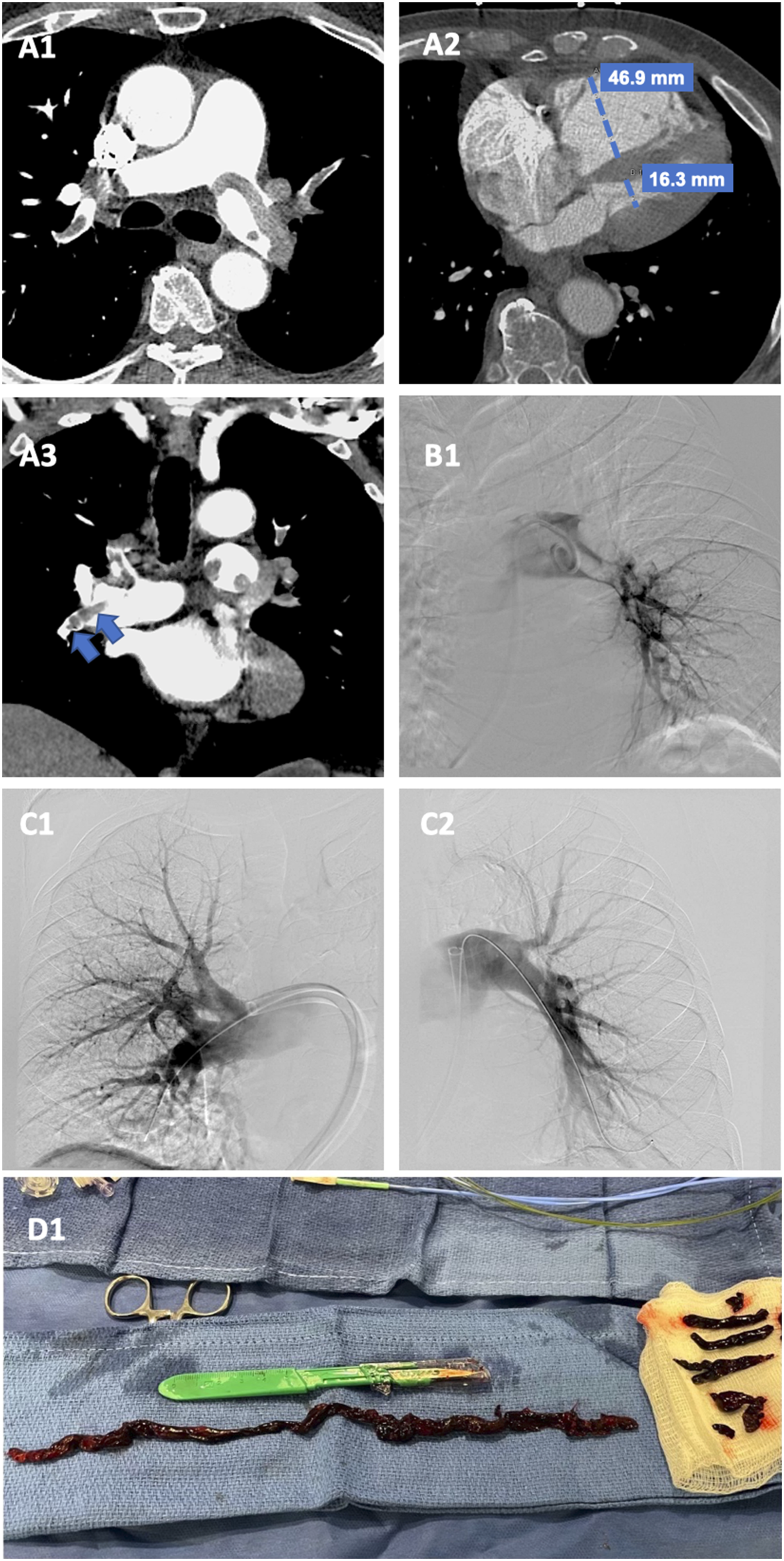
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent has been obtained from the patients for publication of the cases and accompanying images.