
Abstract
Background
Renal cell carcinoma (RCC) with tumor thrombus (TT) may extend into and, in rare cases, actually invade the inferior vena cava (IVC). Techniques of IVC reconstruction after removal of the RCC, TT, and infiltrated portion of the IVC have not been well documented.
Introduction
Renal cell carcinoma (RCC) is the most common malignant tumor of the kidney. Over 73,750 new cases were diagnosed in 2020. 1 RCC has a myriad of presentations, and although infrequently encountered, it may extend by a tumor thrombus (TT) into the inferior vena cava (IVC) and right atrium.2-6 The TT inside the IVC can be very bulky and may directly invade the IVC, requiring dissection and/or grafting of the IVC. The surgical approach has evolved as techniques2-6 and prosthetics have been refined.7-9
We report our experience of RCC with a TT directly infiltrating the wall of the IVC. Replacement of the affected portion of the IVC with a ringed polytetrafluoroethylene (PTFE) interposition graft was necessary in 4 patients with partial obstruction of the IVC. The novel aspect in using this technique was the introduction of an IVC filter inside the PTFE after performing anastomosis of the PTFE to the proximal IVC and corresponding (right or left) renal vein but before performing anastomosis to the distal portions of the IVC. The IVC filter was placed below the anastomosis of the corresponding (right or left) renal vein.
Material and Methods
This study was performed after obtaining Institutional Review Board approval of the University of Miami Miller School of Medicine (# 20200791) and following the ethical principles of the Helsinki Declaration (as revised in 2013). A written informed consent was obtained from the participants in this study. A retrospective chart review was performed on 4 patients at our institution who underwent surgical treatment for large, aggressive, locally advanced RCC with direct TT infiltration of the IVC wall. None of the patients had significant lower extremity edema. Abdominal computed tomography and/or magnetic resonance imaging were used to diagnose the renal tumor, delineate the TT inside the IVC, and depict the extent of invasion of the IVC. Cardiac, renal, and respiratory status were evaluated pre-operatively. Cranial extent of the TT into the IVC was defined as Level II, III, or IV by a previous classification. 10 However, 2 patients had level IIIa (retrohepatic) and level IIIC (suprahepatic, infradiaphragmatic) TT according to our further subclassification. 11 For pathological staging, the 2009-TNM classification was used. Tumor grade was classified according to the Furhman grading system. Informed consent was given, including the complexity of the surgery, risks associated with handling and removal of the TT, the possibility of TT pulmonary emboli occurring during IVC manipulation, and the possibility of IVC reconstrucution being required (along with placement of an IVC filter). Intermittent pneumatic compression device, early ambulation, and subcutaneous heparin (5000 U twice/day) started 72 hours after surgery were used as prophylaxis for post-operative venous thromboembolism. Before going home, patients were started on aspirin 325 mg daily.
Intraoperative transesophageal echocardiography (TEE) was used to delineate and monitor the cranieal extent of the TT during the surgical procedure. All relevant data on demographics, surgical details, pathology characteristics, postoperative complications, and major clinical outcomes were collected and analyzed.
Surgical Technique
The organ transplant–based approach that we use includes piggy-back liver mobilization and en bloc mobilization of the spleen and pancreas which facilitates the resection of right or left large renal tumors; these techniques have been previously described.2-6
Briefly, a modified chevron incision was used, commencing approximately 2 fingerbreadths below the right or left costal margin and extending out laterally to the mid-axillary line. Exposure was gained via the use of a Thompson retractor. Exposure of the left kidney began by mobilization of the descending colon. A left-sided tumor required that the spleen was dissected off the diaphragm and mobilized en bloc with the pancreas toward the midline. This exposes the entire upper retroperitoneal space from the diaphragm to the inferior border of the kidney. The right or left kidney was mobilized laterally and posteriorly, and the perirenal collateral circulation was ligated. The collateral circulation collapsed, making the remaining dissection easier to perform. The renal artery was identified, ligated, and divided posteriorly after a midline rotation of the kidney with the tumor. 12
To access the retrohepatic IVC, the liver was completely mobilized off the IVC using an organ transplant–based approach, with the only remaining structural attachments being the hepatic veins and porta hepatis (piggyback liver mobilization).2-6 Furthermore, a plane was created between the IVC and posterior abdominal wall
Of note, the patient with RCC and level II TT did not require such an extensive liver mobilization. The IVC was dissected enough to place vascular clamps at the levels of the proximal and distal IVC and at the level of the left renal vein. The vascular clamps were placed to include normal IVC for the vascular reconstruction.
For the patient with a level IIIa retrohepatic TT, the liver was fully dissected off the IVC and the small hepatic veins were ligated as described.2-6 It was sufficient to allow removal of the TT.
For the patient with a level IIIc TT (suprahepatic, infradiaphragmatic), due to extension of the TT into the diaphragm, the central diaphragm tendon was dissected to the supra-diaphragmatic area, and the intra-pericardial IVC was identified. The dissection was circumferential so that the intra-pericardial IVC could be identified.
Use of intraoperative TEE was critical to delineate the cranial extent and mobility of the TT during dissection of either the retrohepatic or supra-diaphragmatic IVC. In addition, its use ensured that there were no pulmonary artery emboli or TT extending into the right atrium. In addition, the intraoperative TEE guided us during application of the supra-diaphragmatic IVC vascular clamp, ensuring that the clamp excluded TT.
For the patient with level IIIa TT, vascular clamps were placed in the infra-renal IVC followed by the left renal vein and below the major hepatic veins (MHVs) without the need of a Pringle maneuver.
The level IIIc TT of the third patient could not be “milked” downward out of the suprahepatic IVC, as this patient’s TT was bulky and not freely mobile. In this case, a Pringle maneuver was performed to temporarily occlude blood inflow to the liver. Vascular clamps were placed in the infra-renal vena cava, followed by the right renal and adrenal veins, and a Satinsky clamp was placed across the supra-diaphragmatic IVC (under TEE monitoring). The IVC was incised from the MHVs to the renal vein, and the TT was removed. In some areas, the TT was dissected sharply off the IVC wall. The 3 MHVs were visualized, and their orifices were inspected. Following removal of TT and closure of the upper cava, the vascular clamp was repositioned below the hepatic veins. The Pringle maneuver was discontinued, and blood flow to the liver was re-established. Clamping below the MHVs generally allows for a timewise short Pringle maneuver.
Regarding the fourth patient, the TT inside the right atrium was bulky and could not be milked downward. He required cardiopulmonary bypass (CPB). 13 After CPB was initiated, the right atrium was opened and the TT was removed as described before. 13 During the CBP, a Pringle maneuver was infra-renal vena cava, followed by the left renal vein. Once the opening of the right atrium was sutured and CPB removed, the rest of the procedure was similar as described for the third patient with level IIIc TT.
Following removal of the level IIIc and IV TTs and closure of the upper cava, the vascular clamp was repositioned below the MHVs. The remaining IVC below the MHVs was removed in both cases due to the infiltration/invasion of its wall at multiple sites (Figure 1A). (A) Resected inferior vena cava (IVC) with adherent tumor thrombus (white arrow), (B) drawing showing the deployed IVC filter inside the ringed PTFE graft (black arrow), (C) intraoperative ringed PTFE graft anastomosed to the proximal (P) and distal (D) IVC and left renal vein (LRV), (D) Coronal computed tomography scan demonstrating open-ringed PTFE graft (dotted white arrow) with IVC filter (white arrow) 2 years after en bloc resection of renal cell carcinoma with tumor thrombus and IVC.
The IVC was replaced with a vascular conduit of ringed PTFE graft. The PTFE graft was anastomosed to the proximal IVC with 4-0 Prolene and to the left or right renal vein with 5-0 Prolene. Then, a vascular clamp was placed below the right or left renal vein, and the rest of vascular clamps were released. A Trapease® permanent IVC filter was deployed inside the ringed PTFE graft before finishing the distal anastomosis with 4-0 Prolene (Figure 1B). Three patients had the left renal vein anastomosed to the PTFE graft (Figure 1C), and the third patient with left RCC and level IIIc TT, a patch of tumor-free IVC with right adrenal and renal veins, was anastomosed to the ringed PTFE graft.
For each patient, at the end of surgery, a TEE was re-performed to rule out any pulmonary artery emboli or piece of TT being left behind.
Results
Main Characteristics of the Patients.
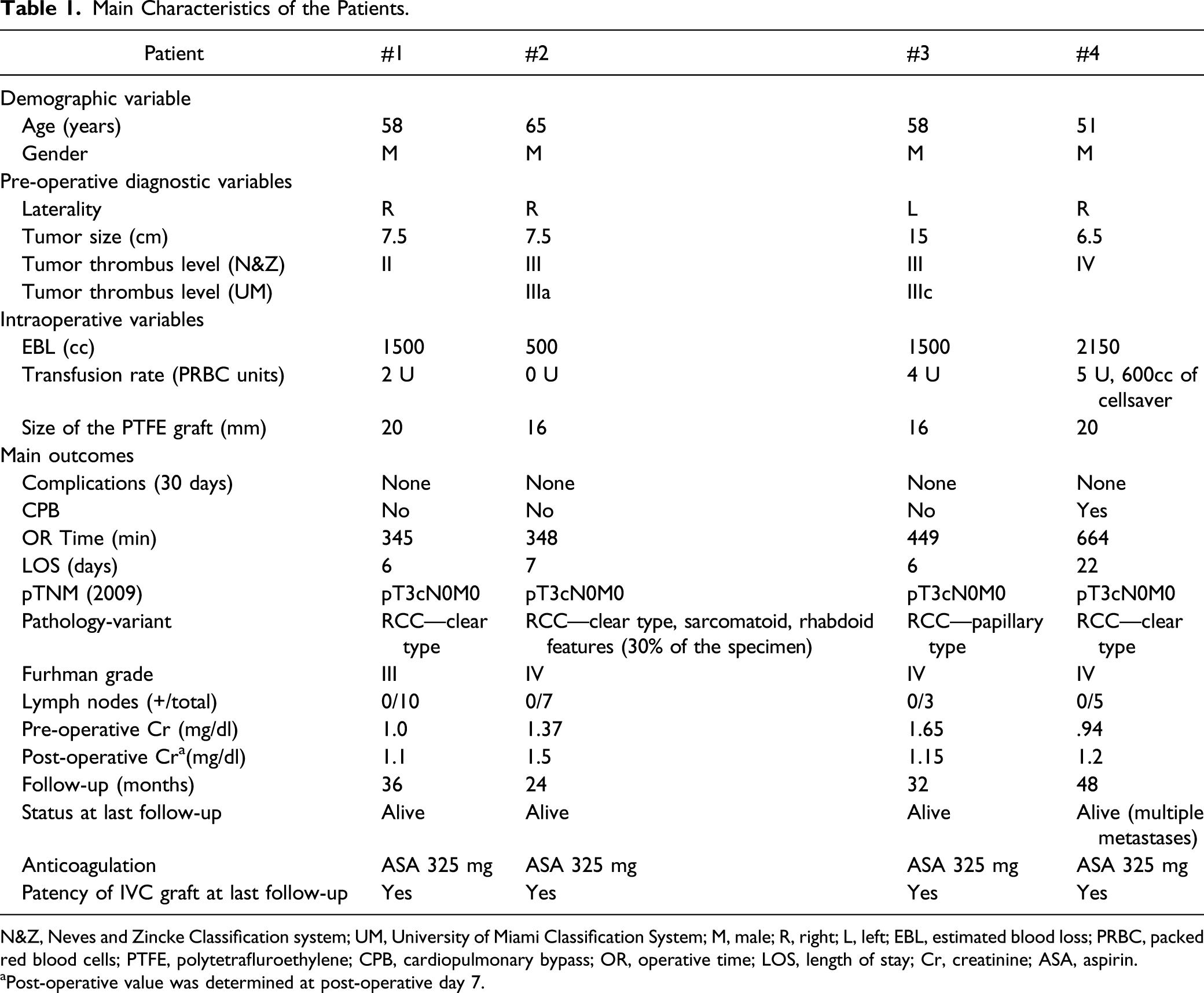
N&Z, Neves and Zincke Classification system; UM, University of Miami Classification System; M, male; R, right; L, left; EBL, estimated blood loss; PRBC, packed red blood cells; PTFE, polytetrafluroethylene; CPB, cardiopulmonary bypass; OR, operative time; LOS, length of stay; Cr, creatinine; ASA, aspirin.
aPost-operative value was determined at post-operative day 7.
The post-operative courses for each of the 4 patients were uneventful.
None of the patients presented with distant metastasis (all were M0), and none of the patients had positive lymph nodes (all were N0). For patients #1, #2, and #4, the RCC was clear cell type; patient #3 had a papillary cell type. Length of hospital stay (LOS) was 6, 7, and 6 days for patients #1–#3, respectively, and 22 days for patient #4. Each patient was discharged with stable renal function (Table 1). Post-surgical follow-up for the 4 patients have been through 36, 24, 32, and 48 months, respectively. The ringed PTFE graft with the IVC filter remained patent throughout each patient’s follow-up period and without any evidence of disease recurrence at the IVC resection site (Figure 1.D). None of the patients experienced a post-operative pulmonary embolic event. Overall survival at 2 years following surgery was 100%. At last follow-up, the fourth patient was being followed by oncology due to the development of multiple bone metastasis; the other 3 patients remained disease-free at last follow-up.
Discussion
RCC with TT extension into the IVC, and sometimes even into the right atrium, continues to be a technically challenging and complex urological surgery to perform successfully.2-7 One of the more stressful surgical problems occurs when the IVC is partially or completely obstructed by the TT. The TT may directly invade the wall of the IVC, and it is almost impossible to determine before surgery whether the TT has invaded the IVC wall. During surgery, the IVC should be carefully inspected to determine where and to what extent the infiltration/invasion by the TT has occurred. In certain circumstances, the TT, while bulky, is not attached to the wall of the IVC, and the IVC can be surgically resected and repaired where needed; otherwise, its continuity can be restored with the use of a synthetic or homologous venous graft.7-9,14
Here, we reported our experience in surgically removing RCC with TT that has directly infiltrated the IVC. The most important aspect of this report is the reconstruction of the IVC with a ringed PTFE graft and an IVC filter inserted into the tubal graft before the vascular anastomoses to the remnant distal IVC was performed. The IVC filter was used in these 4 patients because of the possibility of an existing distal bland thrombus, which could not be determined before or during the surgery. 15 The concept of including an IVC filter has not been previously described in the literature for surgical resection of RCC with TT. The interposition grafts remained patent throughout each patient’s follow-up period, and there was no evidence of disease recurrence at the surgical resection site. None of the patients had a post-operative pulmonary embolic event.
In all 4 patients, abdominal computed tomography and/or magnetic resonance imaging did not show chronic IVC obstruction, but in each case, there was a possibility that IVC infiltration had occurred. After performing an en bloc radical nephrectomy, tumor thrombectomy, and IVC resection, PTFE grafting was necessary in the absence (or poor development) of collateral circulation. The PTFE graft is a synthetic material which is often used as IVC replacement.7-9 The ringed PTFE graft has a low thrombogenic potential and a comfortable patency rate for low flow vessels like the IVC.8,9,14
In 1998, Sarkar et al. reported that only 1 of 10 patients with a prosthetic IVC replacement had graft thrombosis at a mean follow-up of 19 months. 16 Caso et al reported their outcomes in 5 asymptomatic patients with incomplete IVC obstruction who underwent reconstruction of the IVC with PTFE (4 cases) and Dacron (1 case) grafts for different urologic malignancies. Only one of these 5 patients had RCC with TT, and reconstruction of the IVC was performed with the Dacron graft which subsequently occluded at 9 months of follow-up. 14 Recently, Benkirane et al reported that graft thrombosis developed in 5 out of 26 (19.2%) RCC patients with caval thrombus during the first year of follow-up. Patency of the IVC graft at 6 and 12 months was 88% and 79%, respectively. 8
We described in our early experience the routine use of a PTFE interposition graft to replace the IVC gap after extensive surgical resection. 15 It was subsequently observed that patients with complete IVC obstruction caused by the TT did not necessarily need IVC replacement, as most of such patients did not have preoperative lower extremity edema (indicating that sufficient collateral circulation had already developed). Those patients tolerated total IVC interruption or removal.15,17,18
Conclusions
To conclude, when RCC included direct IVC infiltration by the TT, the IVC can be replaced by a ringed PTFE and the novelty of this approach is that an IVC filter can be deployed before completing the distal IVC anastomosis. None of the patients experienced a post-operative pulmonary emboli event, and the PTFE graft in each patient was patent at last follow-up. Nevertheless, there are 2 questions still to be answered when dealing with RCC extending into the IVC and the TT invading/infiltrating the IVC wall. First, does resection of the IVC invaded by TT increase cancer-specific survival? That is, by removing the cava, will the probability of a local recurrence developing at the IVC resection site be reduced? 19 Second, when primarily removing the TT from the IVC without IVC resection or replacement and leaving behind areas of severe endothelial damage, is it sufficient to reasonably conclude that a negative surgical margin has been achieved?
Footnotes
Author Contributions
Gaetano Ciancio: Conceptualization, methodology, investigation, writing—original draft, visualization, supervision, and formal analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.