
Abstract
Background
Middle aortic syndrome is a rare disease. Several surgical treatments are available; however, the optimal treatment strategy and long-term outcomes remain unelucidated. We herein report the 5-year outcomes of six patients treated with extra-anatomical bypass surgery for middle aortic syndrome.
Case presentations
Between 2013 and 2016, six patients underwent extra-anatomical bypass for middle aortic syndrome at our institute: three had Takayasu’s arteritis, one had vessel vasculitis, and two had middle aortic hypoplastic syndrome of unknown origin. The patients included five women and one man, with a mean age of 59.7 years. Four patients had uncontrolled hypertension and were receiving antihypertensive medications. The mean ankle–brachial pressure index was .61. The three patients with Takayasu’s arteritis were hospitalized for congestive heart failure. These patients underwent bypass surgery from the descending aorta to the infrarenal abdominal aorta, and one also underwent concomitant heart surgery. The patient with microscopic polyangiitis underwent Y-grafting with an aortic aneurysmectomy. Subsequently, bypass surgery was performed from the descending aorta to the graft via the diaphragm. The two patients with unknown causes underwent bypass surgery from the proximal descending aorta to the distal descending thoracic aorta. There were no early or late deaths at the 5-year follow-up. We did not observe any changes in anastomotic site stenosis or new aneurysmal changes during the follow-up period. The number of antihypertensive medications was reduced in all cases, and critical symptoms, including headache, severe abdominal pain, claudication, and heart failure, improved in all patients. The ankle–brachial pressure index increased to 1.11 and did not change for five years. Renal function remained stable, and the brain natriuretic peptide level decreased from 302.8 to 74.5 pg/mL at follow-up.
Conclusion
Extra-anatomical bypass for middle aortic syndrome is safe and effective, and can help prevent renal failure, and relieve critical ischemic symptoms.
Introduction
Congenital coarctation of the aortic arch is generally well known, and the Centers for Disease Control and Prevention estimated that about 4 of every 10 000 babies born in the United States had coarctation of the aorta. However, the number of patients with Takayasu’s arteritis (TA) was small, and the Japan Intractable Diseases Information Center reported that the number of registered patients in Japan was approximately 5000, and the number of new cases was approximately 100 per year. Additionally, 2731 additional cases of newly diagnosed TA were collected from the Korean National Health Insurance Service from 2006 through 2017. Among patients with TA, lesions from the descending thoracic aorta to the abdominal aorta are sporadic. Coarctation in the descending aorta, abdominal aorta, or both is called middle aortic syndrome (MAS) or mid-aortic dysplastic syndrome. The most common cause of MAS in Japan is Takayasu’s disease or TA,1,2 and MAS is also caused by congenital developmental anomalies, inflammatory aortitis, neurofibromatosis, and Williams syndrome.3,4 Patients with MAS often develop symptoms at a young age and require treatment; however, the onset of MAS in adulthood is rare.
MAS caused by TA commonly contributes to secondary hypertension due to coarctation of the aorta, renal artery stenosis, increased systemic resistance, and arterial insufficiency in the lower extremities. The clinical symptoms include uncontrolled hypertension, lower-extremity claudication, and ischemic abdominal pain. 5 Intermittent abdominal pain due to intestinal viscera ischemia and congestive heart failure due to afterload are similarly observed.
Several surgical treatments are available for MAS. The patient’s general condition and age, the aorta’s anatomy and pathological changes, and any history of surgical intervention in the peripheral arteries should be considered when determining the optimal surgical method. Although the use of endovascular treatments, such as stenting, has recently been reported,6,7 the long-term results are unknown due to prolonged inflammation in the aorta and substantial fibrotic changes, which make the procedure complicated and challenging. 8 Therefore, the optimal treatment strategy for MAS is yet to be determined.
We performed extra-anatomical bypass surgery in six adult patients who were diagnosed with MAS. We herein report the blood pressure control, improvement in organ perfusion based on clinical symptoms, and 5-year outcomes in these patients.
Case Presentations
Patients and Data Collection
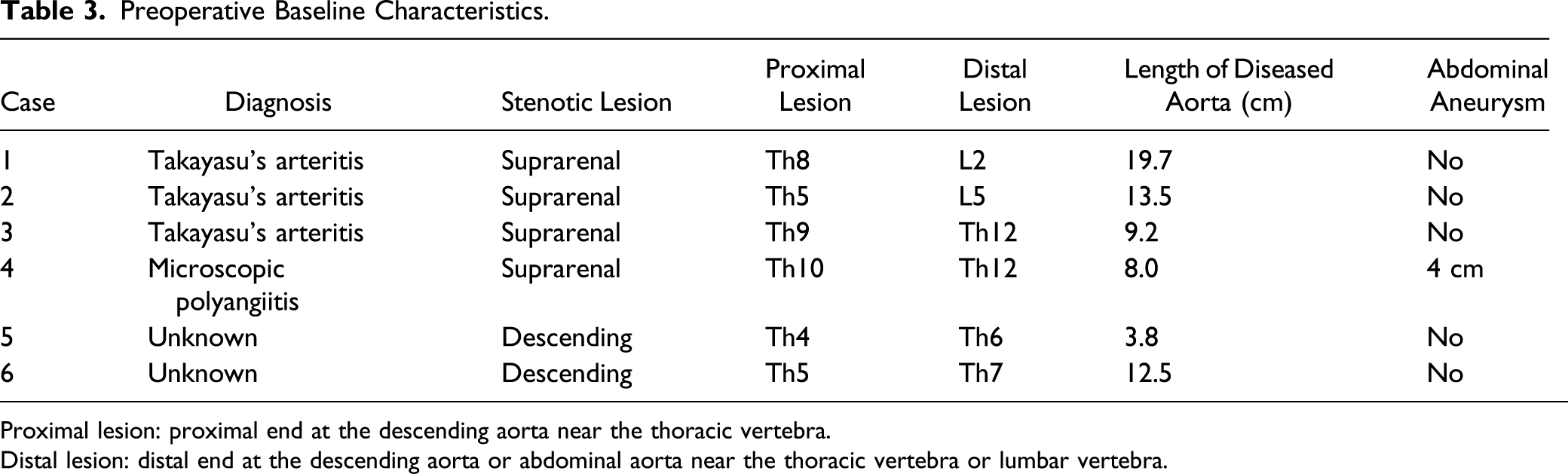
Preoperative Baseline Characteristics.
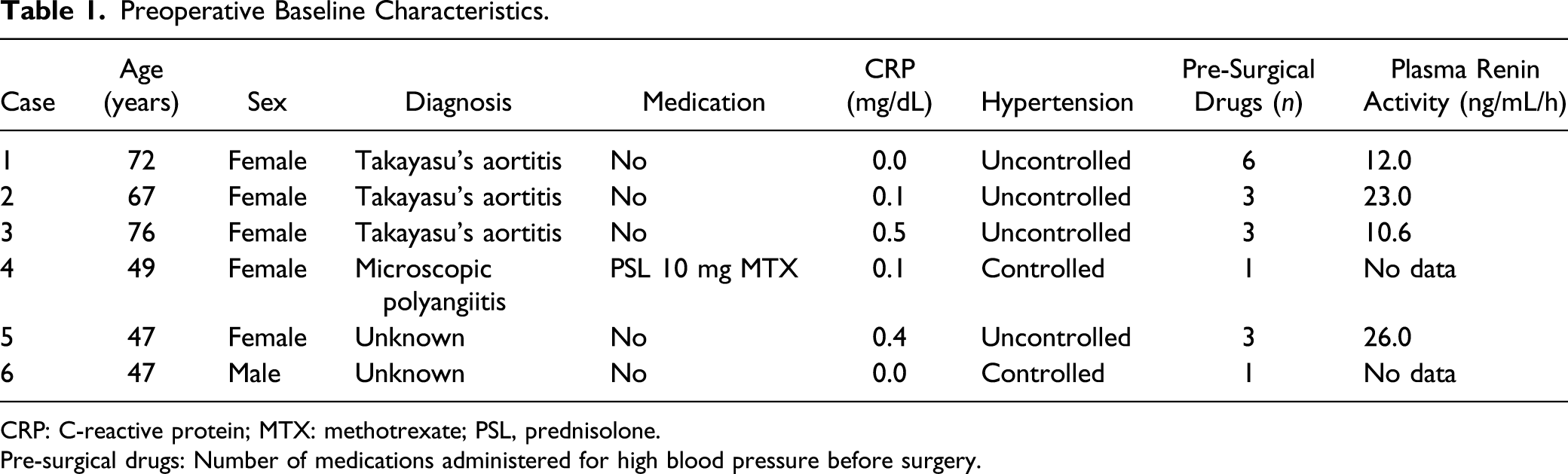
CRP: C-reactive protein; MTX: methotrexate; PSL, prednisolone.
Pre-surgical drugs: Number of medications administered for high blood pressure before surgery.
Preoperative Baseline Characteristics.
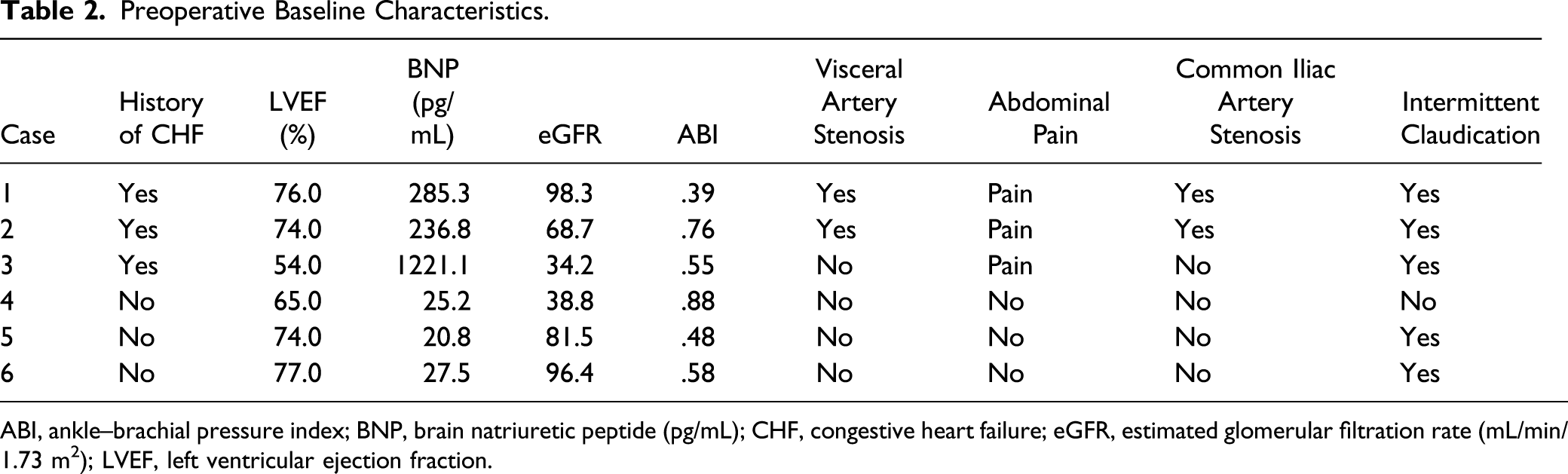
ABI, ankle–brachial pressure index; BNP, brain natriuretic peptide (pg/mL); CHF, congestive heart failure; eGFR, estimated glomerular filtration rate (mL/min/1.73 m2); LVEF, left ventricular ejection fraction.
This study was approved by the Clinical Ethics Committee of Juntendo University Hospital and was conducted in accordance with the principles outlined in the Helsinki Declaration. The IRB approval date and number are September 9, 2020, and JHS20-015. Written informed consent was obtained from each patient for publication of this case series.
Patient Characteristics
We investigated five female patients and one male patient. The patients’ average age at the time of surgery was 59.7 (range, 47-76) years. All six patients, including two with an undetermined cause, were deemed likely to have inflammatory vasculitis and were diagnosed with MAS. Similarly, three patients were diagnosed with TA according to the American College of Rheumatology diagnostic criteria (patients 1–3 in Table 1). Additionally, one patient was receiving steroids and immunosuppressants for vasculitis (patient 4 in Table 1). All patients exhibited disease progression with clinical symptoms, including heart failure, bilateral leg claudication, and intermittent abdominal pain. The mean preoperative C-reactive protein level was .13 (range, .00–.41) mg/dL. Uncontrolled hypertension was the primary clinical symptom in 4 patients, followed by a history of congestive heart failure in the three patients with TA (Tables 1 and 2). We defined hypertension that was maintained at > 140/90 mmHg at home, even with the use of three or more different classes of antihypertensive agents, as uncontrolled hypertension. The three drugs were defined as (1) a calcium antagonist, (2) an angiotensin-converting enzyme (ACE) inhibitor and angiotensin receptor blocker (ARB), and (3) a diuretic. Preoperative plasma renin activity was elevated in 4 patients (patients 1, 2, 3, and 5) (Table 1). Renal dysfunction was not observed in any patients. The mean ankle–brachial pressure index (ABI) was .61, with intermittent abdominal pain in two patients and intermittent claudication in 4 patients’ bilateral legs (Table 2).
Preoperative Imaging
All patients underwent preoperative imaging of the aorta and aortic branches, including the celiac axis, superior mesenteric artery, inferior mesenteric artery, and renal artery. All patients in this study underwent multi-slice thin-section computed tomography angiography.
Anatomical Characteristics
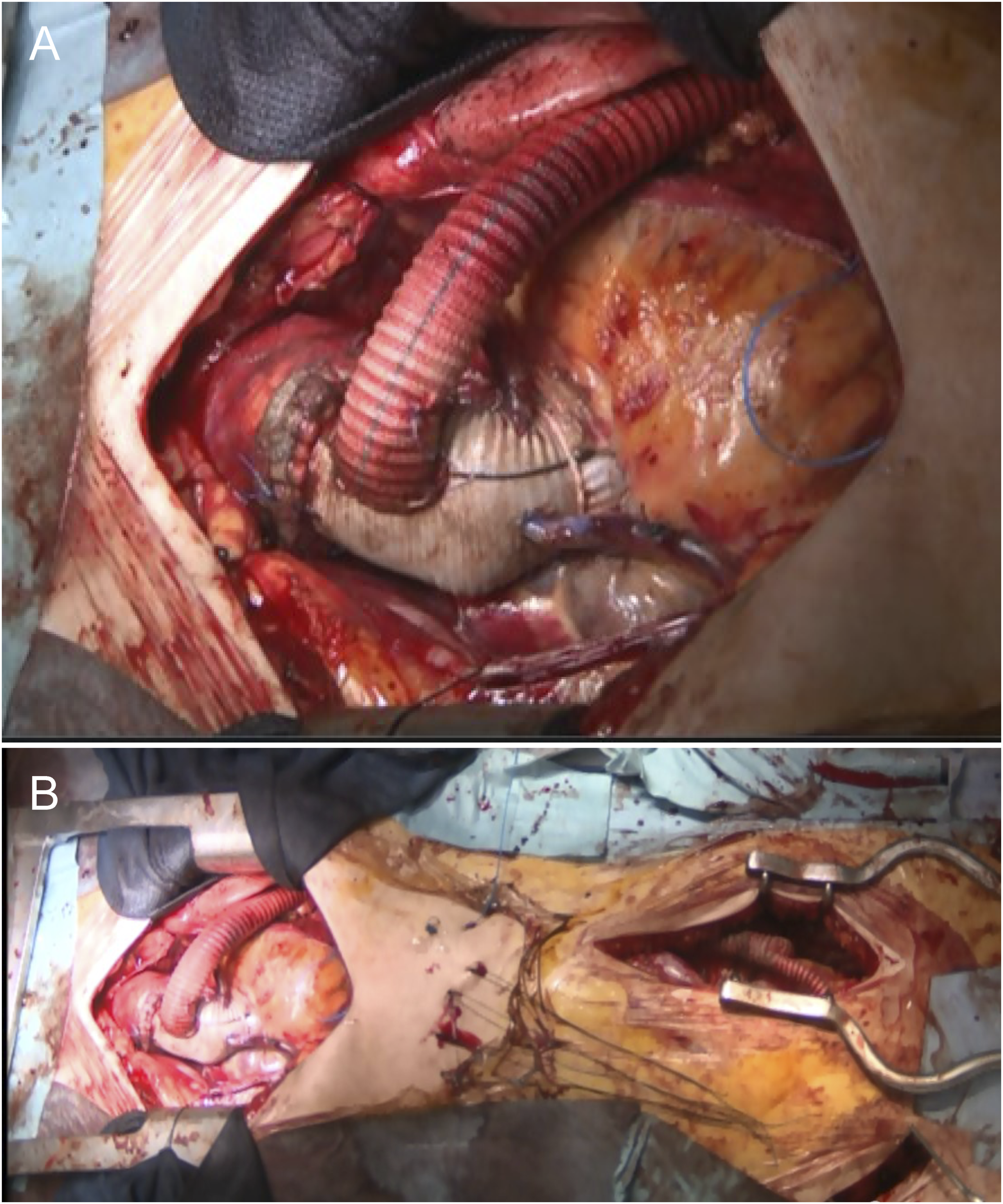
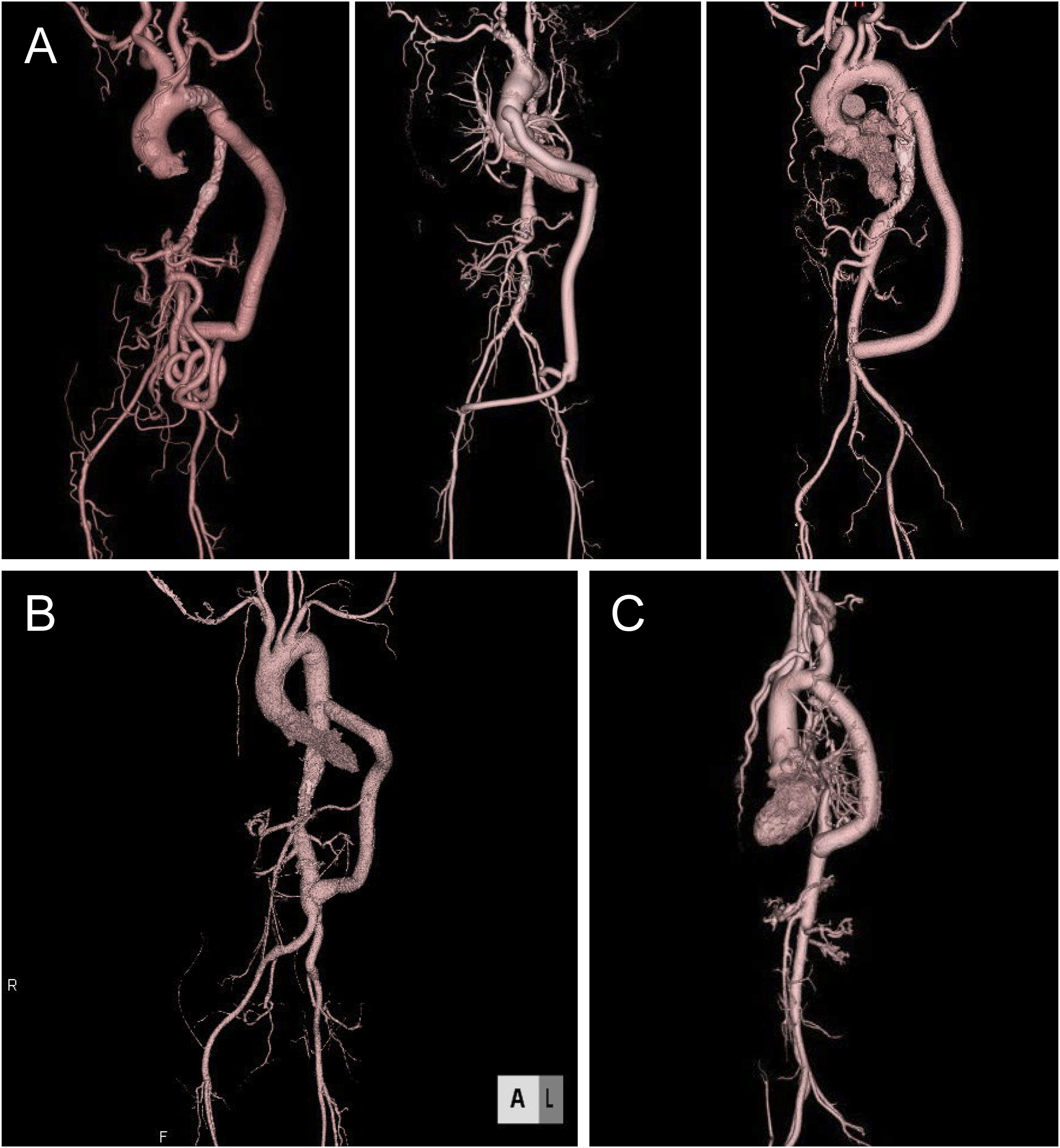
The aortic stenotic lesions in the two patients with TA were complex and extensive, extending from the descending aorta to the abdominal aorta, and the common iliac artery was also narrow. In Case 2, the left subclavian artery was also occluded for the entire length, and the sinus of Valsalva was dilated. In Case 3 of TA, the lesion extended to the abdominal aorta from the distal descending aorta to the branch of the celiac artery. In microscopic polyangiitis (patient 4), there was stenosis from the upper part of the abdominal aorta to above the renal artery, and post-stenotic dilatation was observed below the renal artery. In Cases 5 and 6, the stenosis was mainly located in the central part of the descending aorta (Figures 1–3). The mean length of the diseased aorta was 13.1 cm (Table 3). Regarding aortic branch disease, celiac axis stenosis was observed in two patients, and severe calcification of the bilateral common iliac arteries was observed in two other patients (Figures 1–3). Preoperative imaging findings. (A) Takayasu’s arteritis. Case 1: Extensively diseased section of the aorta (descending aorta to abdominal aorta). The celiac and superior mesenteric arteries receive blood supply from the inferior mesenteric artery. Case 2: Computed tomography image showing ascending aortic dilatation and calcification of the entire circumference of the distal arch accompanied by stenosis and a section of the extensively diseased aorta extending from the descending aorta to the abdominal aorta. The left subclavian artery was occluded. Case 3: Stenosis of the descending aorta and abdominal aortic aneurysm. (B) Microscopic polyangiitis. Case 4: Distal descending aorta to the supra-renal abdominal aorta. (C) Unknown cause. Case 6: Stenosis of the descending aorta. Operative findings in Case 2 with Takayasu’s arteritis. (A) We performed a Bentall operation and coronary artery bypass grafting. We passed the 14-mm straight graft through the left thoracic cavity, diaphragm, and left retroperitoneum. The end-to-side anastomosis was created between the Bentall graft. (B) The end-to-side anastomosis was created between the Bentall graft and the abdominal Y-shaped graft. Three-dimensional computed tomography 3–5 years postoperatively. (A) Takayasu’s arteritis (TA). Left: TA in Case 1. Descending aorta to infrarenal abdominal aorta bypass. This figure demonstrates that the celiac and superior mesenteric arteries receive blood supply from the inferior mesenteric artery at 5 years postoperatively. Middle: TA in Case 2. Ascending aorta to bilateral external iliac artery bypass with Bentall surgery and coronary artery bypass grafting. Right: TA in Case 3. Descending aorta to infrarenal abdominal aorta bypass. (B) Microscopic polyangiitis in Case 4: Descending aorta to abdominal aorta bypass and Y-grafting with aneurysmectomy. (C) Unknown cause in Case 6: Descending aorta to the distal descending aorta bypass. Preoperative Baseline Characteristics. Proximal lesion: proximal end at the descending aorta near the thoracic vertebra. Distal lesion: distal end at the descending aorta or abdominal aorta near the thoracic vertebra or lumbar vertebra.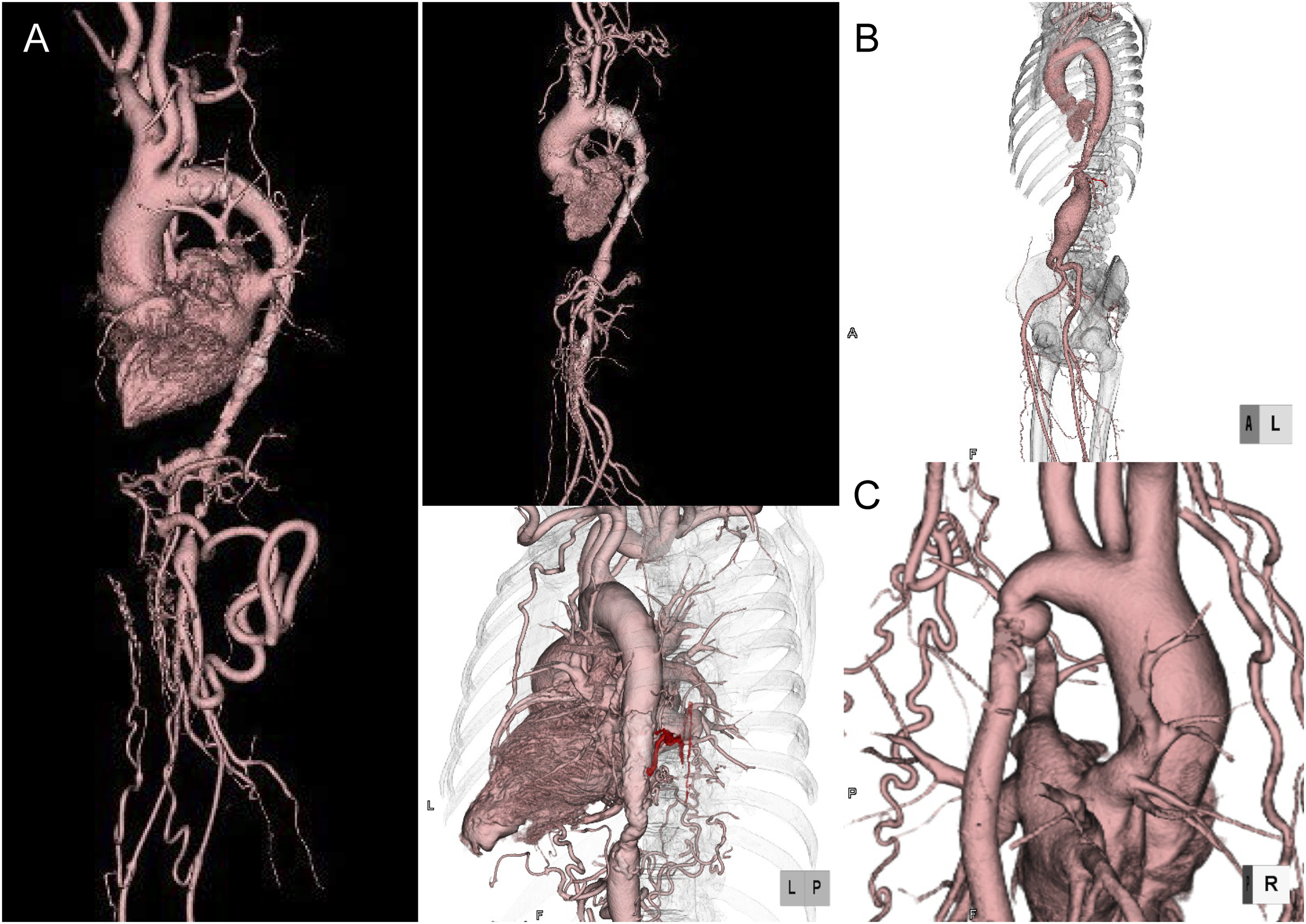
Surgical Indications and Techniques
The three patients with TA (patients 1, 2, and 3) underwent surgery for heart failure due to uncontrolled hypertension. One female patient (patient 4) underwent surgery owing to the rapid progression of stenosis and dilation of the aorta due to microscopic polyangiitis. The remaining two patients (patients 5 and 6) underwent surgery owing to intermittent claudication in both lower limbs.
Operative Data.
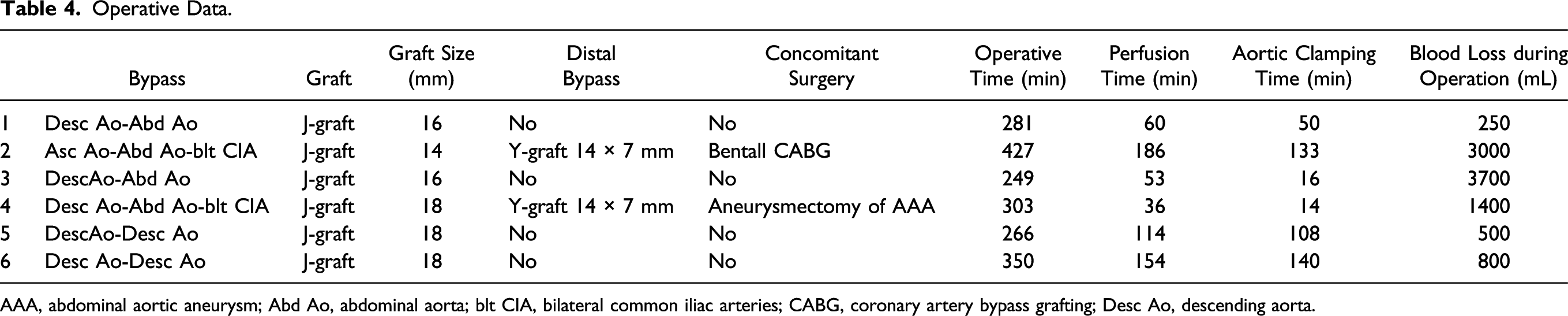
AAA, abdominal aortic aneurysm; Abd Ao, abdominal aorta; blt CIA, bilateral common iliac arteries; CABG, coronary artery bypass grafting; Desc Ao, descending aorta.
We made a subcostal incision in the ninth space for two of the patients with TA (patients 1 and 3) who underwent bypass surgery from the descending aorta to the infrarenal abdominal aorta. The right lateral decubitus position was selected, similar to the position used for thoracoabdominal aortic surgery. In these two cases (patients 1 and 3), it was necessary to perform the end-side anastomosis on the descending aorta; hence, we performed a thoracotomy in the lateral decubitus position. Left heart bypass was performed using a centrifugal pump, and the retroperitoneal space was subsequently cleared. We then exfoliated the descending and abdominal aortas and performed taping around the aorta at the site of the normal aorta without stenosis due to calcification or fiber thickening. Next, we created the route from the left thoracic cavity through the diaphragm to the left retroperitoneum, running under the abdominal internal oblique muscle; this was achieved within approximately 15 minutes. The normal aorta without calcification or wall thickening was routinely selected as the clamping site to avoid aortic dissection and pseudoaneurysm.
In one of the patients with TA (patient 2), the aortic wall of Valsalva was thickened and partially penetrated; therefore, a Bentall operation was performed. This approach involved a median sternotomy and a left paramedian abdominal incision. The retroperitoneum was cleared, and the route to the abdominal aorta was created from the left thoracic cavity to the left retroperitoneum. First, an end-to-side anastomosis was made to the common iliac artery with a 14 × 7 × 7 mm Y-shaped graft because of severe abdominal aortic wall calcification. Coronary artery bypass grafting, in which saphenous vein grafts were anastomosed to the distal right coronary artery and the distal left anterior descending artery, was performed without cardiopulmonary bypass on the beating heart. We could not use the left internal thoracic artery due to a left subclavian artery obstruction. Aortic cannulas were inserted into the ascending aorta, and the reconstructed abdominal bypass graft and venous cannula were inserted into the right atrium. We passed the 14-mm straight graft through the left thoracic cavity, diaphragm, and left retroperitoneum. An end-to-end anastomosis was created between the Bentall and abdominal Y-shaped grafts. The preferred conduit was a shield-woven vascular prosthesis (J-graft Japan Lifeline Co., Ltd. Tokyo, Japan; Figure 2(A) and 2(B)).
The patient with microscopic polyangiitis (patient 4) was receiving steroids and immunosuppressive drugs; however, the inflammation did not improve, and the aortic stenosis and post-stenotic dilatation progressed, resulting in surgical treatment. We first resected the aortic aneurysm and performed Y-grafting. Subsequently, bypass surgery was performed from the descending aorta to the graft via the diaphragm. Owing to the intense inflammation around the aortic stenosis, we avoided completely replacing the aorta with a graft. Additionally, we avoided reconstructing the intercostal, celiac, and superior mesenteric arteries at the aortic site with intense calcification to prevent paraplegia and impaired blood flow to abdominal organs.
We made a subcostal incision in the fifth intercostal space for the two patients with unknown causes (patients 5 and 6) who underwent bypass surgery from the distal arch to the descending aorta. In the absence of calcification, we considered that the thoracic aorta should be bypassed distally to avoid damaging the intercostal arteries. We used a left heart bypass to control blood pressure when clamping the aorta.
The graft size was determined according to intraoperative judgment and accounted for the size of the aortic anastomosis site.
Operative and Clinical Outcomes
Clinical Outcome.
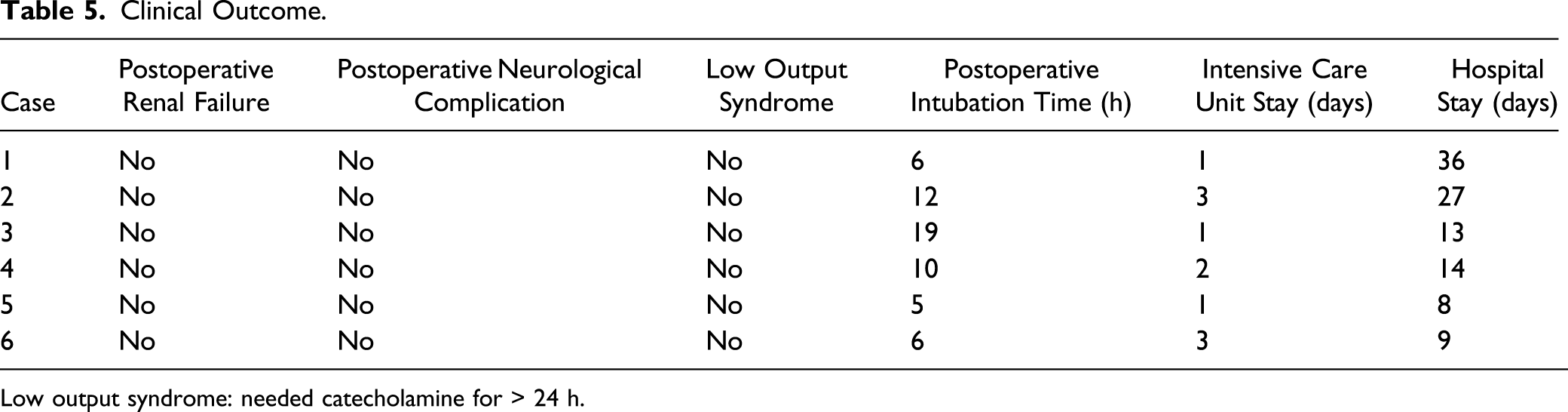
Low output syndrome: needed catecholamine for > 24 h.
Perioperative Data: Preoperative and Follow-Up at Five Years.
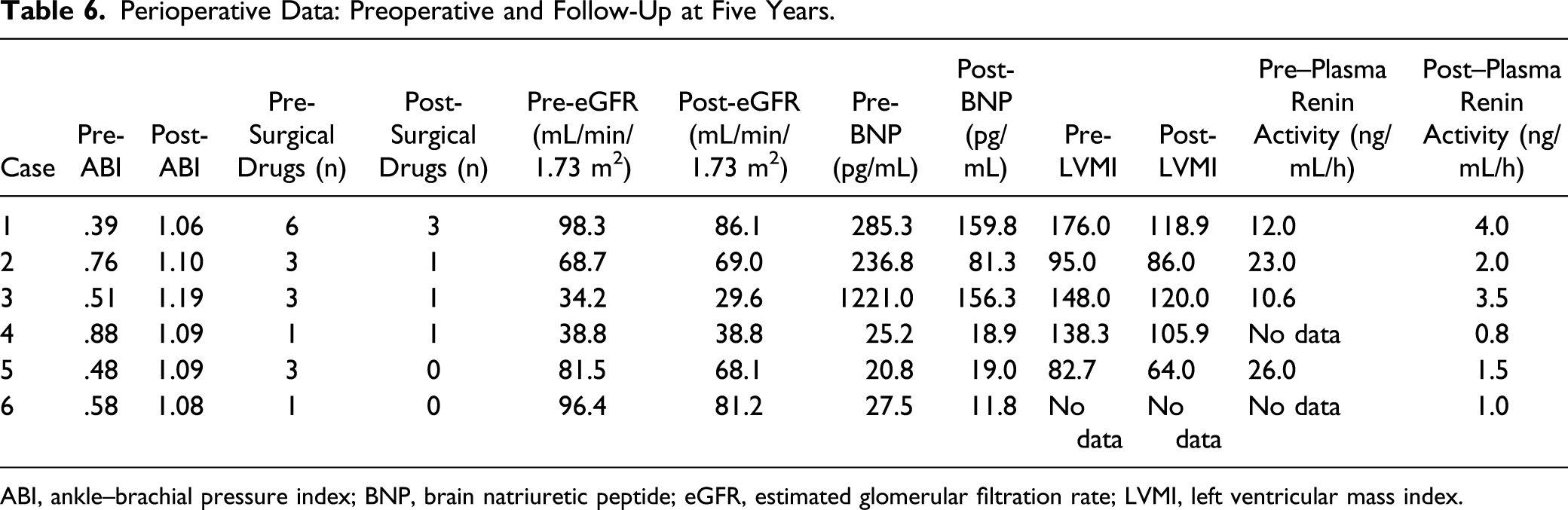
ABI, ankle–brachial pressure index; BNP, brain natriuretic peptide; eGFR, estimated glomerular filtration rate; LVMI, left ventricular mass index.
Postoperative Imaging
Postoperative three-dimensional computed tomography at five years indicated functional graft status (Figure 3), and no pseudoaneurysms or other arterial stenoses were noted in any of the three different surgeries performed. In Case 1, good patency of the bypassed artificial graft and adequate blood perfusion of the lower extremities were observed; however, there may be less blood flow to the abdominal vessels and renal arteries. In Case 2, the anastomosis was to the external iliac artery rather than the abdominal aorta, and good graft patency was confirmed. In other cases, computed tomography revealed good graft patency in locations without aortic calcification.
Discussion
We herein reported the 5-year outcomes of six patients treated with extra-anatomical bypass surgery for MAS. Surgical treatment for MAS should ideally be performed when inflammation, heart failure, and organ ischemia are controlled. 8 Therefore, the primary therapy for MAS is drug therapy, including steroids, to reduce inflammation; however, if inflammation cannot be controlled, cytotoxic and immunosuppressive agents are used. These treatments may prevent aortic stenosis in many patients. 9
However, MAS is characterized by long aortic lesions, and these treatment methods may be inadequate. Various surgical techniques, such as graft insertion, and patch angioplasty, have been reported in the treatment of aneurysms. Endovascular therapy has been used for the treatment of MAS since its introduction in 198010,11; however, it is ineffective if the lesion is long. Only anatomical bypass has been reported to have excellent results for long lesions.12,13
We performed bypass surgery in one patient who received steroids and an adjuvant to control vessel vasculitis inflammation. The active inflammatory phase was short, and the patient had suprarenal aortic stenosis and an abdominal aneurysm, which required bypass surgery from the descending aorta to the infrarenal aorta as well as Y-grafting with an aneurysmectomy. Owing to the intense inflammation around the aortic stenosis, we avoided completely replacing the aorta with a graft. The patient was followed up on an outpatient basis for five years with steroid and immunosuppressive therapy and was relieved of uncontrolled hypertension. Importantly, renal function was preserved.
Inflammation was well controlled in five patients in this study. Although we did not perform imaging tests, such as positron emission tomography–computed tomography or Ga scintigraphy, active inflammation was not observed in any patient on preoperative three-dimensional computed tomography or intraoperative microscopic examination of the aortic wall.
The treatment of MAS is further complicated by TA. Although sporadic, TA may cause lesions not only in the middle aorta but also simultaneously in the aortic root, aortic valve, and subclavian artery. MAS is typically easy to treat; however, surgery becomes difficult with the addition of repairs at other sites. In such cases, careful surgical planning is crucial, as catheter treatment cannot be performed, and all lesions should be resolved simultaneously. We performed Bentall surgery, coronary artery bypass grafting, and aortic bypass surgery simultaneously; however, the operative time was long, and postoperative recovery was slow.
As described above, surgery was performed at the discretion of the cardiologist. However, we had to perform complicated surgery in cases with TA complicated by poorly controlled hypertension and heart failure due to anatomically advanced aortic lesions. Surgical intervention was considered dependent on the length of the aortic lesion and the degree of calcification; hence, three-dimensional computed tomography was performed once a blood pressure difference was observed between the upper and lower limbs. We considered it essential to avoid the calcified aorta and devise a distal anastomosis location so that the bypassed artificial vessel is as short as possible; however, if the anastomosis is impossible due to calcification, it is equally important to anastomose to an artery without calcification. In cases wherein the lesion extends to the thoracoabdominal region, we recommend bypassing the non-calcified aorta through the diaphragm into the non-calcified abdominal aorta to shorten the operation time and reduce the risk of collateral blood circulation disturbance and bleeding complications compared to replacement with an artificial graft.
Despite the many reports of endovascular stenting for aortic coarctation, few have included details of long-term results and clinical improvement. Destruction of elastic fibers in the media and adventitial fibrosis can cause an inadequate vascular response in patients with TA. Similarly, we should consider the possibility of ineffective treatment and conversion to surgical treatment after endovascular stenting. Excellent long-term prognosis is one of the essential factors for selecting treatment, given that most patients with MAS are relatively young. Therefore, we believe that endovascular treatment should be used sparingly and limited to patients with localized aortic stenosis or those at high perioperative risk. Our top priority is long-term graft patency and improved blood flow in the abdominal organs. Recently, endoscopic surgery with a small incision 14 and revascularization using the new four-branch Dacron graft have been reported, and good long-term results are expected; however, careful follow-up after surgery is required.15,16
The thickened intima and adventitia of patients with TA can cause arterial dissection and anastomotic pseudoaneurysm. Destruction of the media’s elastic component occurs before adventitial fibrosis can weaken the vessel wall and cause complications. 17 The incidence of anastomotic aneurysms was 13.8% at 20 years of age, and the cumulative rate of anastomotic aneurysms was 12.2%, 21.2%, and 37.3% at 10, 20, and 30 years of age, respectively. 18 In a recent multicenter study of 166 vascular procedures performed in patients with TA, the 5- and 10-year aortic event-free survival rates were 56% and 45%, respectively. Although we observed good results in the current 5-year follow-up, regular monitoring using various imaging modalities is required.
The purpose of surgical treatment is to reduce organ ischemia and cardiac load through optimal blood pressure management. We performed regular outpatient follow-up and confirmed bypass graft patency using ABI and diagnostic imaging to evaluate organ dysfunction. Additionally, we confirmed that no new lesions had appeared. In the six cases of MAS reported here, the number of antihypertensive drugs was significantly reduced five years postoperatively, indicating good blood pressure control. Moreover, there was no recurrence of lower-limb ischemia or abdominal ischemia and no readmissions.
The strain on the left ventricle results from pressure overload; heart failure; sudden cardiac death; and brain complications, such as cerebral hemorrhage. On echocardiography, left ventricular mass and left atrial volume indices represent the left ventricular diastolic status due to cardiac load. 19 Kim et al. 13 reported that all these echocardiographic parameters improved in all 14 patients in their study following bypass surgery; left ventricular diastolic dysfunction and LVMI improved immediately after surgery and were observed for one year. Our observations were conducted for five years, and all showed improvement in LVMI. During our 5-year follow-up, these parameters remained stable, and reductions in the LVMI, brain natriuretic peptide level, and plasma renin activity were observed. Thus, our follow-up period of five years is relatively short for determining late complications and mortality. Therefore, consistent follow-up is still needed regarding cardiovascular or cerebrovascular diseases.
The study findings indicate that our surgical technique results in a reduction in endocrine stress due to improved adrenal and renal blood perfusion, with good prosthetic graft patency for five years. Therefore, this technique may contribute to the reduction of cardiac, aortic, and cerebrovascular complications associated with hypertension and increased endocrine stress.
This study has some limitations. Our current study was a retrospective case series with a small number of patients. Additionally, we reported only surgical bypass results and did not compare the endovascular treatment data. In future studies, we need to confirm the indications for endovascular treatment, determine whether endovascular or open bypass surgery is preferable based on preoperative imaging, and evaluate the long-term prognosis over a period of ≥ 10 years.
Conclusion
Extra-anatomical bypass for MAS is safe and effective and was shown to help prevent renal failure and relieve critical ischemic symptoms during a 5-year follow-up period.
Footnotes
Author contributions
All authors contributed equally to the article, revised the article critically for intellectual content, read and approved the final version, and agreed to be accountable for this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Data associated with this manuscript are not publicly available but can be made available by the corresponding author upon request.