
Abstract
Mycotic aneurysms are vascular dilations caused by fungal or bacterial infections. The involvement of the pulmonary artery or its branches is extremely rare with only a few cases reported in the literature posing a diagnostic challenge. We present the case of a young adult patient with acute myeloid leukemia undergoing chemotherapy, who presented with febrile neutropenia, recurrent bacteremia due to Pseudomona Aeruginosa and Klebsiella Pneumonie and hemoptysis. The management was unconventional, opting for the placement of a covered endovascular stent, being the first successful case with this reported technique. Rapid detection of this pathology and individualization in the management of each patient is essential because of high risk of mortality due to sepsis and rupture of the aneurysm.
Keywords
Introduction
Mycotic aneurysms (MA) represent 1% to 3% of all arterial aneurysms. They are most frequently located in the femoral artery, abdominal and thoracic aorta. Mycotic aneurysms of the pulmonary arteries are exceedingly rare, with only 39 cases reported from 1949 to 2018. 1 We present the case of a mycotic pulmonary aneurysm (MPA) in a patient with acute myeloid leukemia (AML) undergoing chemotherapy treatment, febrile neutropenia, and recurrent bacteremia due to Gram-negative germs; the first to be successfully treated with the placement of a covered stent.
Case Report
39-year-old male, hospitalized for spinal cord relapse secondary to M3 AML diagnosed 1 year earlier. In chemotherapy with venetoclax/azacytidine, he presented high-risk febrile neutropenias associated with Pseudomona Aeruginosa and Klebsiella Pneumonie bacteremia, with improvement in cell lines and clinical condition after antibiotic treatment. He suddenly developed massive hemoptysis of approximately 300cc with clot, dyspnea, and desaturation requiring supplemental oxygen.
Laboratory exams.
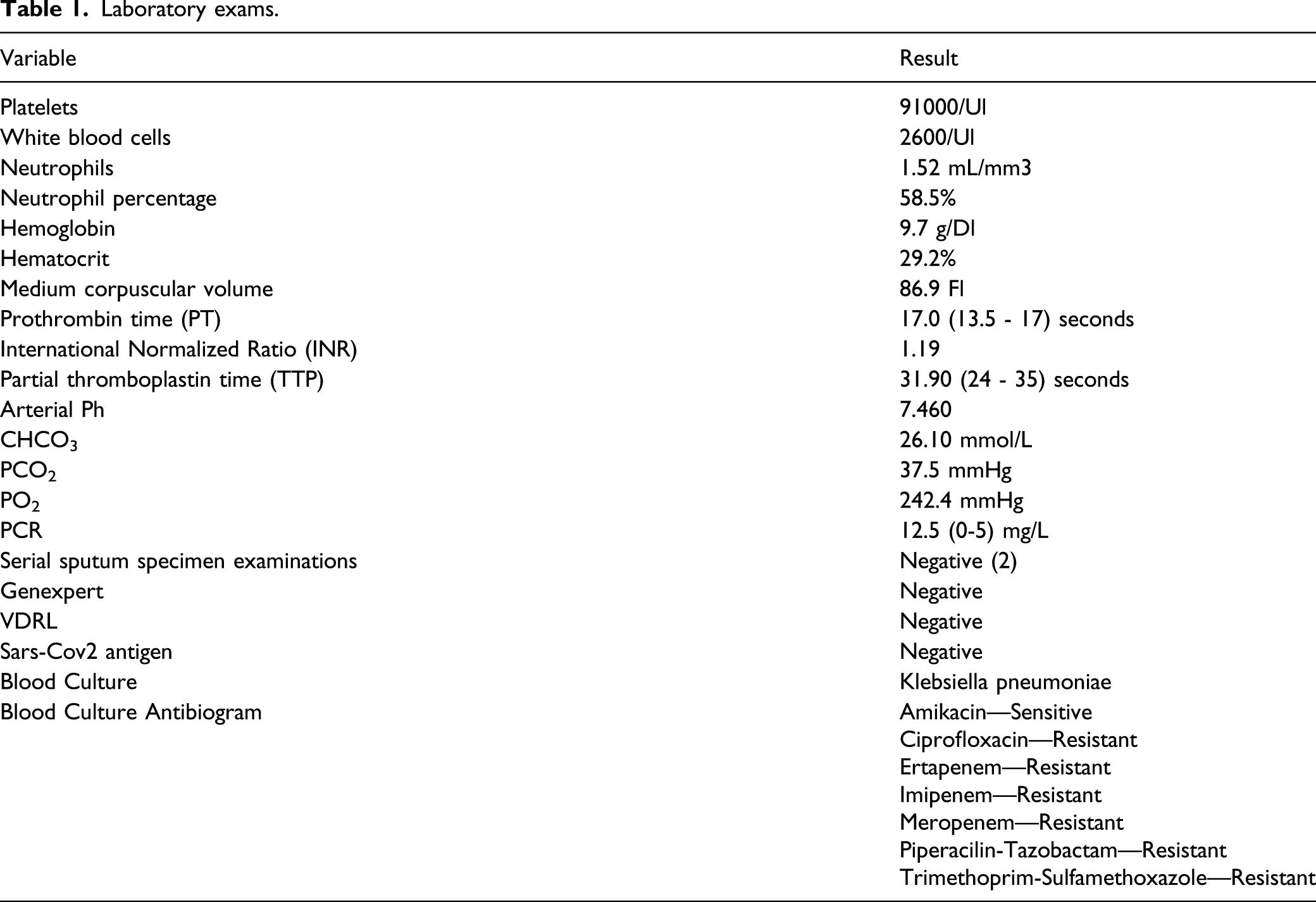
Initial chest images were taken considering that his clinical-radiographic condition did not correspond to an acute infectious process because he did not present the classic respiratory symptoms (cough, fever, dyspnea, tachypnea, etc.). The nonsignificant reduction in platelet count, associated with normal clotting times and the bleeding pattern (not bilateral) ruled out an associated coagulopathy.
Electrocardiogram showed signs of right overload (S1Q3T3), for which a transthoracic echocardiogram was performed with preserved ventricular function (LVEF 64%) and cavities free of vegetations.
We researched the patient’s previous clinical history and found a former CTA scan in which the vascular structures were intact (no masses, adenopathy, or alterations in the airspace and interstitium), but given the current hemodynamic alteration, it is decided to take a new CTA scan without intravenous contrast which highly suggested a pulmonary embolism (PE) (Figure 1). Lower extremity duplex was negative for deep vein thrombosis, Wells score was 5 points, so a chest computed tomography angiography with PE protocol was performed. The condensation of the airspace in the lingula and a lateral sector of the posterior segment of the left upper lobe was found without signs of PE. A mycotic aneurysm was suspected due to the volume of the hemoptysis, the history of immunosuppression, blood culture and images. A: CTA with pulmonary embolism protocol. B. Volumetric reconstruction. Arrows: condensation of the airspace in the lingula and a lateral sector of the posterior segment of the left upper lobe. Circle: Aneurysm at the left lower lobe vasculature.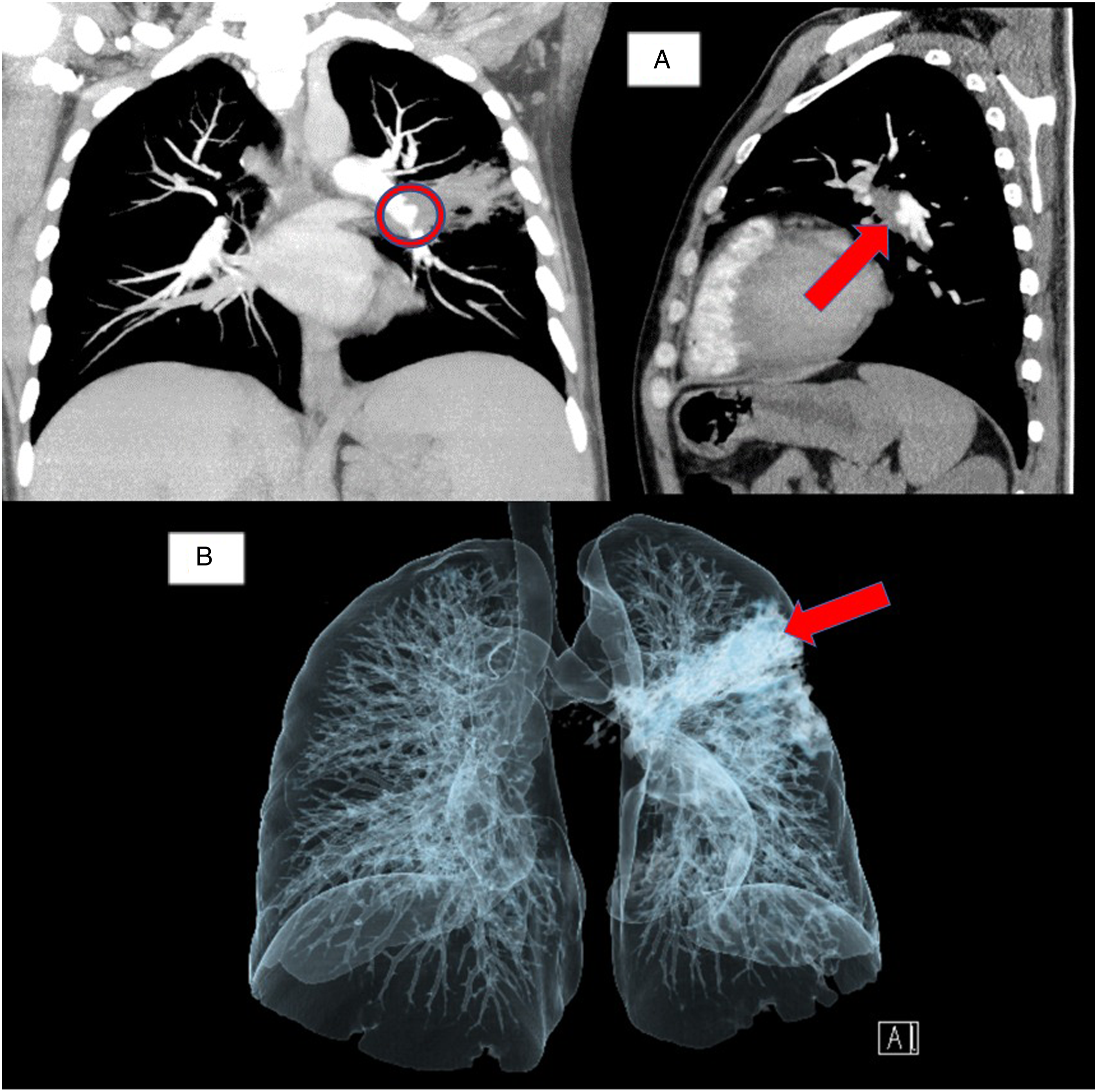
The left pulmonary artery angiography showed a saccular aneurysm at the level of the origin of the lower left segmental artery of approximately 16 × 18 mm in diameter with a wide neck that involved the left-lateral-inferior branch. The aneurysm was embolized with a coil, subsequently with a microcatheter and a microguide. A peripheral metallic stent graft was positioned, and it was postdilated. The hemorrhage was successfully controlled, with total occlusion of the aneurysmatic dilatation (Figure 2). There were no complications. A: Arrow shows saccular aneurysm at the level of the origin of the lower left segmental artery of approximately 16 × 18 mm. B: Arrow shows management with covered stent.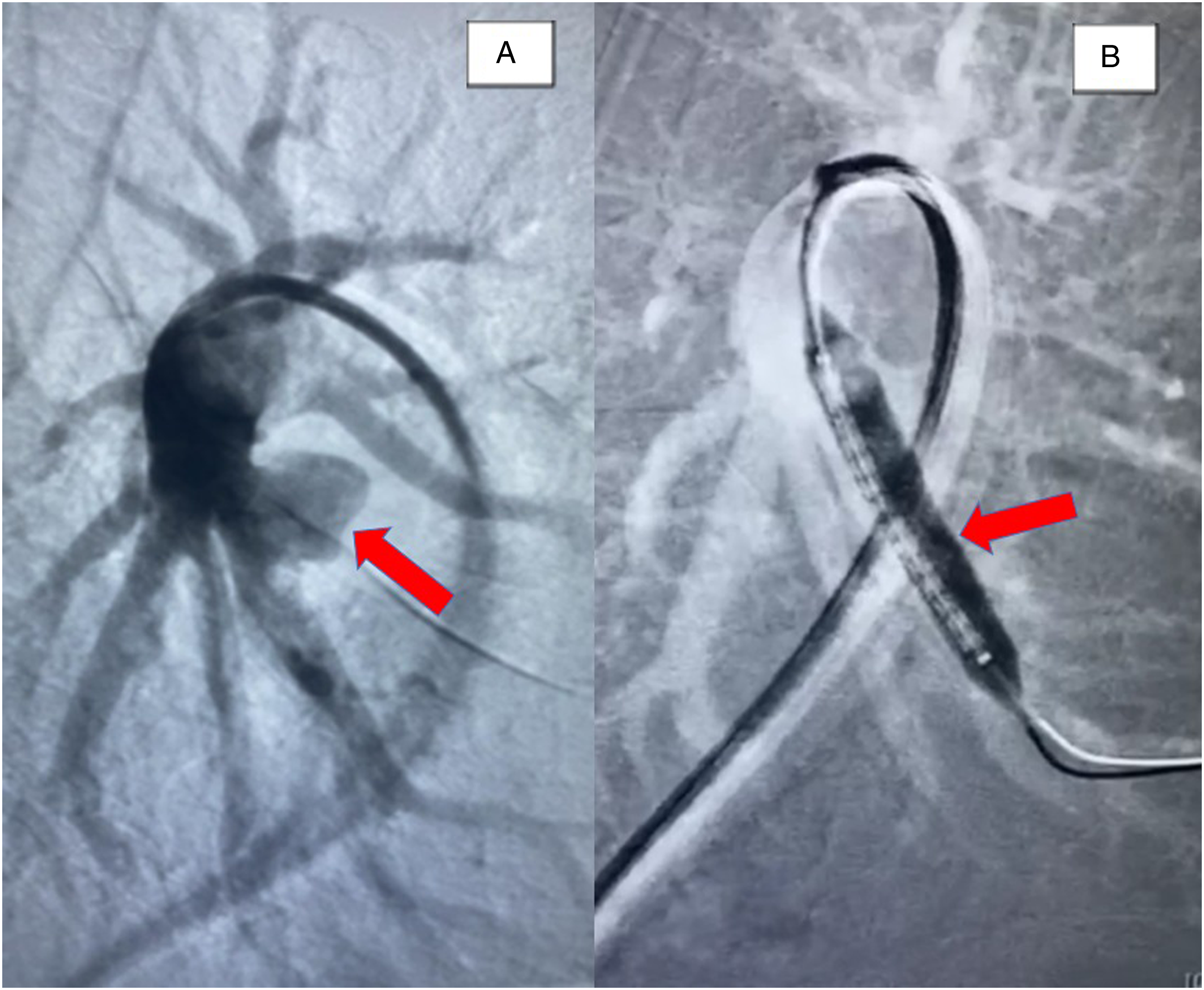
After the procedure, the patient was managed using dual antiplatelet therapy (acetylsalicylic acid/clopidogrel). Multiresistant K. pneumonie bacteremia was managed with meropenem and polymyxin B. Follow-up showed successful response to the antibiotics, with complete remission of the infection in 30 days after hospital discharge. No new episodes of hemoptysis were described. No evidence of additional bleeds was observed on the follow-up CT scan (Note: Previous images are not available due to a change in the health care center image database.)
Discussion-Conclusions
A mycotic aneurysm is an irreversible focal dilation of an artery, associated with the destruction of the 3 layers (intima, media, and adventitia) of the vessel wall due to infection. 2 Risk factors are: arterial injury, history of infections, immunosuppressed status, and atherosclerosis in the elderly. 3 Our patient had recurrent Gram-negative bacteremia, immunosuppression due to his underlying disease (AML), and chemotherapy.
The most common causative agents are Gram-positive bacteria such as Staphylococcus and Streptococcus spp;2,4 however, in patients with hematologic diseases and associated febrile neutropenia, up to 80% of bacteremia are caused by Gram-negative bacteria, especially those who received reinduction chemotherapy. 5 To date, 6 cases of AML patients who presented MA have been reported, all of which had febrile neutropenias and associated bacteremia, only 1 of them was located in the pulmonary vasculature, with Aspergillus being the etiological agent.
Compared with MA in other locations, those described in the pulmonary arteries occur in young patients and equally in men and women.1,6 Those that affect the pulmonary trunk and branches are called central or proximal, those that are located in intrapulmonary segmental and distal arteries are called peripheral. 7 Of the 39 cases reported until 2018, 15 were central and 24 peripheral (13 involved right branches, 3 left branches, and 8 were bilateral). 1 Our case corresponds to a young adult man who presented with a vascular alteration in the most frequent group of pulmonary MA (peripheral aneurysm), however, it presented with involvement of the left branches, which are the least affected.
The most frequently described symptoms of pulmonary MA are hemoptysis, cough, and fever. 8 However, in the case presented, the patient only manifested the first 1. Presence of MPA should be suspected whenever this symptom is shown. Differential diagnoses to consider include: PE, Rassmusen aneurysm and ischemic involvement of the arterial walls due to infection of the vasa vasorum. 9
Various pathophysiological mechanisms have been proposed in the development of pulmonary MA.1,4,9 Based on the clinical history, we can assume that the MPA in our patient was generated as a consequence of a direct extension to the vessel wall due to hematogenous dissemination of intraluminal septic emboli from distant foci.
MPA carry high morbidity and mortality from fulminant sepsis and massive hemorrhage when not treated promptly. Up to 80% of patients who do not undergo surgical intervention die compared to those who undergo intraoperative procedures in which rates are reduced to 22%, therefore, rapid identification is essential to prevent the development of these potential lethal complications.1,4,10
Due to its low incidence, there is no clear consensus on the treatment approach to this pathology. Currently, there are 3 treatment options to address each case individually: medical, surgical and endovascular. Among the 39 reported cases, 16 received pharmacological treatment, 18 surgical and 5 were managed endovascularly (coil embiolization of placement of covered stent). Both endovascular options carry significant mortality in the reported literature. Four cases of coil embolization have been reported, of which 75% have died. Placement of an endovascular stent for treatment of pulmonary MA has only been reported in a single patient, who did not survive. In our case, the patient was managed with a covered stent without complications, thus being the first successful report of management with this technique according to our review. 1
Footnotes
Declaration of Conflicting Interests
The author(s) declare(s) that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sector.
Ethics Statement
The author(s) declare(s) that this article adhered to the existing national and international regulations regarding biomedical research, to the guidelines of good clinical practices of the international harmonization committee and to the ethical principles of the Declaration of Helsinki. In addition, informed consent has been obtained from the patient for publication of the case report and accompanying images.