
Abstract
Background
To evaluate the efficacy and safety of ascending aortoiliac bypass surgery for one-stage repair of adult coarctation of the aorta (CoA) and concomitant cardiac disease.
Methods
From March 2012 to October 2018, 51 consecutive CoA patients were treated with ascending aorta to bilateral iliac artery bypass concomitant with and cardiac surgerical procedures performed for a variety of reasons. A Y-shaped graft was used for the bypass procedure. We evaluated early outcomes, including postoperative death, systolic blood pressure and differences between upper and lower limb blood pressure.
Results
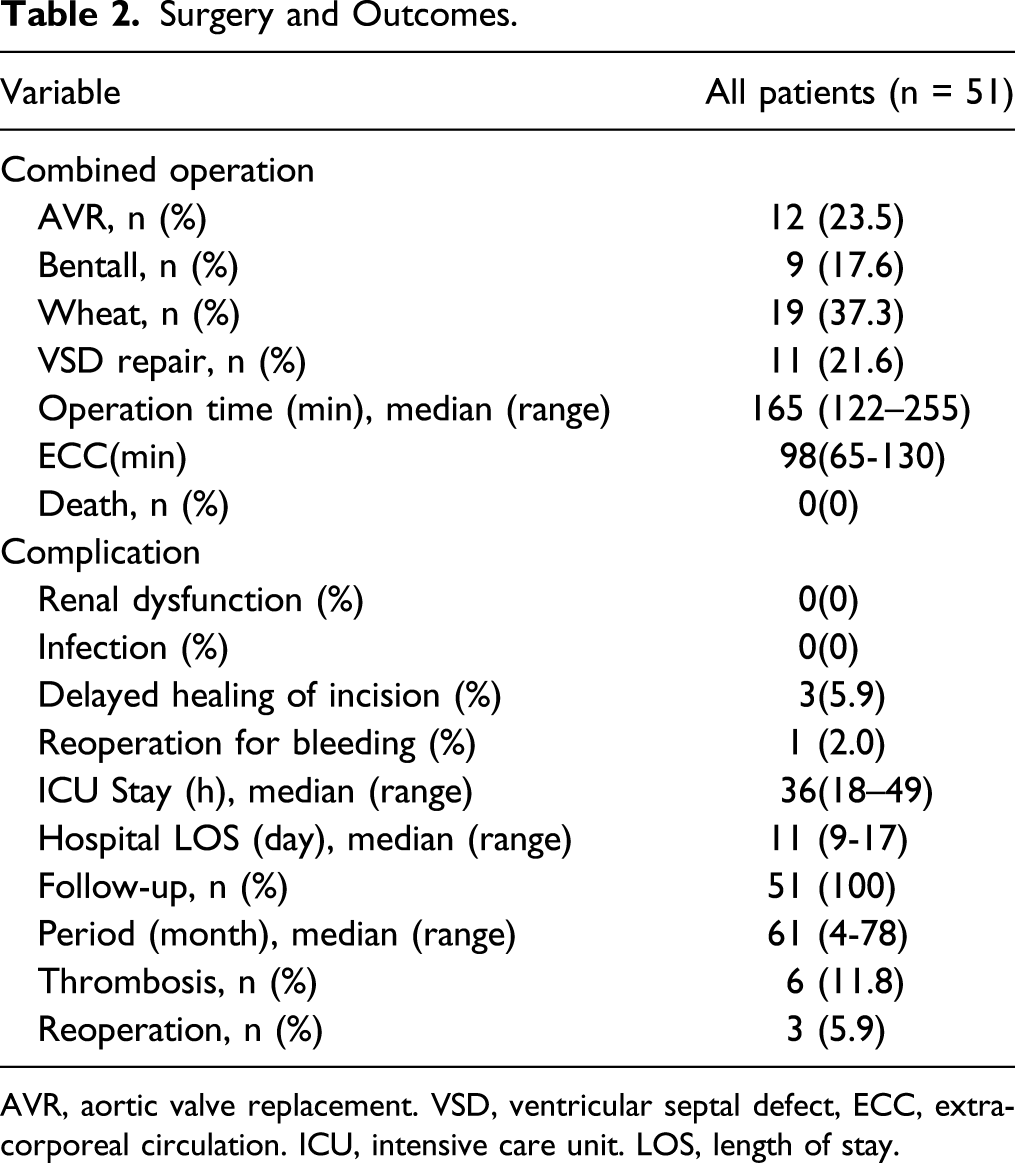
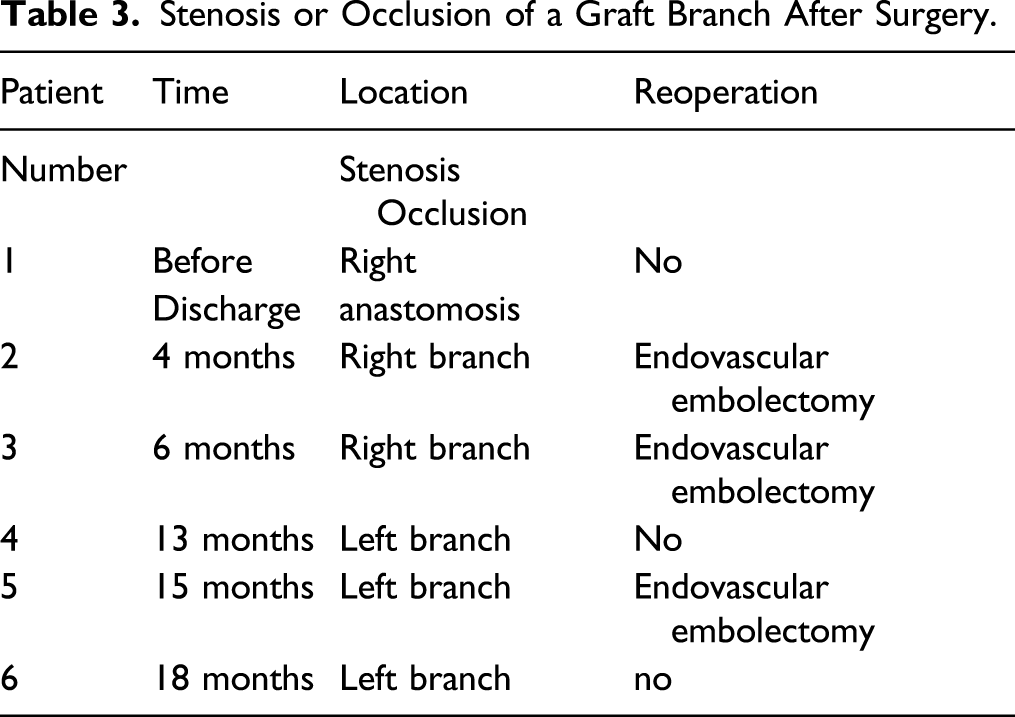
The average age was 41 years and 64.7% of patients were men. Simultaneous cardiac procedures included aortic valve replacement, ventricular septal defect repair, Bentall procedures and Wheat procedures. No deaths occurred in the early postoperative period. Three patients had delayed healing at the site of the abdominal lower quadrant incisions. The average systolic pressure in the upper limb and the average difference between the upper- and lower-limb blood pressure decreased significantly after surgery (162.7 ± 13.4 mmHg vs 128.4 ± 6.7 mmHg, P = .000; 69.6 ± 15.6 mmHg vs 8.7 ± 7.6 mmHg, P = .000, respectively); The systolic blood pressure in the lower limb increased after bypass surgery (93.1 ± 6.2 mmHg vs 119.6 ± 7.7 mmHg, P = .000). The follow-up rate was 100%, with an average follow-up time of 61 months. Six patients (11.8%) had graft stenosis or occlusion. Three patients (5.9%) underwent endovascular embolectomy.
Conclusions
In our small series, ascending aortoiliac bypass for one-stage repair of CoA with concomitant cardiac lesions appears safe and efficacious in effectively reduceing differences between upper and lower limb systolic blood pressure. Further study with larger sample size and longer follow-up is needed.
Introduction
Coarctation of the aorta (CoA) is a relatively common cardiac anomaly that accounts for 7% of all congenital heart defects.1,2 In some patients, diagnosis is delayed until adulthood, and is discovered due to complications such as heart failure, hypertension, or cerebral hemorrhage. The reported fatality rate in patients younger than 50 years has been as high as 75%. 1 CoA has been recently linked to certain genetic alterations that have been associated with other cardiac diseases. 3 CoA is often complicated by obstructive left heart disease, such as bicuspid aortic valve, hypoplastic left heart syndrome, and hypoplastic aortic arch.4,5 Patients in whom CoA is diagnosed in adulthood may have a combination of cardiac lesions, including aortic stenosis, ascending aortic dilatation, and aortic dissection. Most studies discussing surgical treatment of CoA with concomitant cardiac lesions, particularly single-stage repair of these comorbid conditions, are limited to sporadic case reports.6,7
Some surgeons have adopted techniques such as ascending aorta-abdominal aorta bypass or ascending aorta-thoracic aorta bypass.7,8 However, these invasive approaches carry a high risk of postoperative gastrointestinal complications and increased bleeding. We have adopted a repair technique that involves constructing a Y-shaped graft from the ascending aorta to the external iliac arteries while performing repair of the comorbid cardiac lesions to reduce the trauma and risks associated with a staged procedure. This article reviews our clinical experience with this surgical approach and analyzes its safety and efficacy.
Patients and Methods Study Design and Patients
The study enrolled 51 consecutive patients with CoA and concomitant cardiac diseases admitted at Fuwai Hospital between March 2012 and October 2018. Their diagnoses were confirmed by cardiac ultrasonography and computerized tomography (CT) scanning of the aorta. All discharged patients were followed up in the outpatient clinic with CT angiogram. The inclusion criteria were as follows: patients aged >28 years; cardiac pathology requiring median thoracotomy; a difference between the upper and lower limb systolic blood pressure >30 mmHg or refractory hypertension (systolic blood pressure >160 mmHg) in the upper limb; CoA cases unsuitable for balloon dilatation and stent placement (such as severely calcified; angle of the stenosis >90°; and length of the stenosis segment >4 cm); diameter of the common iliac arteries >6 mm; and no significant arterial occlusive disease distal to the iliac artery. Exclusion criteria included post-stenotic dilatation >4 cm; distal to the coarctation extensive arterial occlusive disease distal to the target external iliac artery; and history of prior abdominal surgery or abdominal inflammatory process (appendicitis, cholecystitis, cholangitis, peritonitis, and pancreatitis). This study was approved by the Ethics Committee of Fuwai Hospital (2015025).
Surgical Procedure and Management
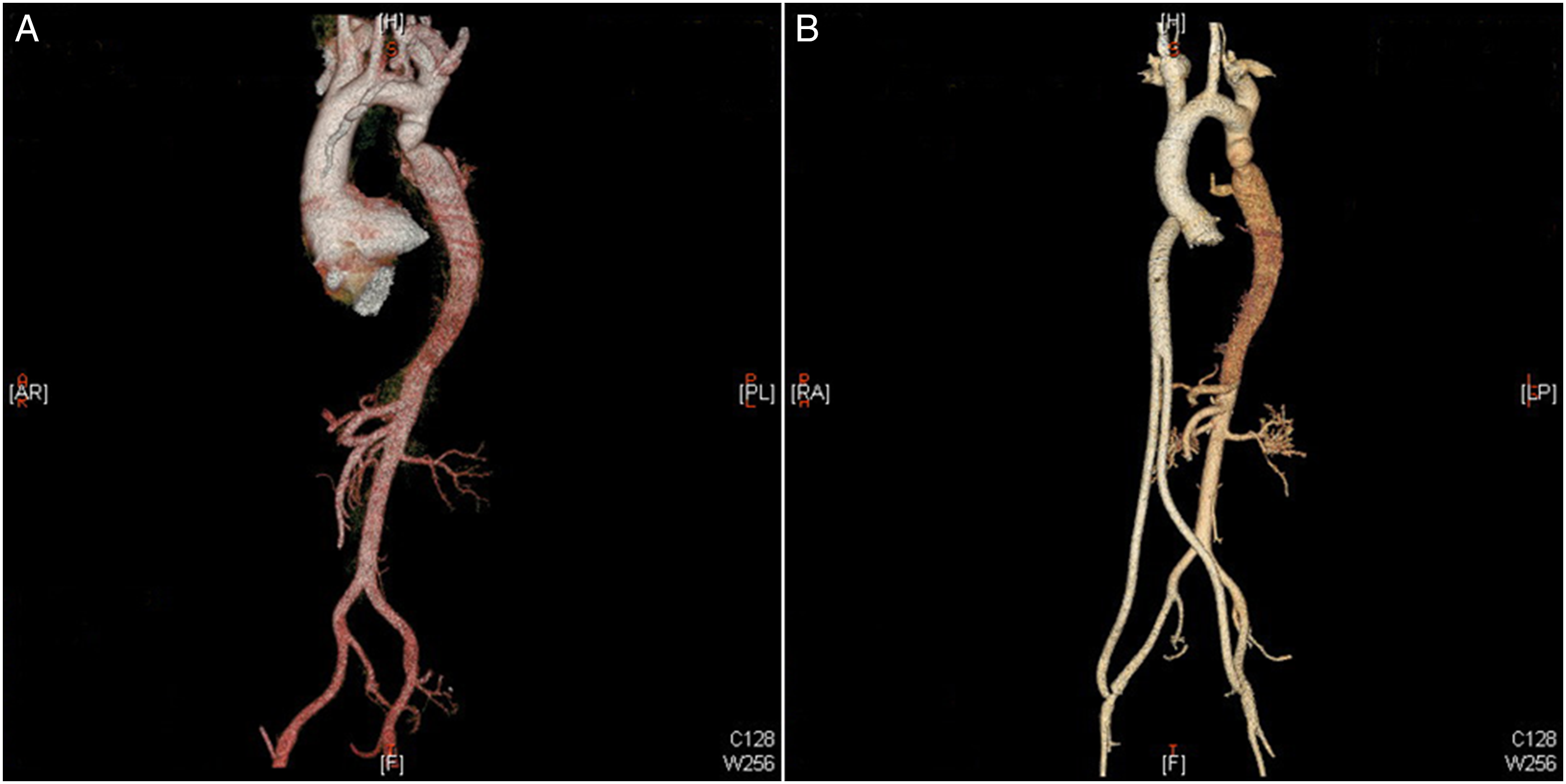
All patients underwent surgery with extracorporeal circulation (ECC) and mild hypothermia. A 16 mm × 8 mm × 8 mm Y-shaped graft (Maquet, Wayne, NJ, USA) was used for the bypass procedure. Upper and lower limb arterial lines were placed to monitor arterial pressure. The external iliac vessels were exposed near the iliac fossa by making an oblique incision 2 cm above the inguinal ligaments. A medial sternotomy was then performed. Cannulation of the ascending aorta was used for the ECC during antegrade perfusion of the upper and lower body under mild hypothermia. After aortic valve replacement and ventricular septal defect (VSD) repairs were completed, ECC was withdrawn when the heart was restarted. The incision was extended from the sternum to 2 cm below the xiphoid process. A tunnel was created, with assistance of a tunneling device, from under the xiphoid process to the iliac fossa; the iliac arteries were exposed using an intraperitoneal approach, The tunneler performed advanced on either side of the ligamentum teres along the anterior surface of the right liver, and delivered so as to exit at the incision superior to the inguinal ligament from the abdominal cavity. Care is taken to confirm that there is no extraneous tissue (mesenteric, intestinal wall, etc.) overlying the translucent peritoneum, before incising the peritoneum and delivering the tunneling device. Each limb of the bifurcated Dacron graft is delivered in this fashion to each external iliac artery. The proximal main body of the graft is then inserted into the pericardial cavity through the subxiphoid incision. The ascending aorta was occluded using a side-biting clamp, followed by end-to-side anastomosis between the aorta and the proximal end of the Y-shaped graft. The other two distal ends were anastomosed end-to-side with each external iliac artery (Figure 1). Finally, protamine was administered to reverse the effects of heparin. We used a slightly different protocol during aortic root surgery (Bentall/Wheat): when the heart was restarted, ECC was withdrawn after the proximal and distal ends of the Y-shaped graft were anastomosed in the aforementioned order. A CoA with aortic root aneurysm; B Ascending aorta and bilateral iliac arteries bypass surgery with aortic root replacement (Bentall's procedure).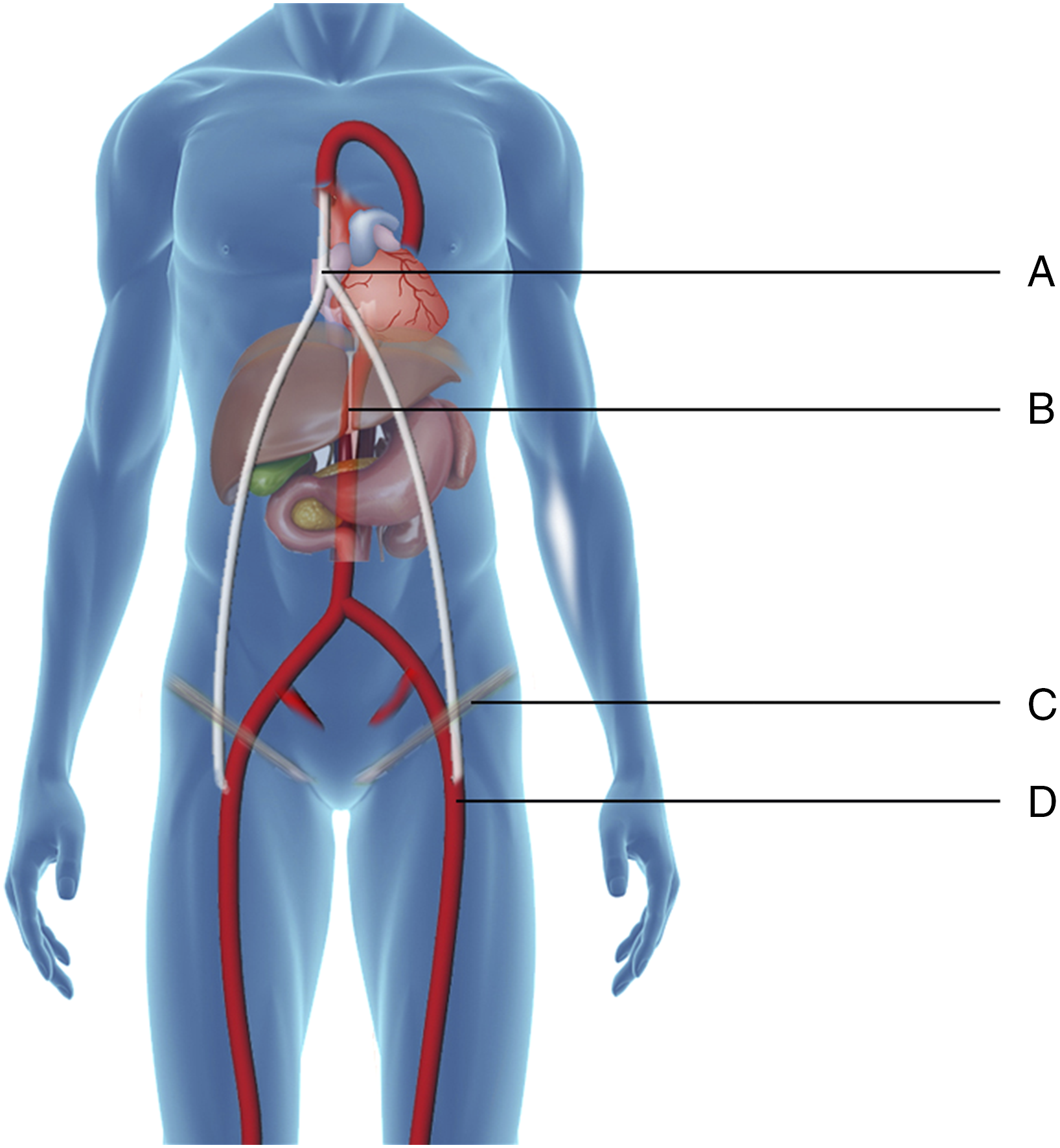
We evaluated the rates of early postoperative mortality (before discharge and within 30 days of surgery) and complications. Graft patency was assessed by follow-up CT. Antiplatelet therapy with aspirin was initiated in all patients after removal of the endotracheal tube and continued for at least 1 year. For those patients who underwent aortic valve replacement, anticoagulation with warfarin was added to the regimen. All patients received antihypertensive treatment with calcium channel blockers or/and angiotensin converting enzyme inhibitors before and after surgery.
Statistical Analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS) software, version 21.0 (IBM, Armonk, NY, USA). Measurement variables are represented as means with standard deviations for continuous variables; if variables were not normally distributed, the median and quartile are provided. Frequencies and percentages are provided for categorical variables. Descriptive analysis was used for main results, beyond that, paired t-tests were used to compare blood pressure measurements before and after surgery, and the Wilcoxon rank sum test was performed as appropriate.
Results
Patient Characteristics.
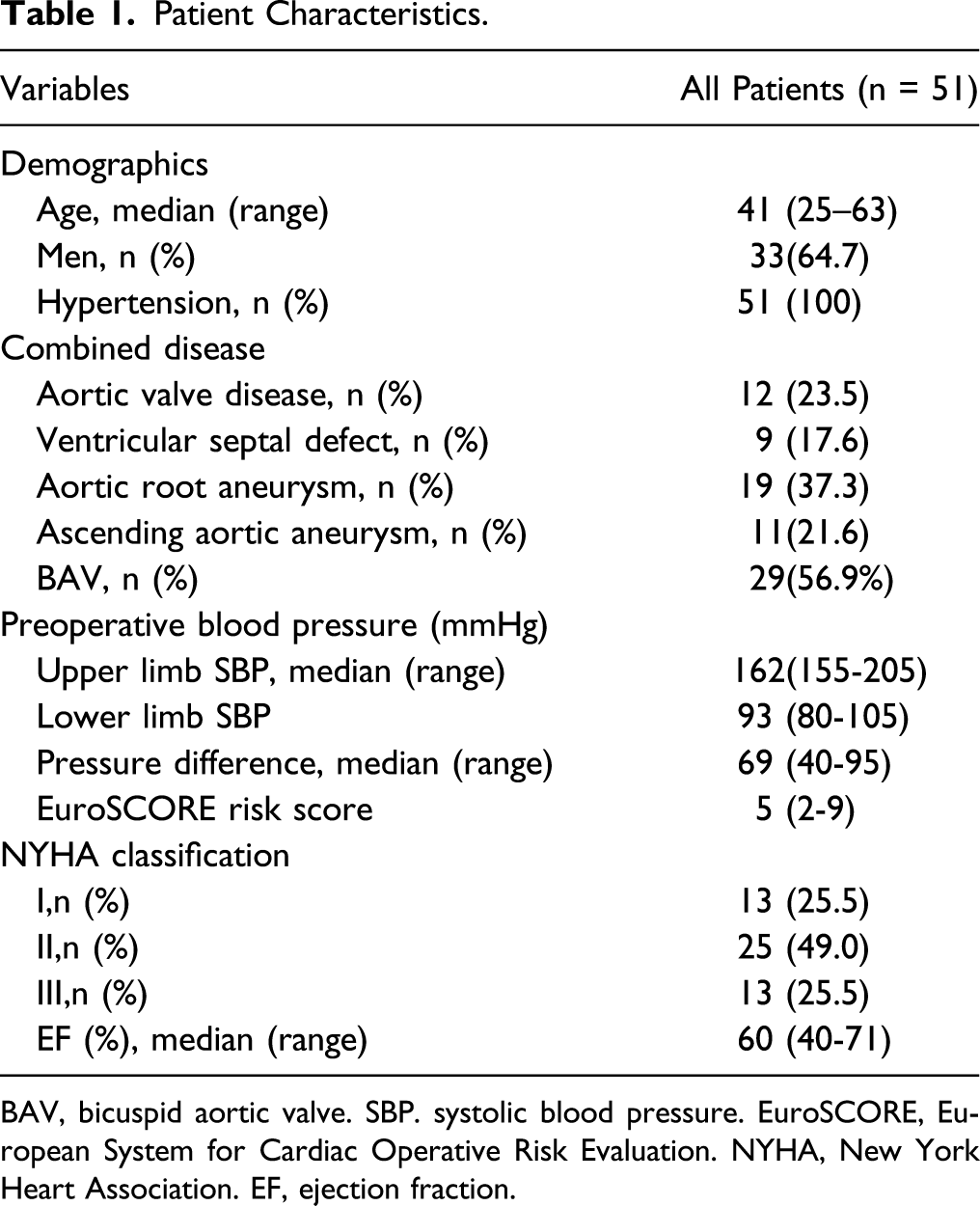
BAV, bicuspid aortic valve. SBP. systolic blood pressure. EuroSCORE, European System for Cardiac Operative Risk Evaluation. NYHA, New York Heart Association. EF, ejection fraction.
All patients underwent CoA repair using the ascending aorta to iliac arteries bypass technique; 12 patients underwent simultaneous aortic valve replacement, 9 patients underwent VSD repair, 19 patients underwent Bentall procedures, and 11 underwent Wheat procedures (Figures 2 and 3). The average operating time was 165 (122–255) minute and average ECC time was 98 (65–130) minute. No death occurred in the early postoperative period. None of the patients presented with postoperative renal dysfunction. Delayed healing at the site of the abdominal lower quadrant incisions was reported in three cases. No abdominal complications, such as bleeding, infection, or bowel obstruction, were detected (Table 2). The average systolic pressure in the upper limb and the average difference between the upper and lower limb systolic blood pressure decreased significantly after surgery (162.7 ± 13.4 mmHg vs 128.4 ± 6.7 mmHg, P = .000; 69.6 ± 15.6 mmHg vs 8.7 ± 7.6 mmHg, P = .000, respectively); the systolic blood pressure in the lower limb increased markedly after bypass surgery (93.1±6.2 mmHg vs 119.6±7.7mmHg, P=.000). The diagram of the surgical procedure. We use a tunneling device as a guide to perform the process. Tunneling device was advanced through the right or left side of the round ligament of the liver at the anterior surface of the right liver, and arrived to exit at the incision superior to the inguinal ligament from the abdominal cavity. The ascending aorta was occluded using a side-biting clamp, followed by end-to-side anastomosis between the aorta and the proximal end of the Y-shaped graft. The other two distal ends were anastomosed end-to-side with each external iliac artery. A: Y- shaped graft; B: round ligament of the liver; C: inguinal ligament; and D:external iliac artery. A. Coarctation of the aorta with aortic valve stenosis; B. Three-dimensional reconstruction of computed tomography after ascending aorta to bilateral iliac arteries bypass surgery with aortic valve replacement. Surgery and Outcomes. AVR, aortic valve replacement. VSD, ventricular septal defect, ECC, extracorporeal circulation. ICU, intensive care unit. LOS, length of stay.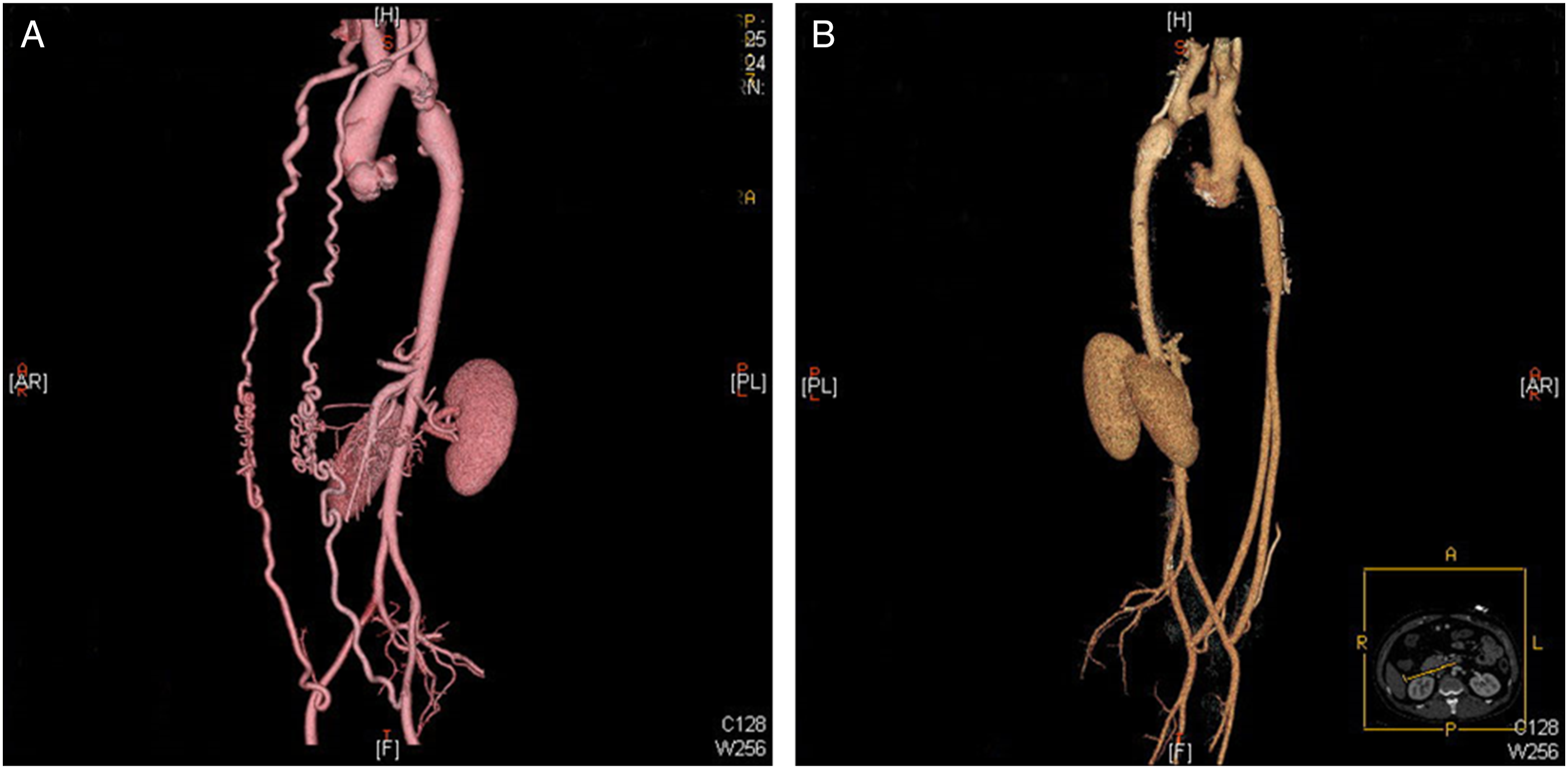
Stenosis or Occlusion of a Graft Branch After Surgery.
Discussion
As most patients with CoA are treated effectively in early childhood, the mortality rate associated with this condition has been reduced to 1-2% and 20-year survival rates are as high as 86.4%.9,10 Unfortunately, this disease continues to remain undiagnosed until adulthood in some patients. Moreover, CoA often coexists with obstructive left heart diseases, which should be evaluated comprehensively. 11 In our study, 56.9% of patients with CoA had concomitant bicuspid aortic valves and 58.8% had concomitant aortic root or ascending aortic dilation. The rates of comorbid cardiac lesions that required repair were similar to those reported in other studies.12,13 Hybrid procedures are emerging as viable options for the repair of various cardiac lesions. These techniques have been proven to minimize the difference in systolic blood pressure between the upper and lower limbs; additionally, no rupture or pseudoaneurysm was found at the site of stenosis and no stent restenosis was observed during midterm follow-up. However, the local anatomy of adult CoA is not always suitable for covered stents. Lesions such as long-segment coarctation (especially in cases with hypoplastic aortic arch), severely calcified stenosis, and multiple aneurysms still require open surgical repair.14-16
To avoid the trauma of a two-stage procedure involving a left thoracotomy, surgeons in our center have performed simultaneous repair of CoA and concomitant cardiac lesions using the ascending aorta to abdominal/thoracic aorta bypass technique. 17 Results of this procedure included a decrease in average systolic blood pressure in the upper limbs from 160 mmHg before surgery to 114 mmHg postoperatively. However, the complexity of this surgical approach has led to longer cardiopulmonary bypass (CPB) time, increased risk for arrhythmia due to placement of the graft in the pericardial cavity, and increased risk for abdominal complications. To address the drawbacks of simultaneous repair, we performed an aortoiliac bypass procedure using a midline incision. We found that our approach can effectively reroute the blood flow, simplify the surgical procedure, avoid cardiac compression caused by the graft, and minimize abdominal organ disturbance, while achieving an efficacy similar to that of the ascending aorta to abdominal/thoracic aorta bypass technique.
The Y-shaped graft must be carefully placed during surgery. The serum exudation from the artificial graft that implanted subcutaneously may cause the subcutaneous fat liquefaction and delayed wound healing. This speculation came from the experience of our center that the first 5 cases implanted percutaneously with one suffering subcutaneous fat liquefaction and delayed wound healing. The reasons for this complication were not clear, which may be related to hemodynamics between ascending aorta and femoral artery and the materials of graft, but further research is needed. Since the abdominal cavity is a larger space with increased absorptive capacity, the grafts in our study were placed intraperitoneally through the subxiphoid sheath. This approach not only improved absorption of extravasations but also eliminated subcutaneous discomfort, improving the patients’ quality of life. Three patients had delayed healing at the site of the abdominal lower quadrant incisions due to local lymphatic leakage; these patients fully recovered after two weeks with drainage. No patients presented with abdominal complications such as bleeding, infection, or bowel obstruction. Additionally, all patients were discharged in stable condition. None of the patients presented with postoperative renal dysfunction, even though antegrade perfusion was used only at ascending aorta during operation with ECC. This may be attributed to the abundant collateral circulation between upper and lower limbs in adult patients with longtime CoA. The ECC time during our one-stage procedure did not increase compared with the bypass procedure we performed previously, 18 suggesting that this modified approach is much safer and more effective.
Graft stenosis or thrombosis is a significant complication, which is closely related to the pathology of the vessel and the vessel patency distal to anastomosis. Ameli et al.19,20 reported a graft occlusion rate of 12% in patients undergoing aortofemoral bypass surgery for iliac occlusive disease. Creating the proximal anastomosis off the ascending aorta may decrease the risk of thrombosis due to higher blood pressure and better blood flow from the ascending aorta. However, six patients (11.8%) in our study developed thrombosis of the graft branch. Previous studies examining patency rates for aortobifemoral bypass have reported that the small graft size and the prosthetic graft material were among the major causes leading to thrombosis.19,21 Antiplatelet or antithrombotic therapy can be administered to ensure long-term graft patency, but the combination of oral anticoagulants (target international normalizing ratio 2-3) and antiplatelet therapy was associated with an increase in life-threatening bleeding.21,22 We suggested post-operative anticoagulation with warfarin treated for at least 3 months, maintaining an international standardized ratio at 2.0–2.5, followed by a regular dose of aspirin.
Tissue engineering blood vessels (TEBV) with rapid development in recent years may be an alternative because autologous endothelial cells that incorporate onto the inner layer of the synthetic graft, which can decrease immune reaction and retain the ability for remodel and patency, are the natural defenders against thrombosis or occlusion in small diameter graft. 23 Although in the one-stage approach we have described that above remains a palliative therapy compared with other procedures, such as the resection and interposition graft technique, our study, indeed, showed some advantages offered by the one-stage repair and patients undergoing this approach need to be closely monitored for long-term outcomes.
Our study has several limitations. First, this study was a single-center descriptive study, lacking an effective control group. Randomized controlled clinical trials are needed, so as to guide the selection of clinical treatment strategies. Second, the sample size of this retrospective analysis was relatively small and the follow-up period is limited. Since the graft from the ascending aorta to the iliac artery is long, with a small diameter, long-term patency of this graft requires further assessment. Finally, bypass surgery does not achieve anatomic correction in CoA patients with post-stenotic dilation or localized dilatation of the aorta. A longer and more comprehensive follow-up is necessary for these patients to monitor for adverse events and determine the need for secondary surgery.
Conclusion
The clinical outcomes of aortoiliac bypass for one-stage repair of CoA with concomitant cardiac lesions are acceptable, which can effectively reduce differences between upper and lower limb systolic blood pressure values. Nevertheless, this approach needs further evaluation, particularly in terms of graft patency and long-term adverse events.
Footnotes
Acknowledgments
The authors would like to thank Iulia Filip for editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.