
Abstract
Traumatic injuries to the mesenteric vessels are rare and often lethal. Visceral vessels, such as the superior mesenteric artery (SMA) and vein (SMV), supply blood to the small and large bowel by a rich system of collaterals. Because fewer than 100 such injuries have been described in the literature, they pose challenges in both diagnosis and management and can unfortunately result in high mortality rates. Prompt diagnosis, surgical intervention, and resuscitation can lead to improved outcomes. Here, we review the literature surrounding traumatic injuries of the SMA/SMV and discuss management strategies.
Introduction
Injury to large intra-abdominal vasculature is uncommon in both blunt and penetrating abdominal trauma. When they do occur, these injuries tend to be highly morbid and management is extremely challenging. This is especially true for injuries to the SMA and SMV. SMA injuries alone can quadruple mortality risk. 1 Overall mortality associated with these injuries remains high due to the technical difficulty involved in exposure, access, and control. In addition, these high capacitance vessels have robust blood flow, so injury leads to early exsanguination, hemorrhagic shock, and multi-organ system failure.2,3 With improvements in trauma response times and pre-hospital resuscitation, more patients with SMA/SMV injuries are surviving long enough to present to a trauma center where their injuries can be identified and managed in a timely manner. Overall, the rate of mesenteric vascular injuries has been increasing. This is likely due to an increased incidence of high velocity motor vehicle collisions with seat belt use, as well as enhanced pre-hospital survival and improved imaging protocols. 4 Unfortunately, most data regarding outcomes is derived from small case series and there are no universally applicable guidelines for operative, non-operative, or endovascular therapies. 4 This review presents a contemporary review of the literature regarding SMA and SMV injuries including strategies for diagnosis, workup, and management.
Historical Perspective
Traumatic SMA Injuries Series Summary.
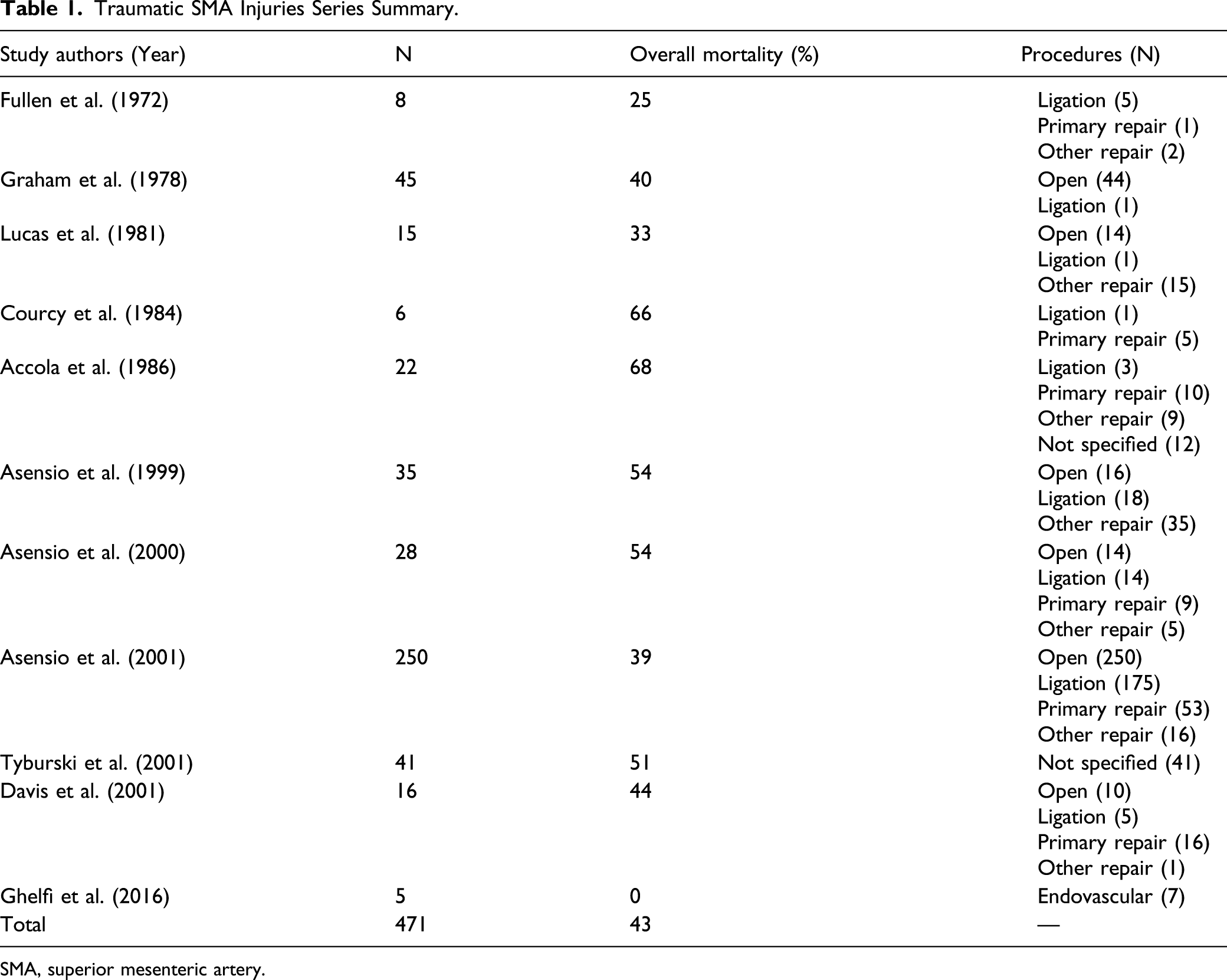
SMA, superior mesenteric artery.
Traditional management of abdominal vascular trauma centered on immediate operative repair. Outcomes of early case series were grim with mortality approaching 50%. Literature in the second half of the 1970s and throughout the 1980s investigated ligation as a way to prevent exsanguination while accepting the sequelae of ischemia. Though ligation remained the most common surgical treatment through the end of the 20th century, outcomes were consistently poor. Therefore repair, whenever possible, continues to be recommended. 7 Repair with autologous vein or synthetic graft materials such as Dacron or polytetrafluoroethylene (PTFE) saw limited use and was met with largely unfavorable outcomes. 7 Overall, there is a relative dearth in studies regarding operative management of SMA injuries with the most recent studies published in 2001–2002. 4
The modern tenants of trauma surgery include damage control laparotomies and focus on correction of “The Lethal Triad” over definitive repair. 8 These ideas led Feliciano, Rotondo, and others to support damage control with a planned “second look” for intra-abdominal vascular trauma. This included the use of temporary SMA shunts by Reiley et al in 1995.8–10 Animal model experimentation in 2010 demonstrated promising data with temporary vascular shunts limiting ischemia time. 11 These principles were originally described over a century ago, particularly in military theaters, and even today in the damage control setting, shunting may be the most prudent option.12,13 Still, more contemporary studies have also shown endovascular interventions to be a potentially efficacious adjunct to delayed repair surgery.
Traumatic SMV Injuries Series Summary.
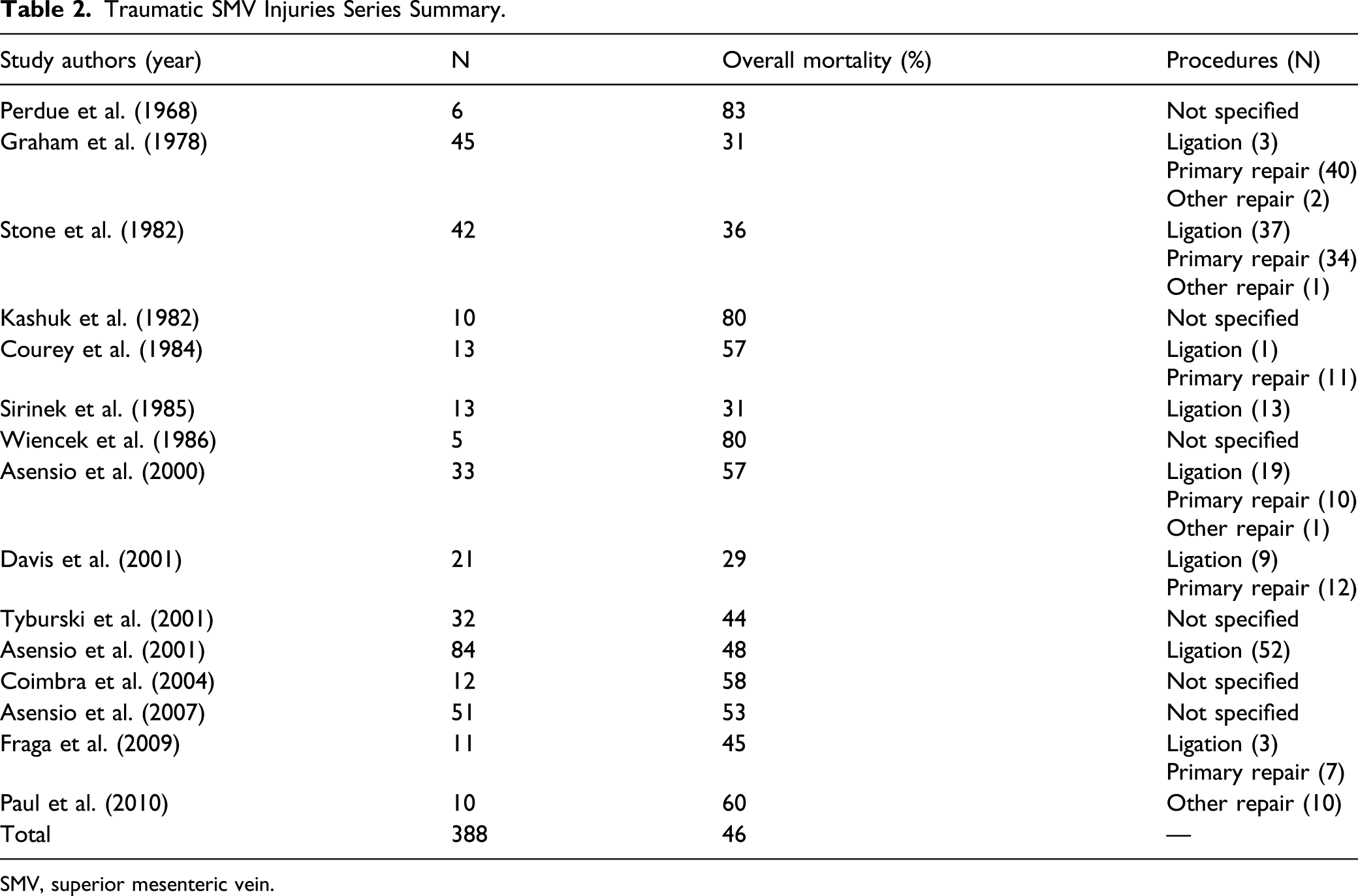
SMV, superior mesenteric vein.
Incidence
The incidence of SMA injuries is historically reported to be less than 1% of all trauma center admissions. 18 A recent query of the Trauma Quality Improvement Program (TQIP) by Maithel et al showed the incidence of a single visceral injury to be .12% of all trauma admissions and SMA injuries were 51.4% of those injuries. 19 20 years ago, penetrating trauma was the major cause of SMA injury with incidence ranging from 67–91%. 5 The percentage of blunt SMA traumatic injuries has increased over time from 12–24% 20 years ago to 64% between 2010 and 2016. 19 In contrast, the incidence of penetrating SMA trauma has decreased over time and now represents only 35% of cases. 19 It has been postulated that the institutionalization of massive transfusion protocols and expedited pre-hospital transport times has improved prehospital survival of blunt SMA injuries. 20
Anatomy
Knowledge of vascular anatomy is always important for surgical decision making following traumatic injury. The SMA provides blood flow to the entire midgut (small bowel) and the proximal portions of the hindgut, including the right colon, appendix, and proximal two-thirds of the transverse colon by way of its middle colic artery branch.
21
The SMA arises directly off of the aorta distal to the celiac trunk within the retroperitoneum (Figure 1). During a laparotomy, the SMA can be palpated by lifting the transverse colon cephalad and tracing down to the root of the mesentery near the ligament of Treitz. The right colic and ileocolic arteries originate distal to the middle colic artery and supply the right colon and appendix, respectively. Zones of injury to the superior mesenteric artery.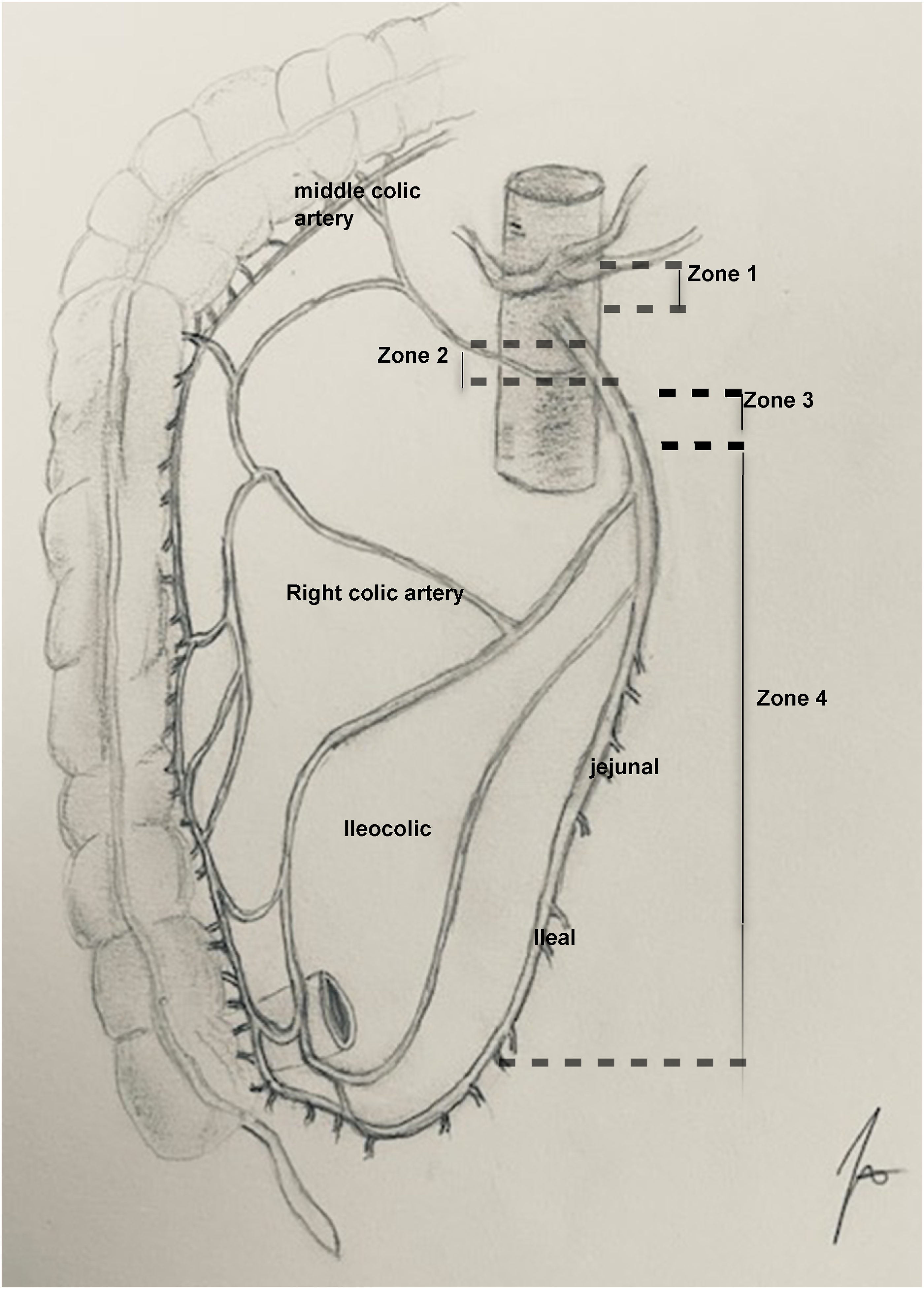
Superior Mesenteric Artery Injury and Ischemic Bowel Risk.
The SMV acts as the primary conduit for venous blood return from the abdominal viscera and joins with the splenic vein to form the portal vein. The portal vein therefore receives all non-hepatic intraperitoneal visceral venous return prior to the entering the liver at the porta hepatis. The first-order branches of the SMV are the ileal and jejunal branches, which can course either directly anterior or posterior to the SMA. While some anatomic variation exists, the SMV also drains blood from the ileocolic, right colic, and middle colic veins. 23 Dissection of these structures can be tedious even in non-emergent situations, such as elective pancreaticoduodenectomy, and again underscores the fact that thorough anatomic knowledge is an important part of surgical management.
Clinical Presentation
Historically, the majority of superior mesenteric vessel injuries were devastating with mortality rates as high as 53–71% as reported by Asensio et al 5 With advancements in pre-hospital care, standardization of trauma management, and improved blood transfusion protocols, we have seen an increase in the survivability of these injuries. This has also provided us with more information about clinical presentation. 19
The major causes of blunt injury to the superior mesenteric vessels are from rapid deceleration mechanisms such as with motor vehicle collisions, seat belts injuries, and posterior crush injuries to the spine. 24 The most common nonvascular injuries associated with blunt superior mesenteric vessel trauma are small bowel injuries followed by colorectal and then liver injuries, respectively. 19
Penetrating abdominal injuries normally cause destruction of the tissue along its trajectory but can also have circumferential blast effects as seen in gunshot injuries. Similar to blunt injuries, the most common associated nonvascular injury is the small intestine followed by colorectal, liver, and pancreatic injuries. Associated pancreatic injuries are as high as 21% in penetrating injuries compared to 7.6% in blunt injuries. 19
Arterial injury may generally be stratified to 1 of 4 grades as proposed by Biffl. Grade I, intimal irregularity with <25% narrowing; Grade II, dissection or intramural hematoma with >25% narrowing; Grade III, pesudoaneurysm; Grade IV, occlusion; Grade V, transection/rupture with extravasation. 25
Both blunt and penetrating trauma can present in a varied fashion. The most minor injury, an intimal tear (Figure 2), can present with abdominal pain secondary to thrombosis.
26
Intimal tears can occur primarily or secondary to blast effects. These intimal flaps can progress to bowel ischemia and delayed perforation requiring operative intervention. These patients normally present hemodynamically stable and remain that way until ischemia occurs. Such tears can initially be treated with aspirin to help stabilize the area of the flap with later imaging to evaluate healing or progression.
27
Computed tomography imaging findings of a superior mesentery artery flap on axial (A) and sagittal (B) views.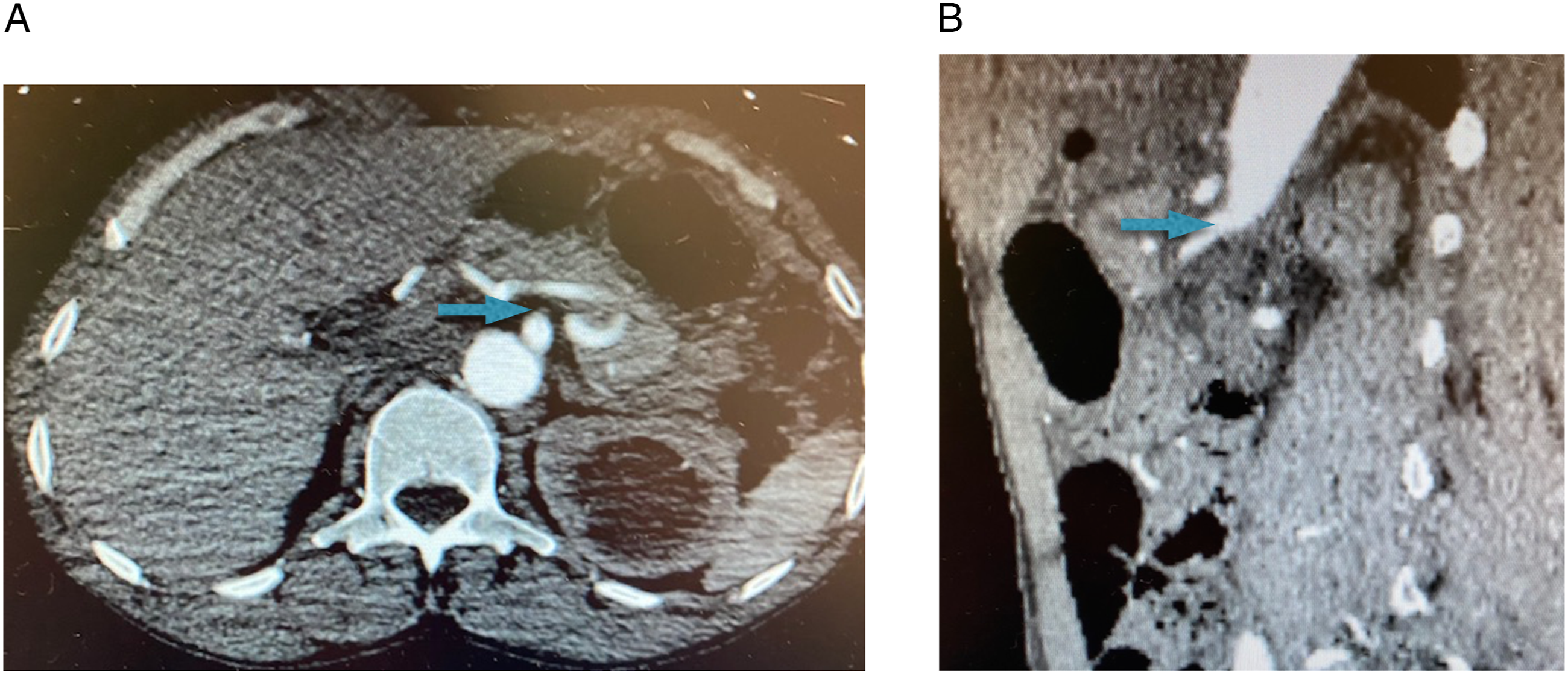
One of the most common intraoperative findings from traumatic vascular injuries is a retroperitoneal hematoma, which is reported in up to 96% of cases. 28 This can be a pulsatile hematoma from a tear in the arterial wall or a non-pulsatile hematoma from a venous injury. Patients respond initially to resuscitation but become hemodynamically unstable once the hematoma is evacuated in the operating room, classifying them as “transient responders.”26,29 When the entire vessel is transected or avulsed, there is free intraperitoneal hemorrhage. These patients present hemodynamically unstable and are unresponsive to resuscitation classifying them as “non-responders.”7,27 They require immediate operative intervention.
The least common presentation of a SMA injury is a pseudoaneurysm, which occurs less than 1% of the time. 28 These can present either as a ruptured or non-ruptured pseudoaneurysm. Non-ruptured pseudoaneurysms are typically discovered incidentally on follow-up imaging while ruptured pseudoaneurysms present days after initial presentation with sudden acute change in hemodynamics with or without abdominal distension. Such grades III injuries may be amenable to endovascular management depending on the patient’s hemodynamic status. 27
If clinically stable, multi-detector row computed tomography (MDCT) is the imaging modality of choice given its ability to identify active contrast extravasation from an injured vessel or intimal tears. Improved imaging capabilities have increased the detection of clinically silent vascular injuries. 30 Focused abdominal sonography for trauma (FAST) is useful in blunt abdominal trauma for identifying hemoperitoneum but is not useful for identifying certain mesenteric injuries, especially if retroperitoneal. 28
Surgical Management
Superior Mesenteric Artery Injury
Patients with SMA injuries often present to the hospital in hemorrhagic shock that ultimately necessitates operative intervention following initial resuscitation. Since isolated SMA injuries following penetrating or blunt trauma are rare, the astute trauma surgeon should always consider that concomitant injuries could affect patient physiology. Optimal resuscitation with blood products in balanced 1:1:1 fashion with close monitoring of hemodynamic status is paramount. Strategies for management of SMA injuries include primary repair, shunting, endovascular therapy, or as last resort, ligation. Due to the risks of ischemia, ligation should be a last resort and only considered for more distal injuries. The first step for approaching SMA injuries is exposure, followed by obtaining proximal and distal control. A generous midline laparotomy incision from xyphoid to pubis is made. Exposure of the SMA or SMV is best achieved by a left medial visceral rotation (Mattox Maneuver). The left white line of Toldt is incised and the viscera is rotated medially to expose the abdominal aorta, the ostia of the celiac trunk, SMA, and left renal artery. Because hemorrhage control relies on proximal and distal control, additional exposure or mobilization may be needed. A left anterolateral thoracotomy may be necessary to obtain proximal control of the aorta in the chest. From the abdomen, mobilizing the left lobe of the liver and exposing the right crus of the diaphragm can allow aortic cross-clamping. Once vascular isolation is obtained, the surgeon can define the extent of the injury and plan the repair. This may not be possible for patients presenting in extremis. A damage control approach provides provisional control of hemorrhage and gastrointestinal spillage with temporary closure of the abdomen. These patients will receive further resuscitation prior to definitive laparotomy and repair.31,32 Temporary shunting of the SMA was first described by Reilly in 1995 and can be lifesaving in these situations. 31 Continued bowel perfusion is gained and allows time for resuscitation, treatment of other life-threatening injuries, or even transfer to a more suitable facility. 33 Temporary abdominal closure also allows for serial examination of bowel and further resections if required. 34
Insertion of a temporary intravascular shunt (TIVS) in pig models of SMA injury was associated with improved mortality compared to primary repair. 35 Randomized to 4 different time groups, pigs who were shunted for up to 6 hours did not experience any occlusion of the shunt and had reversible intestine ischemia-reperfusion injuries. Conversely, shunting between 9 and 12 hours produced 50% and 100% occlusion rates, respectively, with higher rates of intestinal necrosis. 35 Further investigations demonstrated that longer shunt times are associated with increased endothelial injury from the physical placement of the shunt. 36 Based on this data, in cases of shunting, transected portions of the artery that have come into contact with the shunt should be evaluated for intimal injury prior to interposition graft placement. 36 In the case of SMV injuries, or concomitant SMA/SMV injuries, venous shunting is also possible and has been shown to be useful in austere conditions, such as wartime. 14
When length of the vessel injury is fairly minimal or the injury encompasses <50% of the lumen diameter, an attempt at primary repair may be considered if there is no significant intimal injury.
37
This can be done with interrupted 5-0 or 6-0 polypropylene suture, closing the arteriotomy transversely to decrease risk of stenosis. Primary anastomosis of transected arteries has a substantial risk of thrombosis; however, as demonstrated by Lucas et al, 67% of primarily repaired SMAs have been shown to thrombose.
38
In cases of primary failure, interposition grafts using reversed saphenous veins or PTFE may be required.
28
Autologous grafts are commonly preferred over synthetic grafts due to the infectious risk from gastrointestinal spillage in the operative field. Synthetics remain a viable option as well if contamination is minimal or other factors preclude the use of autologous grafts.
33
Figure 3 demonstrates the use of a synthetic graft to repair a combined aortic and superior mesentery artery injury reconstruction following a gunshot wound to the abdomen. Combined aorta and superior mesentery artery injury with reconstruction.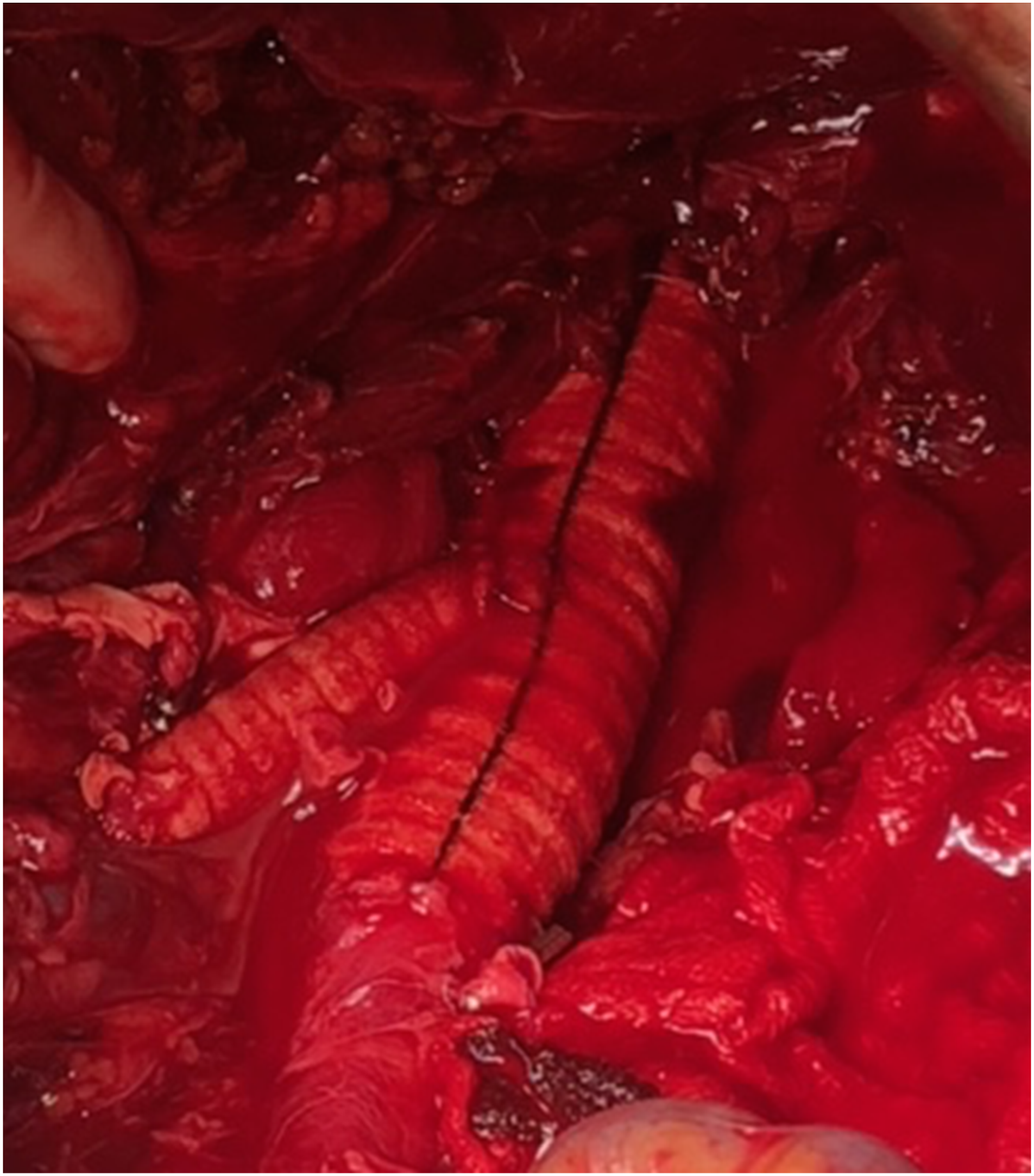
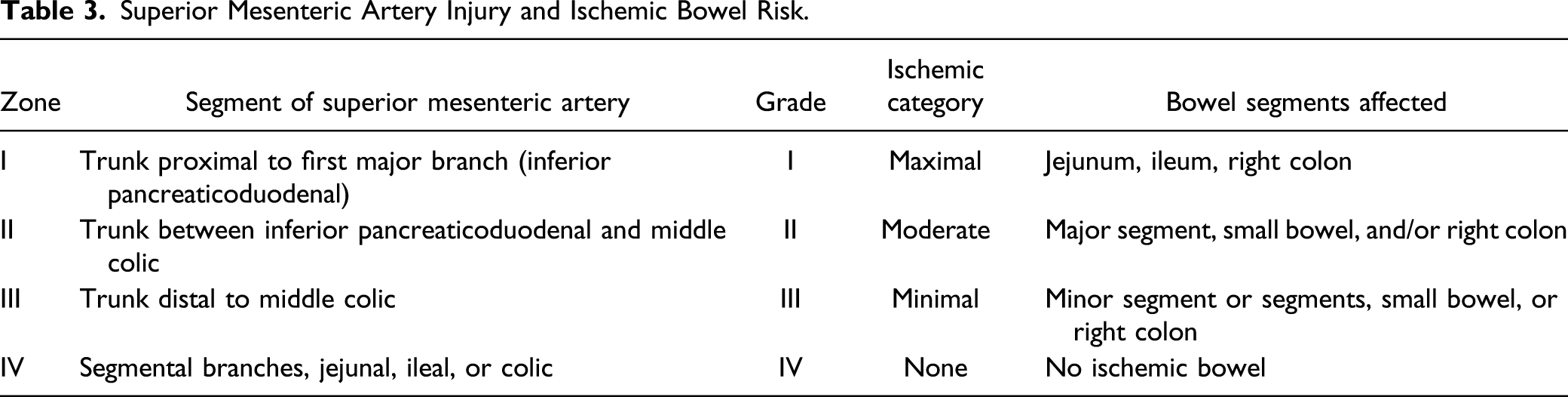
If technically feasible, injuries of the SMA should always be repaired. 39 In exsanguinating patients however, ligation may be a last resort. The exact location of the injury defines the extent of bowel necrosis. Ligation of the SMA in zones I and II of the Fullen classification may result in extensive necrosis if collateral flow from the celiac trunk and inferior mesenteric artery (IMA) are limited. 18 More distal ligation in zones III and IV are likely to be better tolerated due to the rich collateral network of the cascades. Whenever ligation is performed, second-look laparotomy should be planned because sequential bowel resection may be requried. 33
Endovascular interventions can be advantageous because they are minimally invasive, effective, and fast, but are only appropriate in hemodynamically stable patients. 37 Rarely, SMA embolization is necessary following interval and remote presentation of bleeding. As with operative ligation, this can lead to bowel ischemia and necrosis and a second-look laparotomy is warranted. The overall clinical picture of the trauma patient will determine the most optimal approach. Another adjunctive measure is the use of the resuscitative endovascular balloon occlusion (REBOA). Although this aortic occlusion can temporarily control massive hemorrhage, its use is associated with many complications, so widespread adoption is limited. 40 Hybrid “RAPTOR” (Resuscitation with Angiography Percutaneous Treatments and Operative Resuscitations) operating rooms with full angiographic capabilities may offer the ideal procedural environment for management of these complex injuries. 41
Superior Mesenteric Vein Injury
Although SMV injuries occur in conjunction with SMA injuries in 34–50% of the time, isolated injuries are rare.28,42 Both concomitant and isolated injuries are rare and only 300–400 cases have been described in the literature. These are associated with greater than 40–50% mortality. 24 As with SMA injuries, patients with SMV injuries often present in hemorrhagic shock and frequently have other life-threatening intra-abdominal injuries. For both of these reasons, meticulous vascular repair of SMV injuries is often not optimal. Furthermore, robust collateral flow usually exists by way of the portosystemic and inferior mesenteric venous branches. Unless primary repair is relatively simple and mitigating factors are few, ligation is usually the option of choice. Several reports have demonstrated this to be a safe option and the majority of patients who undergo ligation survive. 43 This option is not without consequence, however. Severe bowel edema can occur before the development of adequate collateral circulation. 43 In severe cases, complications such as bowel ischemia and necrosis can result. Rarely, systemic hypotension and splanchnic hypertension syndrome can occur. 44 Gastrointestinal function should be closely monitored post-operatively with serial clinical exams and radiographic assessments. Although a few isolated case reports describe successful SMV revascularization through saphenous vein bypass shunts or splenic vein turndown, this is rare and occurs in high volume centers with the assistance of experienced vascular surgeons.45–47
Outcomes and Mortality
The American Association for Surgery of Trauma Organ Injury Scale (AAST-OIS) is the current guideline for defining abdominal vascular injuries. 48 SMA unnamed branch injuries are considered Grade I, named branches are Grade II, injuries distal to the middle colic are Grade III, and SMA trunk injuries are considered Grade IV. As expected, mortality increases with increasing grade and Grades IV injuries predict mortality as high as 76.5%. 28
In addition to the AAST-OIS, Fullen zones I and II injuries correlate with mortality and have been shown to be an independent risk factor for mortality. According to Asensio et al, isolated SMV injuries conferred a mortality rate of 47–57%. 5 Similarly, the mortality rate of isolated SMA injuries is 53.6%. 44 Strangely, combined SMV and SMA injuries have slightly lower mortality rates of 43–45%.5,44 This is thought to be due to decreased pre-hospital survival. Recent literature has shown that overall mortality from these injuries has drastically dropped. The 2010–2016 mortality rates for blunt and penetrating SMA injury was reported to be as low as 19.4% and 31.9%, respectively. 19 One multi-institutional study determined that independent risk factors for mortality include intraoperative acidosis, dysrhythmias, multisystem organ failure, and age greater than 55. 28
Outcomes have improved over the last 20 years for many reasons. First, the development and validation of damage control resuscitation has decreased in-hospital mortality within the first 6 hours of admission following hemorrhagic shock, especially in blunt trauma, as noted by Dente el al.49,50 Another major factor in the improved outcomes of SMA injuries is the use of endovascular therapy. Branco et al compared outcomes between matched patients who underwent endovascular and open procedures from 2002–2010 and found that endovascular procedures had a significantly lower in hospital mortality vs open procedures of 12.9% vs 22.4%, respectively. When early deaths were excluded, endovascular therapy remained significantly lower than open, 8.9% vs 12%, respectively. 51
In some large trauma centers across the country, hybrid operating rooms have been created offering multiple therapies all in one location. These multi-modality rooms are designed to treat patients in hemorrhagic shock and have the ability to perform whole body imaging, endovascular procedures, and open surgical procedures. Such operative suites could increase the use of early endovascular therapy as an adjunct for these injuries. This is important because recent data shows a possible temporal relationship between increased survivability and endovascular procedures. 51
REBOA has been used as an adjunct for hemorrhagic control of the aorta in the setting of blunt abdominal trauma and hemodynamic instability. However, recent data shows that when matched to patients who did not have a REBOA, patients who underwent REBOA placement had higher mortality rates. 52 Given this data, more studies need to investigate the efficacy of REBOA for abdominal vascular injuries.
Another factor affecting outcomes after an SMA injury is lack of collateral circulation as compared to celiac artery (CA) and IMA circulation. This lack of collateral flow means that the bowel supplied by the SMA is highly susceptible to ischemia. Unfortunately, bowel ischemia may not declare itself until several hours following injury. 38 For this reason, SMA injuries have much higher mortality compared to CA and IMA injuries with an almost four-time increased risk for mortality in adult penetrating trauma specifically. 19 It is imperative to perform a delayed inspection for bowel viability in SMA injuries. Second look laparotomy improves patient survival and preserves bowel length.
Limitations of this study include the inherent nature of retrospective review as well as the reliance on potentially incomplete data from trauma registries and other systematic reviews. Furthermore, it is difficult to compare data on specific technical aspects of injury management, for example, outcomes on vein conduit vs other grafts, given the wide range of cases, study designs, and individual outcomes.
Conclusion
Injuries to the visceral vessels are rare events with daunting mortality rates. It is important to have both detailed vascular anatomic knowledge and global awareness of the patient’s physiologic status and trauma burden. These types of vascular injuries are often associated with severe polytrauma that compound patients overall morbidity and mortality. Survival following injuries to the SMA or SMV depends on coordinated trauma teamwork, aggressive resuscitation, and early operative intervention.
Footnotes
Author Contributions
All authors contributed to the journal review, creation, and editing of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.