
Abstract
Keywords
A 27-year-old-woman presented with a history of progressive, intermittent abdominal pain for four months, with increased severity in last one week. The patient gave history of retrievable inferior vena cava (IVC) filter implantation as part of management of post-partum lower-extremity deep venous thrombosis four years back. The filter had not been retrieved till date.
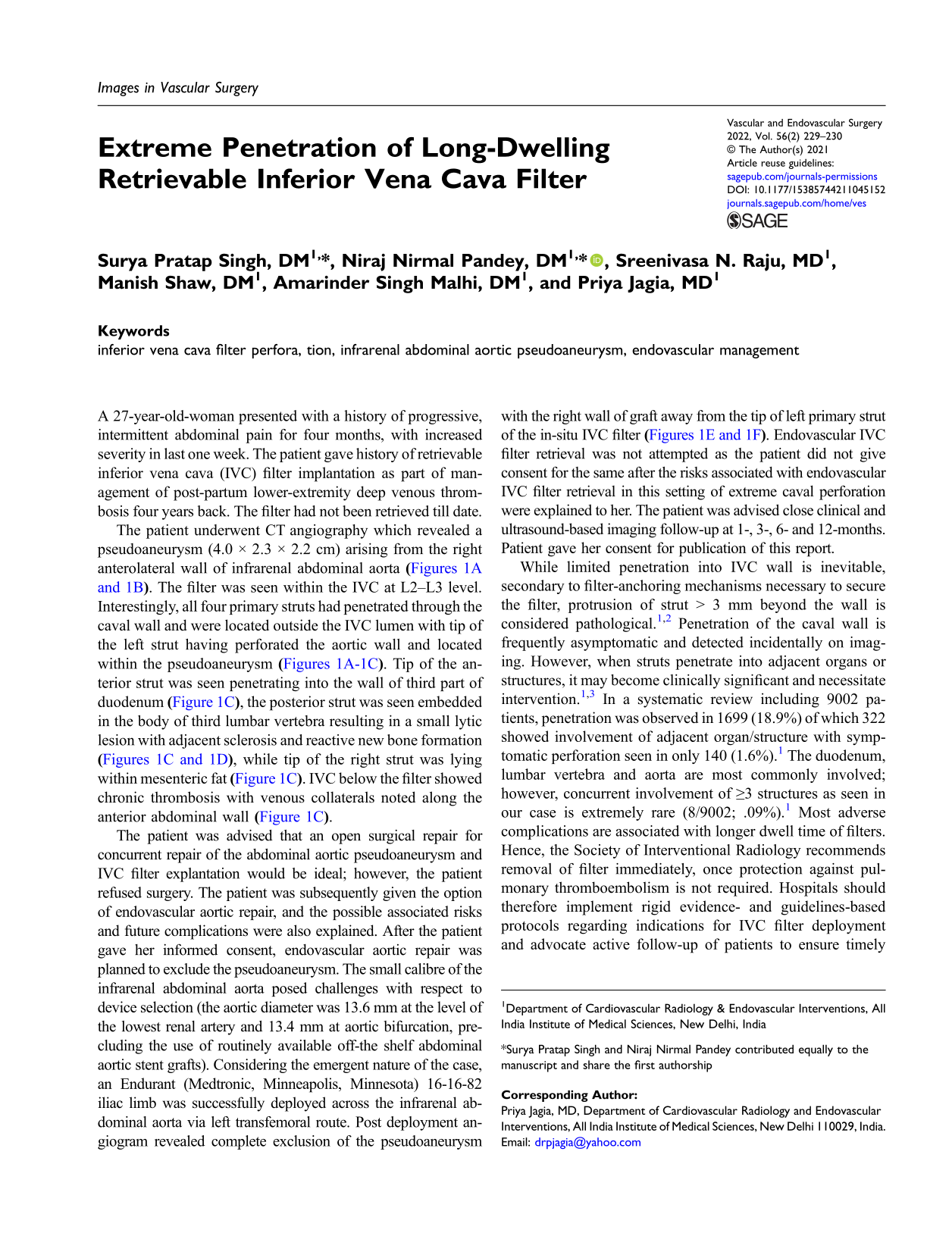
The patient underwent CT angiography which revealed a pseudoaneurysm (4.0 × 2.3 × 2.2 cm) arising from the right anterolateral wall of infrarenal abdominal aorta Volume rendered images 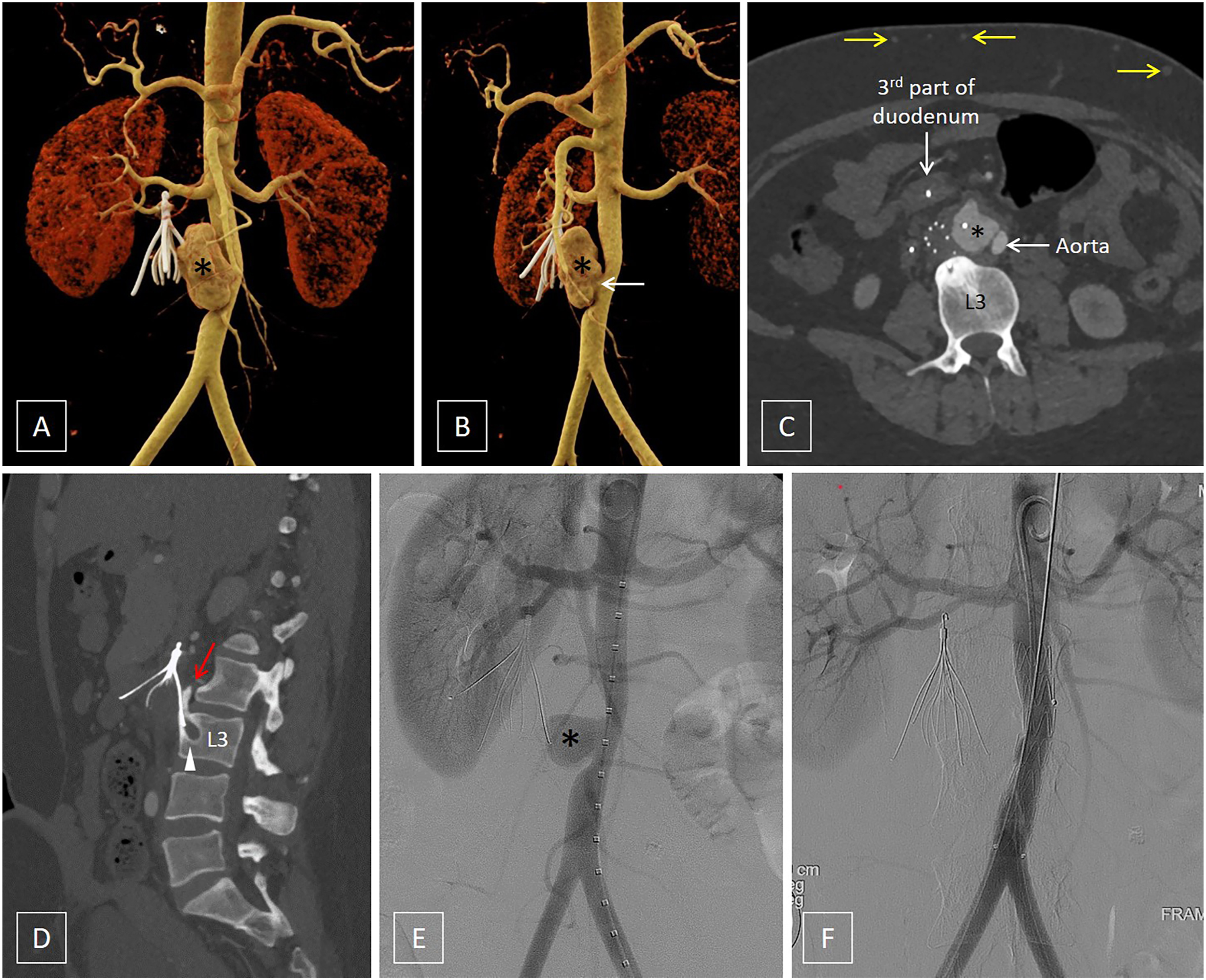
The patient was advised that an open surgical repair for concurrent repair of the abdominal aortic pseudoaneurysm and IVC filter explantation would be ideal; however, the patient refused surgery. The patient was subsequently given the option of endovascular aortic repair, and the possible associated risks and future complications were also explained. After the patient gave her informed consent, endovascular aortic repair was planned to exclude the pseudoaneurysm. The small calibre of the infrarenal abdominal aorta posed challenges with respect to device selection (the aortic diameter was 13.6 mm at the level of the lowest renal artery and 13.4 mm at aortic bifurcation, precluding the use of routinely available off-the shelf abdominal aortic stent grafts). Considering the emergent nature of the case, an Endurant (Medtronic, Minneapolis, Minnesota) 16-16-82 iliac limb was successfully deployed across the infrarenal abdominal aorta via left transfemoral route. Post deployment angiogram revealed complete exclusion of the pseudoaneurysm with the right wall of graft away from the tip of left primary strut of the in-situ IVC filter
While limited penetration into IVC wall is inevitable, secondary to filter-anchoring mechanisms necessary to secure the filter, protrusion of strut > 3 mm beyond the wall is considered pathological.1,2 Penetration of the caval wall is frequently asymptomatic and detected incidentally on imaging. However, when struts penetrate into adjacent organs or structures, it may become clinically significant and necessitate intervention.1,3 In a systematic review including 9002 patients, penetration was observed in 1699 (18.9%) of which 322 showed involvement of adjacent organ/structure with symptomatic perforation seen in only 140 (1.6%). 1 The duodenum, lumbar vertebra and aorta are most commonly involved; however, concurrent involvement of ≥3 structures as seen in our case is extremely rare (8/9002; .09%). 1 Most adverse complications are associated with longer dwell time of filters. Hence, the Society of Interventional Radiology recommends removal of filter immediately, once protection against pulmonary thromboembolism is not required. Hospitals should therefore implement rigid evidence- and guidelines-based protocols regarding indications for IVC filter deployment and advocate active follow-up of patients to ensure timely removal of retrievable IVC filters, once the indication for IVC filter is no longer there.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.