
Abstract
Background
It is well accepted that good muscle coverage of the bones at the end of a below knee amputation (BKA) stump is preferable, for both weight bearing and protection against prosthesis failure. Elderly patients often have atrophy of the leg musculature secondary to age-related physiological changes and decreased use. These patients often have poor coverage and bulk in their stumps after the standard BKA. We propose a selective muscle-sparing approach to these patients, utilizing selective removal of muscle bundles with regard to their blood supply and fascial planes. The surgical method technique along with outcomes of patients undergoing the procedure is presented here.
Methods
A retrospective chart review was performed to identify patients who had undergone a muscle-sparing BKA from March 2008 to October 2017 by a single surgeon. Estimated blood loss, operative time, and perioperative and postoperative complications were assessed.
Results
Forty-six patients greater than 60 years of age underwent muscle-sparing BKA procedures. Complete healing was seen in 30 (65%) patients, while 7 (15%) were lost to follow-up and 9 (20%) required conversion to an above knee amputation (AKA). Intraoperative outcomes in our series were notable for an average estimated blood loss (EBL) of 84.3 ml, lower than the traditional BKA (average EBL 150-500 ml), with comparable operative times averaging 131 minutes and as short as 85 minutes (skin incision to dressing). No patients in the cohort required postoperative blood transfusions (day 0–4), significantly less than the reported 3–7 ml/kg body weight blood requirements in similar patient populations.
Conclusions
The muscle-sparing BKA technique should be considered in elderly patients, where the normally bulky posterior calf muscle mass is lacking. The selective removal of muscle bundles with regard to their blood supply leaves maximum coverage of the bone with decreased potential hematoma formation and blood loss.
Keywords
Introduction
Above the ankle, there are 2 main amputations performed today, the above knee amputation (AKA) and the below knee amputation (BKA). BKA, which includes preservation of the knee joint, is the preferred amputation, allowing a better chance of achieving successful ambulation when compared to an AKA.1,2 It is well accepted that good muscle coverage of the bones at the end of a below knee amputation stump is preferable for both weight bearing and protection against prosthesis failure.1,2 Many age-related physiological changes occur in the elderly population, resulting in atrophy and decreased muscle tone throughout the body. This effect is compounded by decreased mobility and reduced muscle use observed in elderly patients. This translates to poor coverage and bulk in amputation stumps after the standard BKA, more specifically in formation of the posterior flap.3-5 The amputation knife is passed behind the tibia and fibula through the posterior compartment without regard to the individual muscle bundles and their respective blood supply. This leaves a large, raw, bleeding muscle surface prone to hematoma formation in a flaccid, non-bulky stump. The traditional BKA technique manages to leave plenty of muscle to cover the bones in younger, healthier individuals but often does not leave adequate stump coverage in elderly.
We propose a selective muscle-sparing approach to these patients, leaving most of the calf musculature for maximum coverage of the bones with an additional benefit of comparatively decreased estimated blood loss in a population often with concomitant anemia and multiple comorbidities.
Technique
A standard 2/3–1/3 skin incision is made 1 handbreadth below the anterior tibial tuberosity (posterior flap 1/3 the circumference of the leg). The posterior flap is “fanned” to accommodate the additional bulk (Figure 1A). The fascia is incised leaving an additional 1cm, for tension-free closure. The anterior skin and fascia are then peeled off down to the ankle level using electrocautery (Figure 1B). The anterior tibias muscle is then selectively excised with electrocautery, at the level of the fascia and eventual cut tibia (if the flap muscles are extremely atrophied even this is spared) (Figure 1C). The tibia is isolated and transected with a Gigli saw, leaving a 45-degree beveled on the anterior tibial edge. The tibia is then again transected just above the ankle, and the tibial bone was removed completely. The fibula is then isolated by dividing the fascia between the peroneus and extensor digitorum longus muscles, and the fibula is then transected with a bone cutter above the level of the tibia. A rongeur is then used to remove any sharp edges from the fibula. The knee is then bent, and the fibula is pulled out after releasing it from its proximal attachments. Taking care to avoid the perineal and posterior tibial vasculature close by, the fibula is mobilized down its length to the ankle using a combination of electrocautery and periostial stripping with gauze. The fibula is then again transected above the ankle and removed (Figure 1D). The posterior flap, skin, and subcutaneous tissues are then incised in a broad curve (Figure 1E). The muscles are then each transected at a 45-degree angle to the skin. The leg is then passed off. The posterior flap with all the muscle is then rotated anteriorly to determine whether any additional muscle needed to be removed to allow a tension-free closure. The nerve is transected obliquely and allowed to retract but occasionally required a small suture of its feeding vessel. After hemostasis is obtained, the posterior flap is then approximated using interrupted 2-0 Vicryl sutures, leaving no gaps in the fascia. The skin is then closed using interrupted 2-0 vertical mattress nylon sutures (Figure 1F). A single layer of Adaptic (non-adhesive petroleum jelly impregnated gauze) is placed across the incision, followed by “fluffed” gauze around the flap. Finally, a 6-inch Kerlix is applied followed by a 6-inch ACE wrap. (A) Marking of “fanned” posterior flap, (B) electrocautery used to peel the anterior leg skin and fascia down to the level of the ankle, (C) electrocautery used to selectively excise the anterior tibias muscle, (D) fibula transected above the ankle and removed, (E) broad curve incised posterior flap, skin, and subcutaneous tissues, and (F) skin closure with interrupted 2-0 vertical mattress nylon sutures.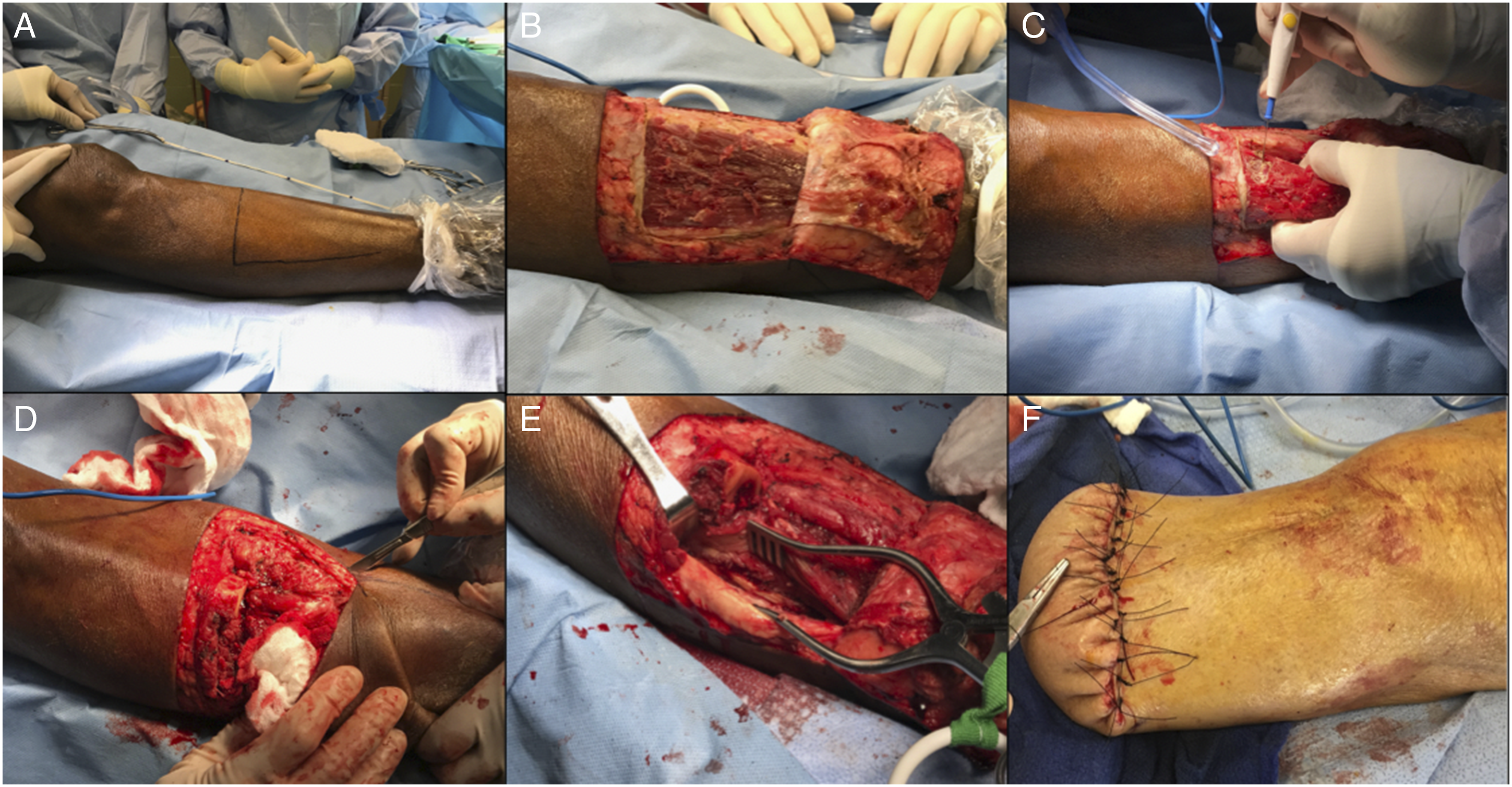
Methods
A retrospective chart review was performed to identify patients who had undergone a muscle-sparing below knee amputation from March 2008 to October 2017 by a single surgeon. Estimated blood loss, operative time, and perioperative and postoperative complications were assessed.
This study consists of two populations from separate institutions, one from an IRB exempt database and another that received IRB approval.
Results
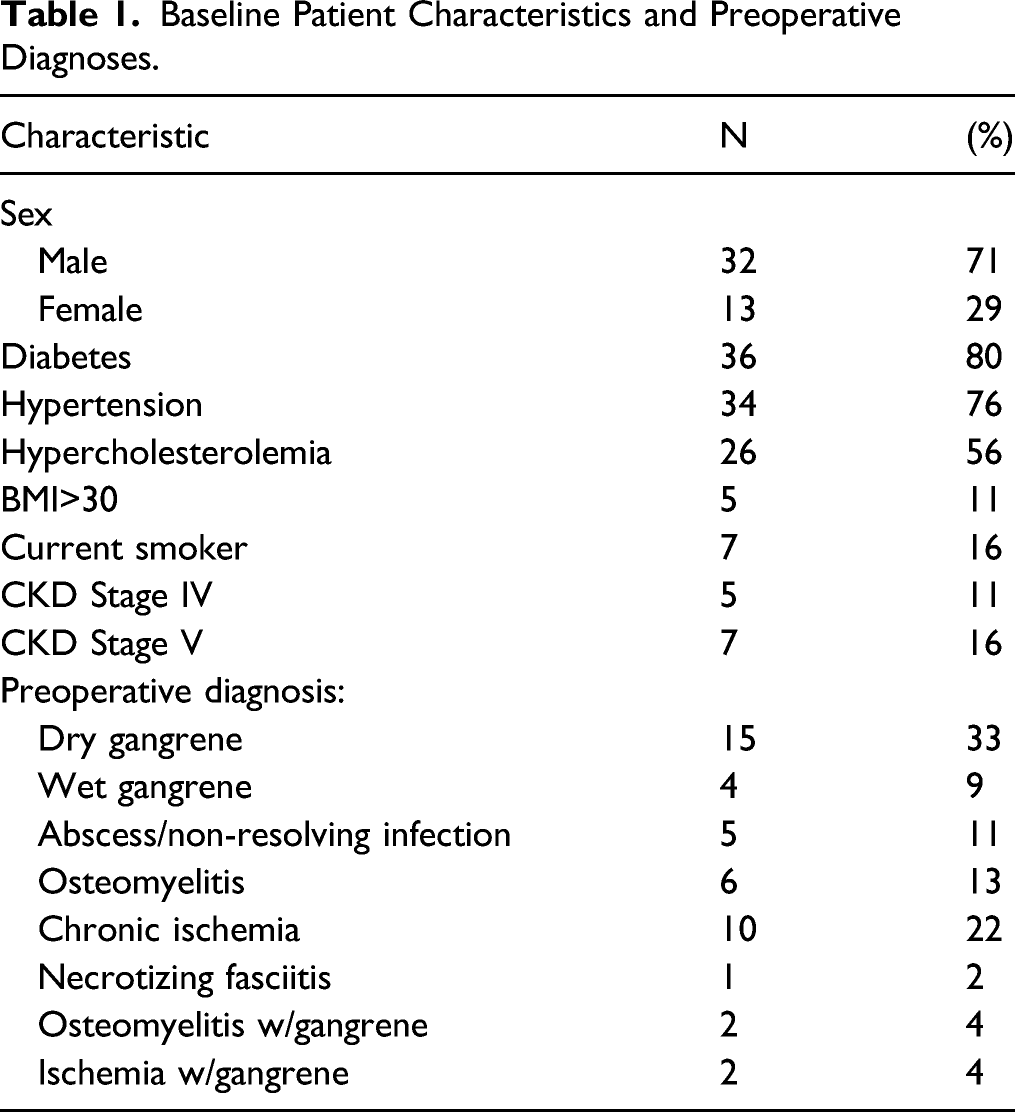
Baseline Patient Characteristics and Preoperative Diagnoses.
Complete healing was observed in 30 of 46 (65%) patients. The average days to complete healing of the stump was 66.6 ± 64.9 days with 19 (66%) of the 30 patients healed in less than 60 days
Discussion
In the United States, approximately 130,000 amputations are performed each year and about 1 in 300 people (over 1 million people) are living with lower limb loss.7,8 Walking requires additional skill, strength, and energy for any person with lower limb amputation.1,2 Due to other comorbidities and health conditions, elderly patients face more challenges with walking and other physical activities after the lower limb amputation.9,10
A significant inverse relationship existed between stump length and energy expenditure measured during ambulation. 11 Moreover, physicians and prosthetists have generally credited longer stump lengths with specific advantages that include longer lever arm, greater muscle capacity, and greater load bearing capability. 11 Therefore, during the amputation, it is important for a surgeon to preserve as much well vascularized muscle as possible to cover the bone. This provides a good weight bearing surface for a prosthesis, especially in elderly population where muscle atrophy and flaccidity are a concern.
The benefits of a muscle-sparing below knee amputation in the elderly population have not been discussed broadly in recent literature. Most of the literature focuses on various flaps such as gastrocnemius transposition flap, muscle transpositions over the tibia, and free myocutaneous flaps for preserving below knee amputation stumps. It is well accepted that good muscle coverage of the bone at the end of the BKA stump is preferable.
The standard BKA routinely removes most of the legs muscle mass, routinely leaving only the soleus muscle and gastrocnemius muscle tendon (Figure 2). In a younger, healthier individual, this technique manages to leave plenty of muscle bulk to cover the bone end. Elderly patients, however, often have poor calf musculature from age and decreased use. The standard BKA does not take this decreased muscle bulk into consideration in the formation of the posterior flap. The standard BKA can often leave a flaccid, thin flap with poor muscle bulk to protect the skin from the bone. The amputation knife is passed behind the tibia and fibula through the posterior compartment during a routine BKA, regardless of the individual muscle bundles and their blood supply. This leaves a large, raw, bleeding muscle surface, which in a non-bulky stump would be more prone to hematoma formation. With high incidence of comorbidities, including peripheral vascular disease, observed in the subset of patients receiving BKA’s, these patients have cannot afford to disrupt important collaterals to the remaining musculature. Cross sectional and lateral illustration highlighting preserved musculature and typical location of a below the knee amputation.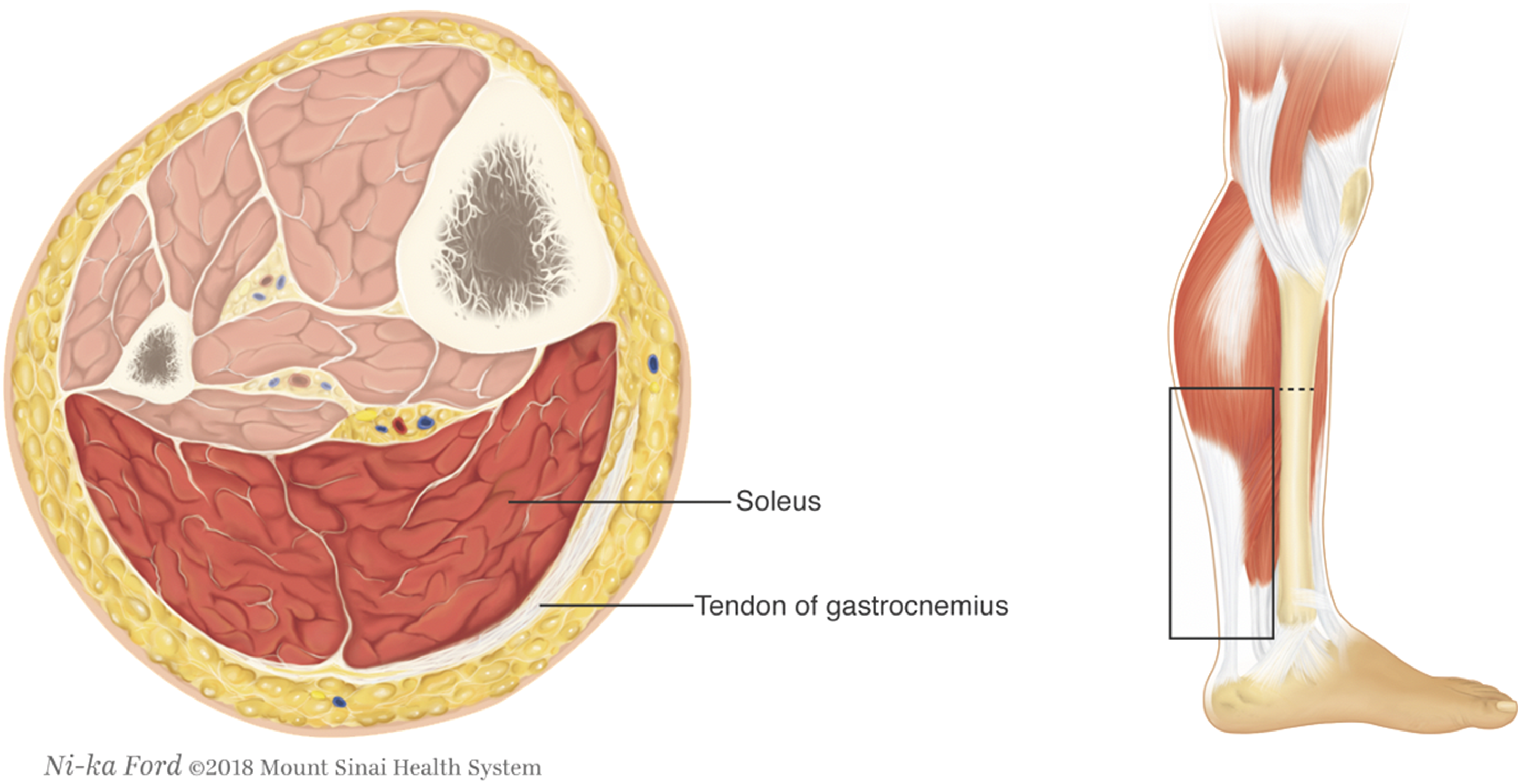
In addition to sparing of the soleus muscle and the gastrocnemius tendon, this technique leaves the extensor and flexor digitorum longus muscles, extensor and flexor hallicus longus muscles, the tibialis posterior, peroneus longus, and brevis muscles (Figure 3). If still more bulk is needed, even the anterior tibias muscle can be left in a BKA stump, further protection against stump failure. Illustration of preserved musculature with the muscle-sparing below knee amputation technique.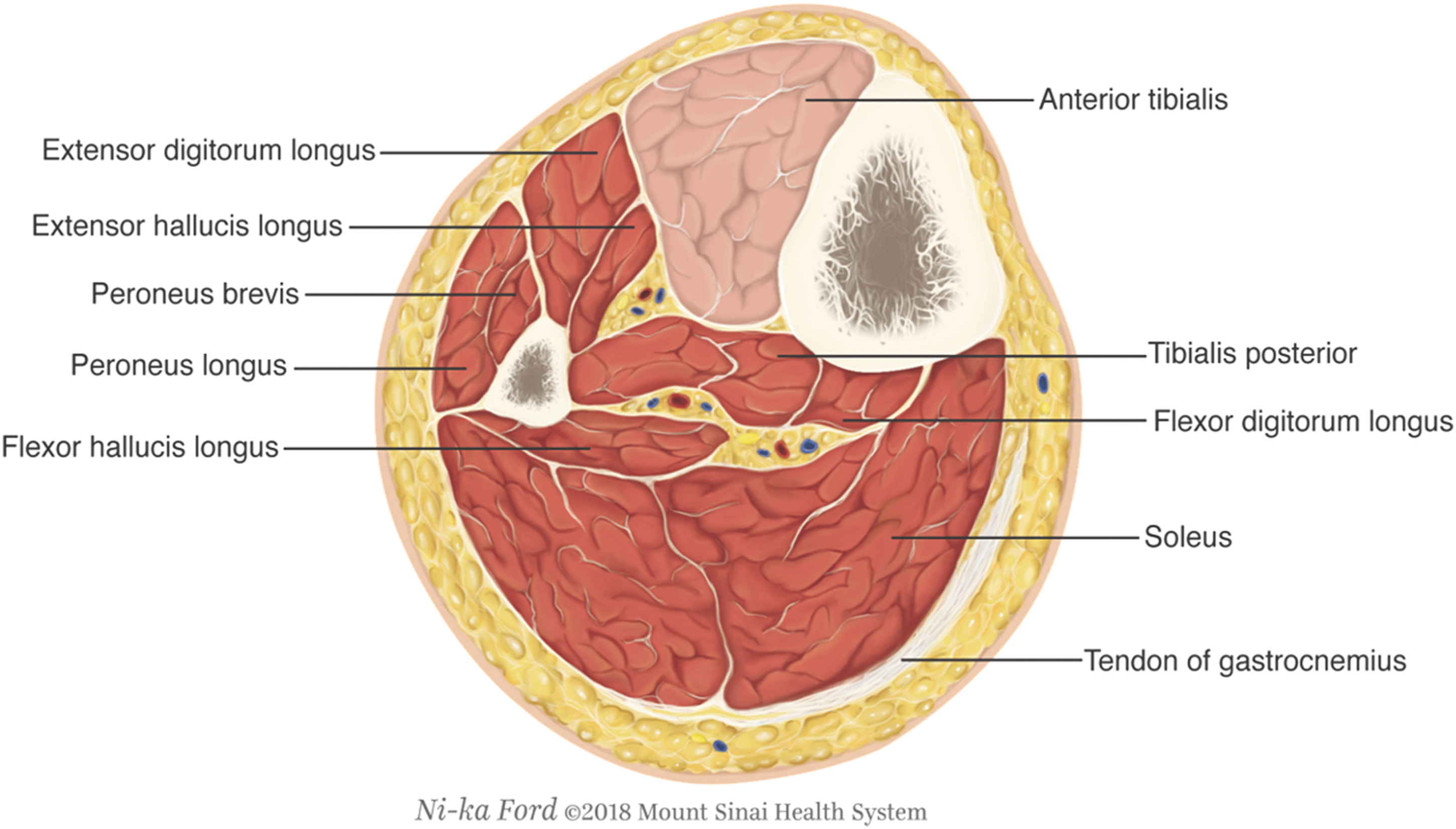
The other benefit observed from this technique is a comparatively decreased estimated blood loss, avoiding transfusions and helping in earlier recovery in elderly patients who more than often have a concomitant history of anemia and comorbidities. This may translate into shorter hospital stays. The increased bulk of the stump should decrease complications seen from poor bone coverage such as ulceration and pain with a prosthesis. The surgeon felt that this technique addressed several shortcomings with the traditional approach. This technique has been adopted routinely in our practice. Finally, this technique may give more satisfactory results to both patients and providers, although longer interval of follow would be needed to support these assumptions.
This study has several limitations. First, we have no quantitative measure of muscle mass. The age of greater than 60 years was arbitrarily chosen based on clinical observation that patients over the age of 60 years tend to have less muscle mass. Second, some of these patients ultimately did not ambulate on a prosthetic due to multiple factors and so was not assessed.
Conclusion
The advantages of muscle-sparing below knee amputation should be highlighted in the elderly population where sparing only the soleus and gastrocnemius muscles may not be enough to provide a stump with adequate muscle mass to prevent stump failure. The muscle-sparing below knee amputation should be considered in elderly and cachectic patients in whom the normally bulky posterior calf muscle mass is lacking. Its selective removal of muscle bundles with regard to their blood supply leaves maximum coverage of the bone, as well as decreasing potential hematoma formation and blood loss.
Supplemental Material
sj-pdf-1-ves-10.1177_15385744211045155 – Supplemental Material for The Benefits of a Muscle-Sparing Below Knee Amputation in the Elderly Population
Supplemental Material, sj-pdf-1-ves-10.1177_15385744211045155 for The Benefits of a Muscle-Sparing Below Knee Amputation in the Elderly Population by Jared M. Theriot, Prabhat Bhattarai and David J. Finlay in Vascular and Endovascular Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.