
Abstract
We report 2 cases of successful thoracic endovascular aortic repair (TEVAR) for acute type B aortic dissection (ABAD) complicated with spinal cord ischemia (SCI). Case 1. A 70-year-old gentleman found with an uncomplicated ABAD with false lumen occluded, developed SCI shortly after admission during the initial medical management. Cerebrospinal fluid drainage (CSFD) was initiated followed by emergent TEVAR. SCI improved, and the patient was discharged. Case 2. A 52-year-old gentleman developed uncomplicated ABAD with patent false lumen. 5 hours after admission, he developed SCI during the initial medical management. Emergent TEVAR was performed followed by CSFD, and the SCI improved before discharge. These cases prompted us to address prompt TEVAR for primary entry closure and true lumen dilatation with postoperative hypertensive management to relieve the dynamic obstruction of the segmental arteries responsible for the compromised spinal cord circulation in complicated ABAD.
Keywords
Introduction
In contemporary guidelines,1,2 optimal medical treatment is recommended as the gold standard for uncomplicated acute type B aortic dissection (ABAD). Emergent surgical or endovascular interventions are required for complicated ABAD in lieu of a high in-hospital mortality rate of 23.5–29.3% reported in complicated ABAD.3,4 A majority of those cases were ruptured complications as opposed to organ malperfusion. The incidence of spinal cord ischemia (SCI) was relatively low (2–4%) in the setting of organ malperfusion,5,6 but paraplegia resulting from SCI, remains a devastating complication, adversely impacting patient outcomes, including quality of life (QOL). We report successful thoracic endovascular aortic repair (TEVAR) for 2 patients with SCI secondary to complicated ABAD.
Case Report
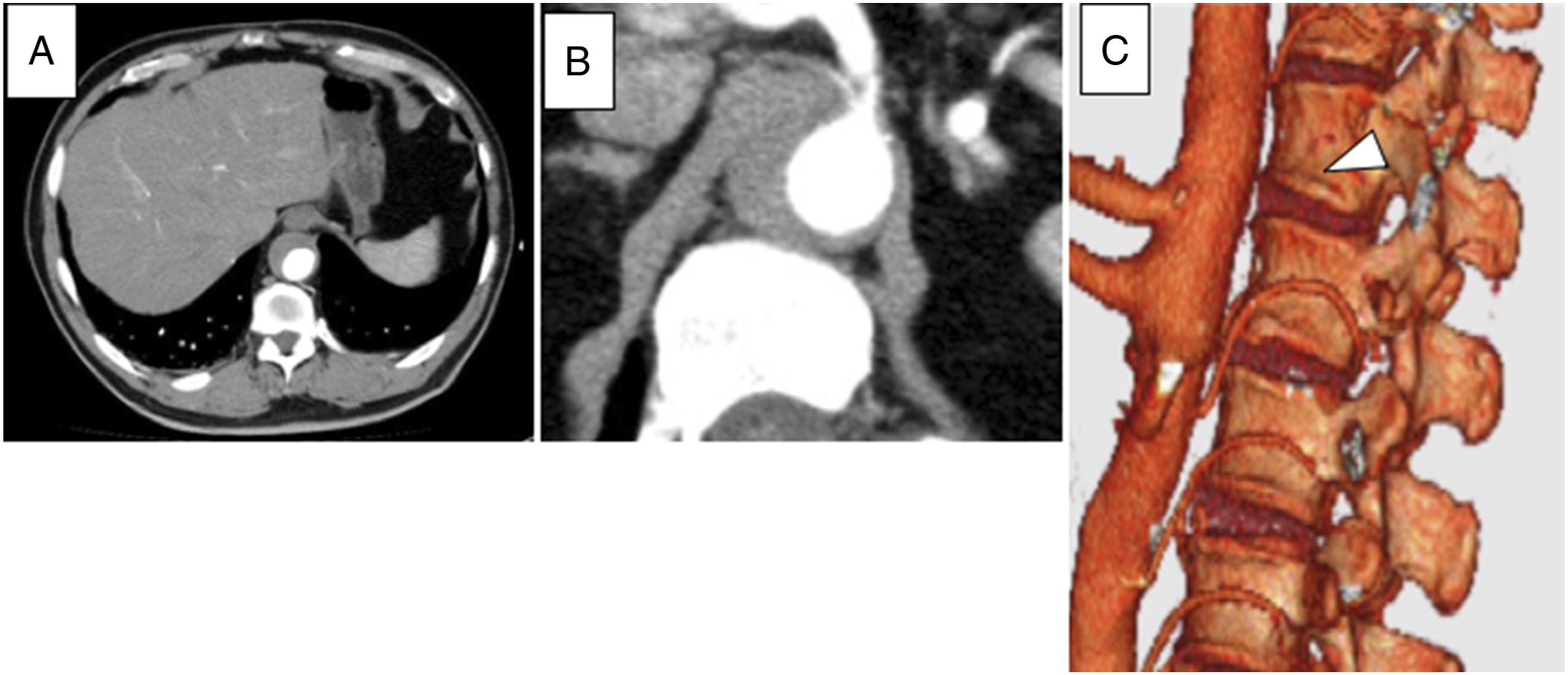
Preoperative computed tomography demonstrating acute type B aortic dissection with the false lumen occluded (A), and the 11th intercostal artery and 1st lumbar artery are contrasted, while the 12th intercostal arteries is not opacified obviously (arrowhead) (B, C).
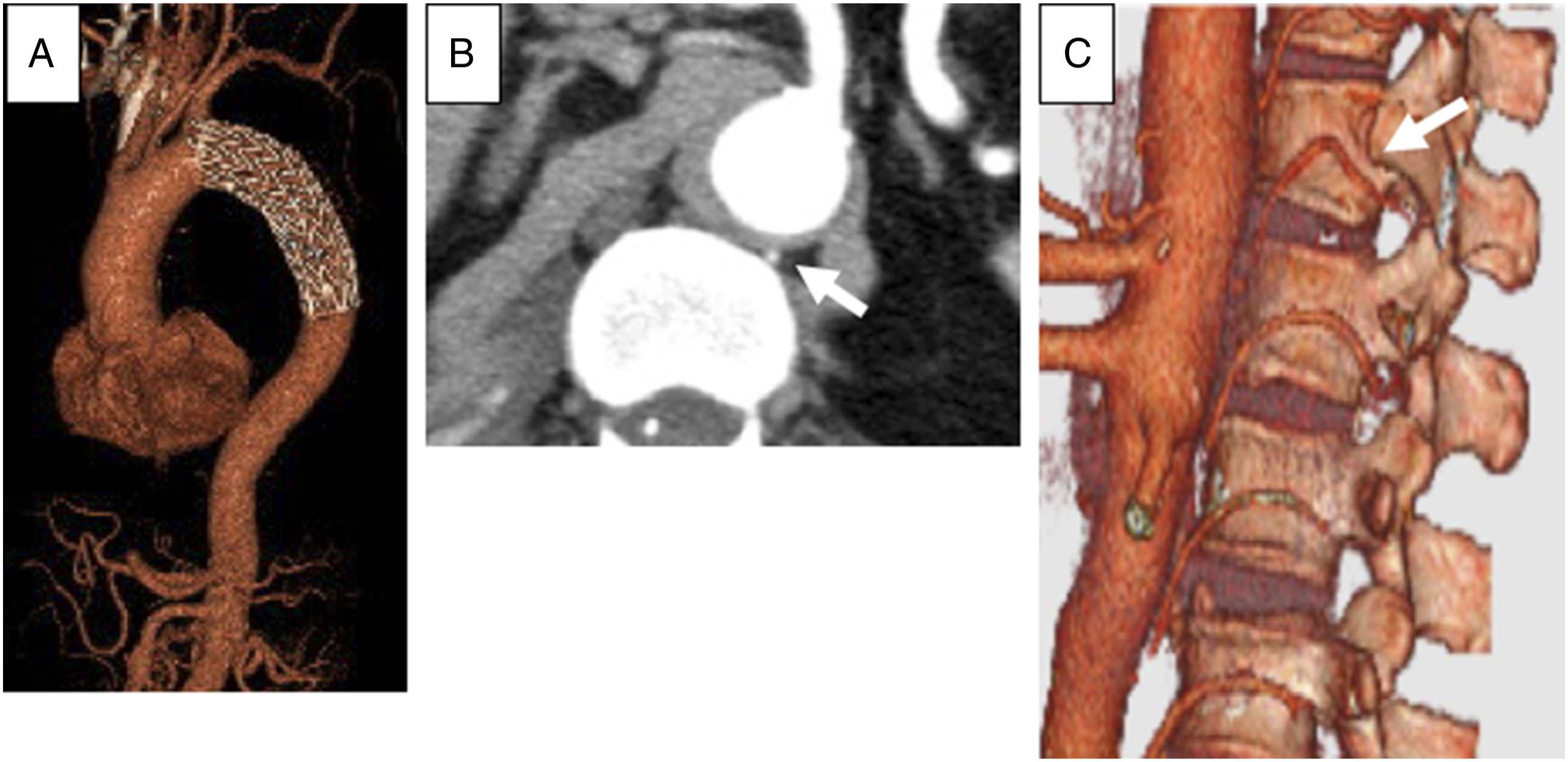
Postoperative computed tomography showing endoprothesis deployed from left subclavian artery to the descending aorta (A). And the dilatation of the true lumen. The 12th intercostal arteries, which had not been demonstrated preoperatively, is opacified (arrow) (B, C).
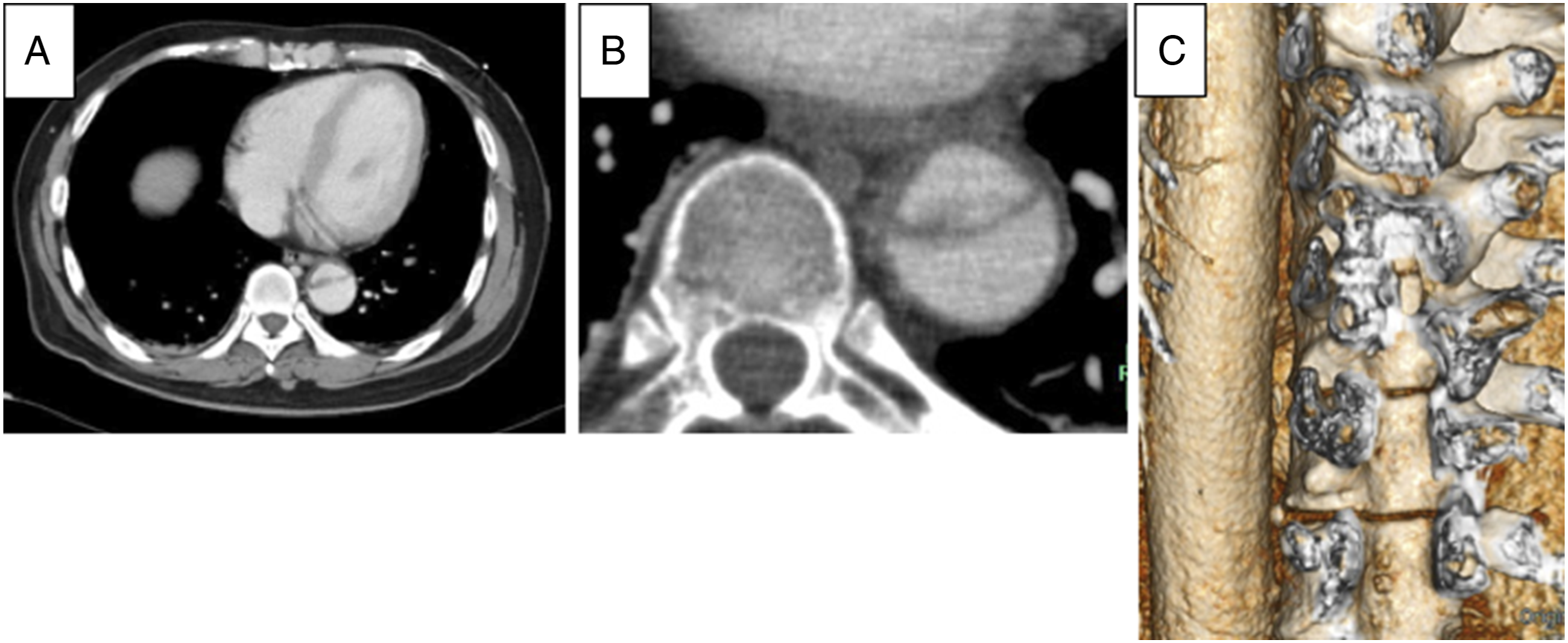
Enhanced computed tomography demonstrating acute type B aortic dissection with the false lumen patent, which causes the compression of the true lumen of the distal descending aorta (A), and the occlusion in almost all intercostal arteries of the descending aorta (B, C).
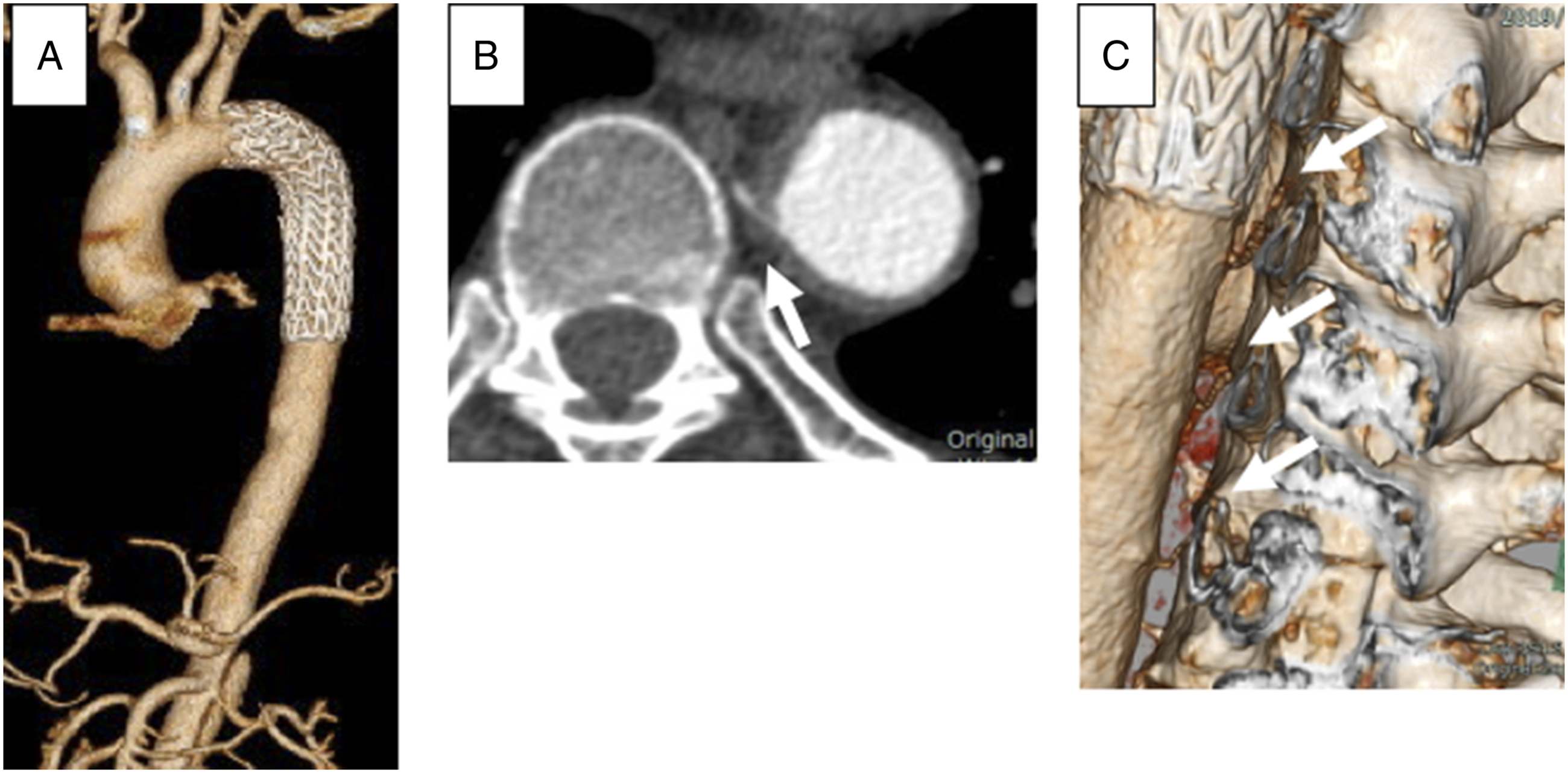
Postoperative computed tomography (CT) showing endoprothesis deployed from left subclavian artery to the descending aorta (A), the true lumen is sufficiently dilatated and the seventh–ninth intercostal arteries, which had not been demonstrated on the preoperative CT, are opacified (arrow) (B, C).
Discussion
In cases with uncomplicated ABAD, rest and antihypertensive therapy are indicated because when this optimal medical treatment is introduced, a much lower mortality rate (0–7.4%) is observed in contrast to surgery, which carries a much higher mortality risk.7-9 The annual survival rate of uncomplicated ABAD is over 80%. 10
However, approximately 25% of ABADs are complicated upon admission or after, resulting in early death or permanent physical disability.11,12 The 30-day mortality rate of complicated ABAD was reported as 23.5–29.3%.3,4 Complicated ABAD is defined as acute aortic rupture or impending rupture, malperfusion involving visceral, renal, spinal cord or extremities, uncontrolled hypertension, persistent or recurrent pain, or rapid expansion evident on CT. 13 During the initial medical management, clinical signs of organ malperfusion manifesting as chest and abdominal pain, motor or sensor deficits, oliguria, or absent femoral pulsation, should be promptly assessed and managed. Moreover, primary and secondary entry locations, true and false lumens diameters, visceral and renal artery branching origins, and the presence of organ contrast effect should be evaluated on CT precisely and serially with great cautions.
Spinal cord ischemia has a very low incidence rate of 2–4% in the setting of all acute aortic dissections.5,6 The current guidelines recommend emergent surgical or endovascular interventions for complicated ABAD,1,2 and recently, it has been reported that TEVAR may be useful for improving kidney, bowel or lower extremity ischemia.14-16 However, in contemporary guidelines, there have been no detailed descriptions on adequate treatments for spinal cord malperfusion because TEVAR cases for SCI are extremely rare due to its low incidence.
Three mechanisms of organ malperfusion have been proposed in ABAD: dynamic, static, and mixed obstruction of the organ perfusion. Dynamic obstruction is caused by true lumen compression and/or compression of the arterial branches by a dilated and higher pressure false lumen in the settings of a larger entry and a smaller re-entry. SCI has been reported to be mostly due to dynamic obstruction secondary to the intimal flap motion within the aortic lumen; the intimal flap itself can obstruct the orifices of segmental arteries. 16
Dynamic obstruction could be managed by prompt TEVAR to restore organ perfusion and prevent irreversible organ ischemia.14,15 TEVAR for ABAD eliminates antegrade flow into the false lumen by coverage of the primary entry,16-18 thereby expanding the stenotic true lumen and restoring branch vessel perfusion. 16 In the present cases, several ICAs that were not detected on preoperative CT were visualized on CT postoperatively.
Prompt TEVAR has another advantage for managing ABAD with organ ischemia. The primary entry closure by TEVAR shrink the false lumen and decrease the risk of fatal aortic rupture; it can allow us to maintain the mean blood pressure around 100 mmHg in order to provide sufficient organ perfusion.
A collateral network concept was proposed by Griepp. et al in 1996; there exists an axial network of small arteries in the spinal canal, the peri-vertebral tissues, and the paraspinous muscles around the spinal cord. It is supplied not only by ICAs and lumber arteries but also by the subclavian and the hypogastric arteries and their branches. 19 Moreover, the etiology of paraplegia is multifactorial, as it may include perfusion failure of Adamkiewicz artery and occlusion of the collateral arterial sources. In addition, systemic hypotension and previous abdominal aortic surgery should be considered among other etiologies.20,21
Therefore, paraplegia can be prevented by maintaining sufficiently high blood pressure without causing fatal aortic rupture.
Conclusion
We report successful prompt TEVARs for SCI complicated with ABAD. Primary entry closure and true lumen dilatation by TEVAR with postoperative hypertensive management is a key management option to relieve SCI secondary to dynamic obstruction in ABAD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent has been obtained from the patient for publication of the case report and accompanying images.