
Abstract
Acquired arteriovenous fistulas involving the carotid artery are most frequently the result of trauma and iatrogenic causes such as central venous catheterisation. Occasionally, they may develop spontaneously due to erosion of an aneurysm into an adjacent vein. We report a rare case of an acquired carotid-jugular fistula secondary to a pseudoaneurysm that occurred four months following carotid endarterectomy
Keywords
Introduction
Acquired arteriovenous fistulas (AVFs) involving the carotid artery are most commonly the result of high-velocity penetrating trauma and stab wounds and iatrogenic causes such as diagnostic and therapeutic catheterisation of the neck vessels. Infrequently, an AVF may develop spontaneously due to erosion of an aneurysm into an adjacent vein. Pseudoaneurysms represent an infrequent complication of carotid endarterectomy (CEA), with an estimated incidence of .3 to .6 percent. 1 Various aetiological factors have been proposed including failure of the suture line, degeneration of the arterial wall or of a patch if used for repair, clamp-induced trauma and infection.2–4 There is only one case report in the literature of an acquired carotid-jugular fistula (CJF) occurring as a delayed complication following CEA. 5
Case Summary
An 85-year-old man presented with crescendo transient ischaemic attack, marked by recurrent episodes of weakness and loss of sensation of the fourth and fifth digits of his right hand. He was an ex-smoker (10 pack years) with a history of atrial fibrillation and gastroesophageal reflux. He was receiving lipid-lowering (atorvastatin), anti-hypertensive (candesartan, lercanidipine and hydrochlorothiazide), anti-reflux (pantoprazole), anticoagulant (rivaroxaban) and antiplatelet (aspirin) therapy. He had no known allergies. Computed tomographic angiography (CTA) demonstrated atheromatous plaque at the origin of the left internal carotid artery (ICA) causing a high grade (> 80%) stenosis. The contralateral (right) carotid and subclavian arteries were patent with minimal calcific disease only. The vertebral arteries were widely patent, arising from the subclavian arteries with co-dominant morphology. The circle of Willis had a conventional anatomical configuration, with no evidence of occlusive or aneurysmal disease in any of its branches. Magnetic resonance imaging had revealed scattered foci of acute infarction in the left parietal cortex, and evidence of chronic small vessel ischaemia.
The patient underwent a left CEA under regional cervical anaesthesia and heparin cover using the eversion technique without requirement for shunt or a patch closure. The eversion technique consisted of complete transection of the internal carotid artery via an oblique incision opposite the origin of the external carotid artery. The ICA plaque was removed via eversion, and the distal common carotid artery (CCA) and the proximal external carotid artery (ECA) were also endarterectomised with good end points achieved in all 3 vessels. The ICA was then re-anastomosed with continuous 6-0 polypropylene suture. At the end of the procedure, good pulses were present in all carotid vessels. Haemostasis was achieved and systemic heparin was reversed with protamine. A suction drain was placed at the operative site.
The patient made an uneventful recovery and had no symptoms post-operatively. He was kept in hospital while undergoing assessment by physiotherapy and social work services. He was discharged 3 days following the operation on low dose aspirin and rivaroxaban therapy. The patient attended for routine follow up duplex ultrasound scans (DUS) at both 3 weeks and 4 months following the operation. Imaging was performed in the same vascular laboratory by the same vascular sonographer.
The 3-week scan showed a normal post-operative appearance of the left carotid bifurcation. The 4-month scan showed a saccular dilatation of the distal left CCA to 1.7 cm, suggestive of a pseudoenauerysm at the anastomotic site. Physical examination confirmed a prominent carotid pulse on the left side, but there was no tenderness or overlying skin change. The patient had no neurological deficit and no signs of heart failure.
The patient was referred for a CTA, which revealed a pseudoaneurysm at the site of the left CEA (Figure 1). The sac appeared well-contained, measuring 10 mm x 8 mm in the coronal-transverse plane. No additional enhancement was seen on the delayed sequence. Following the initial CEA procedure, the patient had not exhibited any local or systemic signs or symptoms of infection, and his biochemical and inflammatory markers were within normal range. CTA Aortic Arch – Circle of Willis, IV contrast (arterial phase), with (a) coronal-transverse and (b) axial views, demonstrating left carotid artery pseudoaneurysm at proximal site of CEA (indicated by green arrows).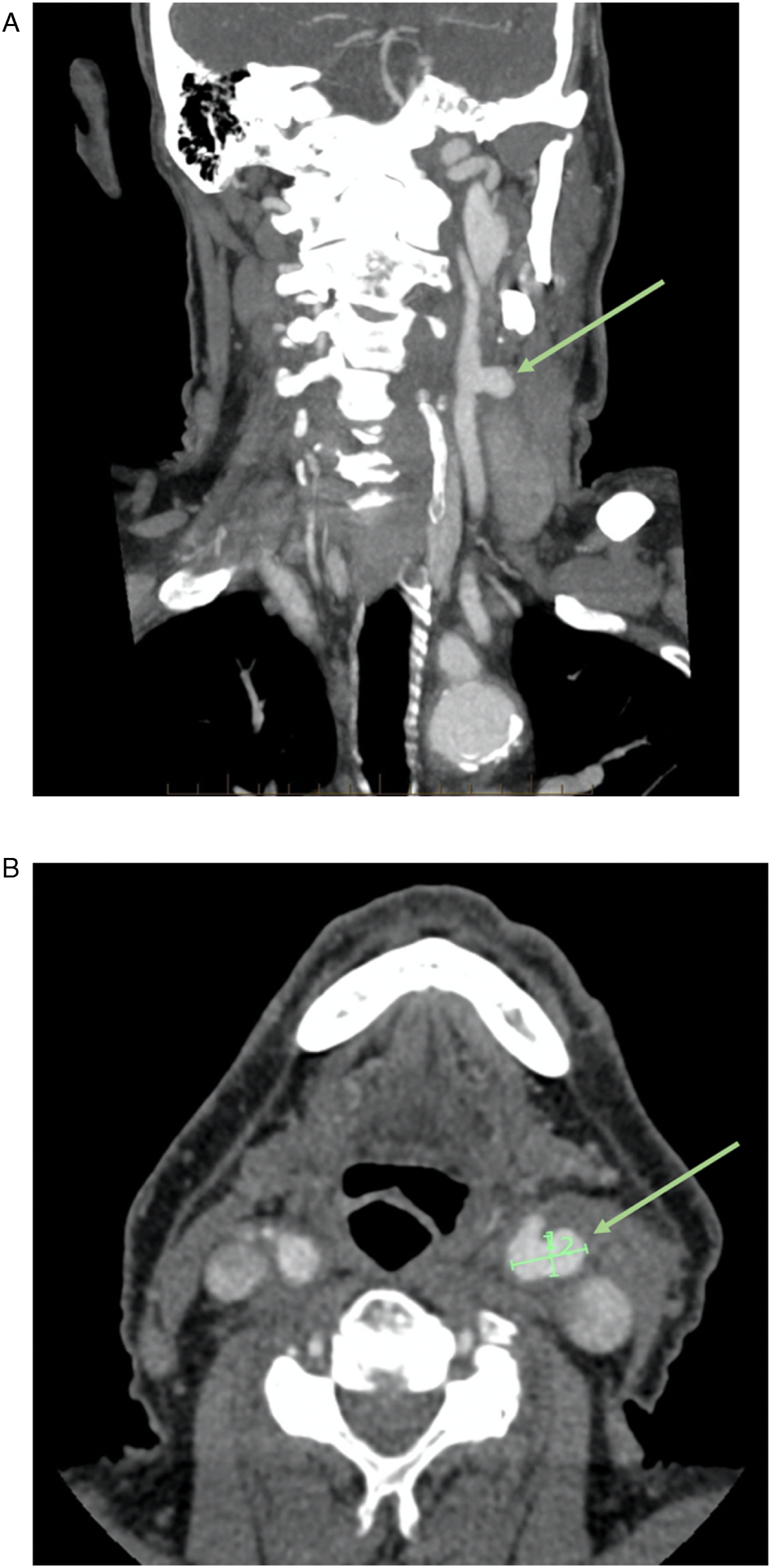
The patient was consented for a further open carotid surgical procedure with the intention to repair the pseudoaneurysm but with the possibility of requirement for ICA ligation under general anaesthesia. The initial carotid procedure was performed under regional anaesthesia; however, given a shunt had not been required, it was inferred the patient’s intracranial circulation was well-collateralised. An extensive dissection was also anticipated.
A precautionary 5Fr Britetip sheath (Cordis, Johnson & Johnson, Warren, NJ) was inserted retrograde into the right common femoral artery. The purpose of this was to allow placement and use of an endovascular carotid balloon, to assist control of carotid haemorrhage, if required. Significant inflammation was noted during the exposure with dense adhesions between the carotid and jugular vessels. The left internal jugular vein (IJV) was dilated.
The proximal and distal ICAs were dissected, and vessels loops placed. Upon application of a loop held under tension, the IJV was observed to be pulsatile, consistent with arteriovenous fistula (AVF). The external carotid artery (ECA) was dissected and looped. Vascular clamps were applied under heparin cover. Upon further dissection of the IJV from the CCA, a pseudoaneurysm was identified eroding anteriorly from the endarterectomy site into the wall of the adjacent IJV. There were no findings to suggest an infective process. The carotid anastomosis suture line appeared to be intact; however, given it was so deeply incorporated within the pseudoaneurysm sac, a defect could not be excluded.
The tissue wall of the CCA proximal to the pseudoaneurysm was friable and of poor integrity in the context of recent CEA and post-operative changes. Attempts to repair the CCA via anastomosis caused tearing through the vessel wall. However, brisk back-bleeding was observed from the ICA and ECA upon clamp release. Given the patient had not required shunt support while awake during the original CEA, carotid ligation was performed.
The distal CCA and the proximal ICA and ECA all required ligation. The sac wall was sent for tissue microbiology and histopathology, which returned negative results. The IJV was dissected out meticulously, proximal and distal to the CJF, in preparation for extrinsic control if required. When the pseudoaneurysm was opened, IJV control was achieved with a single clamp and the defect was oversewn.
Given the theoretical increased risk of ICA thrombosis extending to the intracranial branches and consequent stroke, the patient was anticoagulated with a heparin infusion (activated partial thromboplastin time 70–90s) and a systolic blood pressure target between 140 and 160 mmHg was maintained. His oral anticoagulants were then reintroduced at 72 hours. Intravenous antibiotics were continued for 48 hours.
Post-operatively, the patient exhibited signs and symptoms including left-sided tongue deviation, dysarthria, dysphagia, dysphonia and a bovine cough. These were consistent with intra-operative manipulation of cranial nerve branches IX–XII. Under supervision of a speech pathologist and dietitian, the patient’s speech and swallow function improved rapidly. He was discharged 10 days post-operatively on his regular anticoagulation and antiplatelet therapy, with plans for a follow-up arterial DUS in 4 weeks.
Discussion
Pseudoaneurysms represent an infrequent complication of CEAs, with an estimated incidence of .3–.6%. 1 Various aetiological factors have been proposed including failure of the suture line, degeneration of the arterial wall or of a patch if used for repair, clamp-induced trauma and infection.2–4 The natural history of pseudoaneurysms is poorly understood – the pathology has been described days to years following a patient’s CEA. 6 Acquired arteriovenous fistulas (AVFs) involving the carotid artery are most commonly the result of high-velocity penetrating trauma and stab wounds, or iatrogenic causes such as diagnostic and therapeutic catheterisation of the neck vessels. Infrequently, AVFs may develop spontaneously due to erosion of an aneurysm into an adjacent vein. Carotid artery AVF typically has a communication between the ICA and IJV or its tributaries.7,8
The authors have attributed technical factors, including failure of the suture line, as the best explanation for the development of the patient’s carotid pseudoaneurysm. An infective cause could not be excluded. There were however no signs or symptoms, locally or systemically, to prompt a septic workup pre-operatively. Further, there were no findings to suggest an infective process intra-operatively. The first post-operative scan additionally did not identify any abnormalities. The role of the patient’s anticoagulation in propagating the pseudoaneurysm has been considered. Indeed, there are no anatomical boundaries in the neck to restrict development of pseudoaneurysms once they have developed.
Acquired carotid-jugular fistulas following CEA are extremely rare. A literature search of delayed vascular complications following CEA identified only one case of carotid-jugular AVF 5 . The patient was a 66-year-old man who had presented with symptoms of amnesia, ataxia and fatigue with a history of right-side CEA performed 6 years prior. Catheter angiography revealed an AVF between the right ECA and IJV, treated with access via the contralateral IJV using coil embolization. The patient made a complete neurological recovery. Our service has performed over 2500 CEAs, including over 600 eversion CEAs. All are followed up monthly, four-monthly, nine-monthly and then annually. We have not encountered such findings previously. The development of an acquired CJF between the CCA anastomosis and IJV, secondary to a pseudoaneurysm after CEA, has not been previously reported to our knowledge.
The natural history of an AVF depends upon the diameter of its constituent vessels, its size and location, the collateral circulation and the valvular competence of veins distally. While some AVFs reduce in size over time and close spontaneously, a significant proportion develops larger communications due to degenerative changes in the arterial wall. 9 The most common presenting signs of an AVF are a thrill, bruit or pulsatile mass. 10 Together with distended neck veins, these may be the only findings in patients with a small CJF. However, large and untreated CJFs may cause ischaemic neurological symptoms secondary to thromboembolism or shunting of blood through the fistula. 7 They may additionally precipitate high-output congestive heart failure as a result of increased venous return. 9
Imaging with colour-flow DUS is useful in identifying AVFs and arterial injuries but is limited by its operator-dependence and poor sensitivity in identifying correctable defects such as intimal flaps 11 . Our case notwithstanding, CTA is a highly sensitive and specific modality for the diagnosis and evaluation of cervical AVF. 12 It is fast, minimally invasive, well-tolerated and less expensive than catheter angiography. Its principal drawbacks are associated radiation exposure and contrast-induced nephropathy. It is noteworthy that neither DUS nor CTA were able to detect the CJF in our patient. The authors propose that the early development of the CJF and low flow across the lesion may have precluded its diagnosis.
The goals of treatment for acquired CJFs include closure of the fistula and reconstruction of the affected arteries and veins, while maintaining haemodynamic stability. When repair is not possible, vessel ligation is the only option for patient survival. AVFs of the CCA, carotid bifurcation and proximal ICA are amenable to repair with standard surgical techniques. Repair of AVFs involving the distal ICA may require anterior subluxation of the mandible and other manoeuvres to improve exposure at the base of the skull. Similarly, AVFs of the origins of the CCA may require median sternotomy. Shunts are used selectively, based upon carotid backpressure and AVF location. 8
Endovascular repair presents an alternative for high-risk surgical candidates and those with surgically inaccessible lesions of the neck. Available options include transcatheter embolization techniques, stent-graft deployment or a combination. Prerequisites for endovascular management of CJFs are accessibility of the artery above and below the lesion, and anatomy appropriate to facilitate deployment of embolic material or stent-graft. Endovascular repair would have obviated the patient’s post-operative neuropraxia, and treatment with a covered stent was considered. However, in the setting of an infective process, the patient would have been at risk of significant post-operative consequences including septic embolism, acute thromboembolism and stroke.
A hybrid approach can be employed, whereby endovascular balloon occlusion is used to minimise bleeding and assist surgical repair. There are no case series or studies with long-term follow-up comparing open and endovascular treatments. 13
Following carotid ligation, the ICA fills progressively with thrombus and may result in stump embolization. It is recommended that patients be treated with therapeutic anticoagulation using intravenous heparin before transitioning to warfarin oral anticoagulation. 14 The duration of therapy is not standardised; however, regimens between 2 weeks and 3 months have been described.15,16 The outcomes of carotid ligation in the context of aneurysmal disease vary widely and depend upon the type, size and location of the diseased segment. Carotid ligation was historically associated with a 30 to 60 percent risk of stroke.17,18 Of these, approximately 50 percent did not survive.17,18
More recently, in a review of the 13 largest single-centre series since 1950, El-Sabrout and Cooley reported a combined rate of stroke and mortality associated with carotid ligation of 12 percent. 19 This change may be referable to improved peri-operative anaesthetic technique, medical management and post-operative anticoagulation. 14 By comparison, the combined rates of stroke and death for patients managed by surgical reconstruction and patients treated non-operatively are 9 and 21 percent, respectively. 19
Conclusion
We have reported a unique case of an acquired carotid-jugular fistula secondary to a pseudoaneurysm, occurring four months following carotid endarterectomy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent has been obtained from the patient for publication of the case report and accompanying images.