
Abstract
Objective
The purpose of this study was to evaluate the efficacy and safety of ultrasound-guided repeat access and repeat closure with an ExoSeal vascular closure system.
Methods
A total of 123 endovascular therapy (EVT) procedures were performed in 59 patients (65 limbs) with ultrasound-guided repeat access and repeat implantation of an ExoSeal vascular closure system between January 2019 and March 2021. The procedural details and postprocedural outcomes of EVT with repeat access and use of ExoSeal (RE group) were compared with those of EVT with initial use of ExoSeal (IE group) in the same patients. In a subgroup analysis, these outcomes were also compared in early repeat (within 3 months) and late repeat (over 3 months) cases.
Results
The technical success rate of ultrasound-guided access in the RE group was 100%. The procedural success rate of EVT and deployment success rate of ExoSeal in the RE group were 93% and 94%, respectively, which were not significantly different to those in the IE group. Access site complications in the RE group occurred in 2 cases (2%), again with no significant difference with the IE group. The median puncture, procedural, and hemostasis times in the RE group were 3 [2-5], 36.5 [29-54], and 7 [5-10] min, respectively, which were not significantly longer than those in the IE group. In the RE group, early and late repeat closure was performed in 66 (54%) and 57 (46%) cases, respectively, and there were no significant differences in the technical success of ultrasound-guided access, procedural success of EVT, deployment success of ExoSeal, and access site complication rates in these cases.
Conclusions
Ultrasound-guided access facilitated higher technical success of repeat access and fewer access site complications in EVT with repeat use of ExoSeal, regardless of the interval between procedures.
Introduction
Endovascular therapy (EVT) for peripheral arterial disease (PAD) is increasingly used worldwide due to its minimal invasiveness, technical advances, safety, and efficacy.1-3 Manual compression after the procedure was the standard method for achieving hemostasis at the femoral access site. However, this procedure has several problems, including prolonged hemostatic time, longer required bed rest, and pain during bed rest. Therefore, several closure systems (Angio-Seal, ExoSeal, ProGlide) have been established for use after EVT.4,5
ExoSeal (Cordis Corporation, Bridgewater, NJ, USA) is a vascular closure device consisting of a plug applier and a bioabsorbent polyglycolic acid plug. After implantation, ExoSeal is thought to absorb completely in 2 to 3 months. Therefore, repeat access and closure with ExoSeal are reasonable for EVT using the same access site after 3 months. However, most chronic limb-threatening ischemia patients require repeat EVT; there is limited information on repeat access and closure within 3 months using ExoSeal in patients with PAD. 6 Therefore, the aim of this study was to evaluate the efficacy and safety of ultrasound-guided repeat access and closure with ExoSeal in this patient population.
Patients and Methods
A total of 123 EVT procedures were performed in 59 patients (65 limbs) with PAD using ultrasound-guided repeat access and implantation of an ExoSeal device between January 2019 and March 2021. Data were collected from medical records for patient background (age, sex, Rutherford classification, diabetes, hypertension, dyslipidemia, smoking history, coronary artery disease, cerebrovascular disease, and hemodialysis); procedural details (femoral approach method, sheath size, number of previous closures with ExoSeal, technical success of access, procedural success of EVT, deployment success of ExoSeal, puncture time, procedural time, and hemostatic time); and postprocedural outcomes (access site complication, hospital death, major amputation, and cardiovascular events). The procedural details and postprocedural outcomes were compared for repeat (RE group) and initial (IE group) use of ExoSeal in the same patients. In a subgroup analysis, outcomes were compared in early repeat (within 3 months) and late repeat (over 3 months) cases.
Study Endpoints
The primary endpoint was the technical success of access. The primary safety endpoint was access site complication. The secondary endpoints were the puncture, procedural, and hemostatic times for EVT and the procedural success of EVT.
Definitions
Technical success of access was defined that the sheath could be inserted within 10 min without hematoma. Procedural success of EVT was defined as ≤30% stenosis remaining, based on the completion angiogram. Major amputation was defined as limb loss above the ankle level. Puncture time was defined as the interval between local anesthesia administration and sheath insertion. Hemostatic time was defined as the manual pressure time. Early repeat use was defined as that within 3 months from previous use, and late repeat use was defined as that over 3 months.
EVT Procedure
All patients for whom EVT was recommended were treated as inpatients. If the common femoral artery (CFA) after implantation of ExoSeal was the preferred site for access, this site was punctured, regardless of the interval from the initial implantation of ExoSeal. If ultrasound revealed incomplete absorption of the previously implanted ExoSeal, especially in early repeat cases, the puncture needle was inserted approximately 5 mm proximally from the initial implanted ExoSeal under ultrasound guidance (Figure 1). A residual ExoSeal plug 2 weeks after common femoral artery closure shown on ultrasound (white arrows).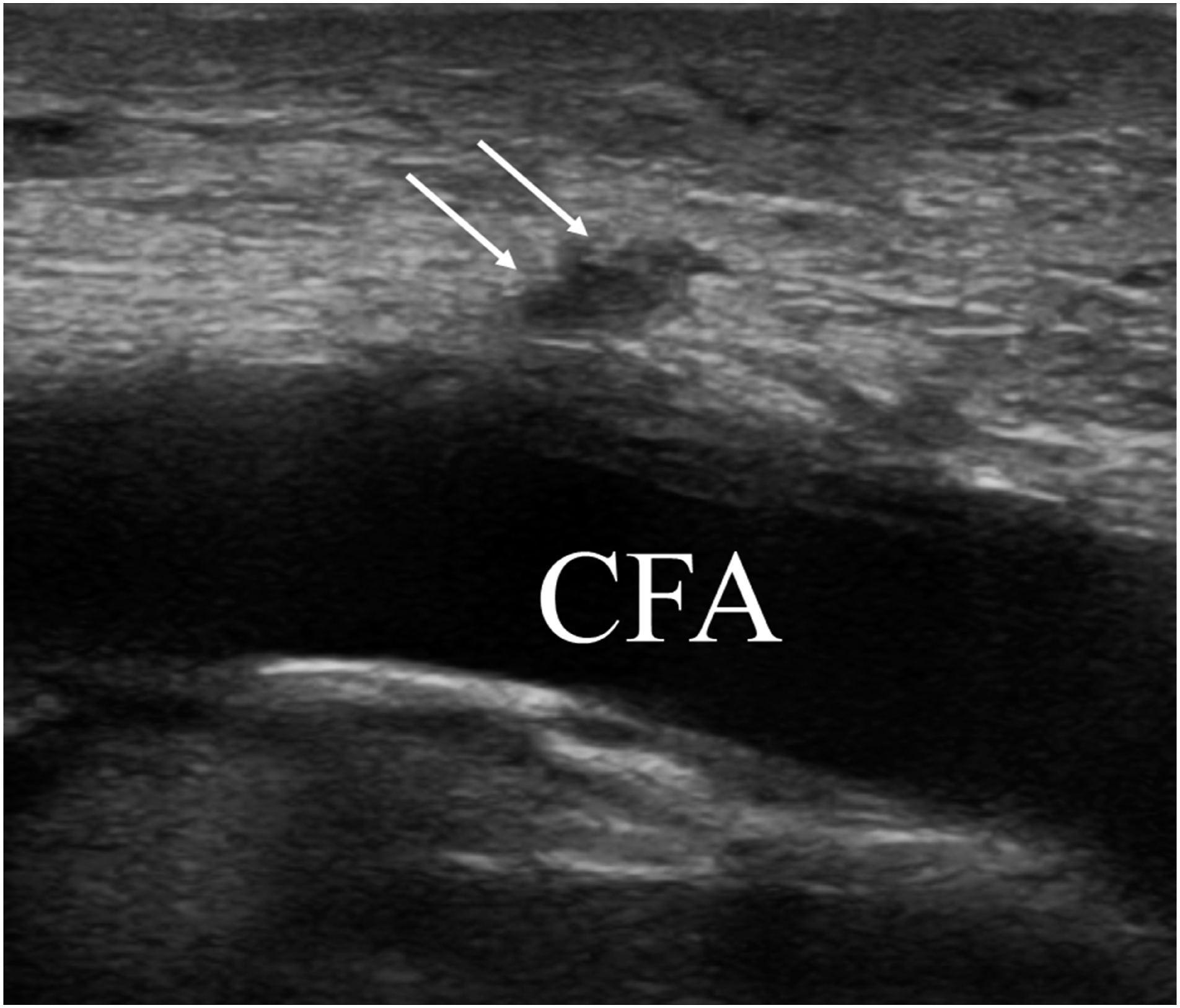
After a guidewire was inserted into the CFA, the access site was dilated with a dilater alone. After puncture site dilation, a 5 or 6 Fr sheath (Glidesheath Slender; Terumo Corp, Tokyo, Japan) was inserted. Heparin sodium was administered intravenously at 3000 units. The guidewire was passed through the lesion, and the lesion was expanded for 120 s using an optimally sized balloon. For an iliac lesion, a self-expandable nitinol stent was deployed. For a femoropopliteal lesion, a drug-coated balloon was the first choice, after plain old balloon angioplasty (POBA) without flow-limiting dissection or recoil. A self-expandable nitinol stent, a stent graft, or a drug-eluting stent was deployed only when flow-limiting dissection or recoil occurred. For an infrapopliteal lesion, POBA alone was performed. After the EVT procedure, the ExoSeal device was used. We routinely performed light manual pressure for 5 min after implantation of this device. If any blood leaked after release of this pressure, additional manual pressure was used. The procedures were performed by 2 surgeons and 2 cardiologists.
Medication
Patients who were already taking antiplatelet agents continued to take the same medication. For those taking no antiplatelet agents, aspirin (100 mg daily) or clopidogrel (75 mg daily) was started at least 1 week before EVT and continued lifelong.
Ethical Considerations
This study was approved by the ethics committee of JA Hiroshima General Hospital (Hatsukaichi, Japan; approval number, 21-28).
Statistical Analysis
Continuous variables are expressed as median values [25th-75th percentile]. Categorical variables are shown as absolute values and percentages. Differences in procedural details and postprocedural outcomes between groups were compared by Fisher’s exact test for categorical data and by the Mann–Whitney U test or Wilcoxon signed rank test for continuous variables. P < .05 was considered significant. All statistical analyses were performed with EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). 7
Results
Patient characteristics and clinical data.
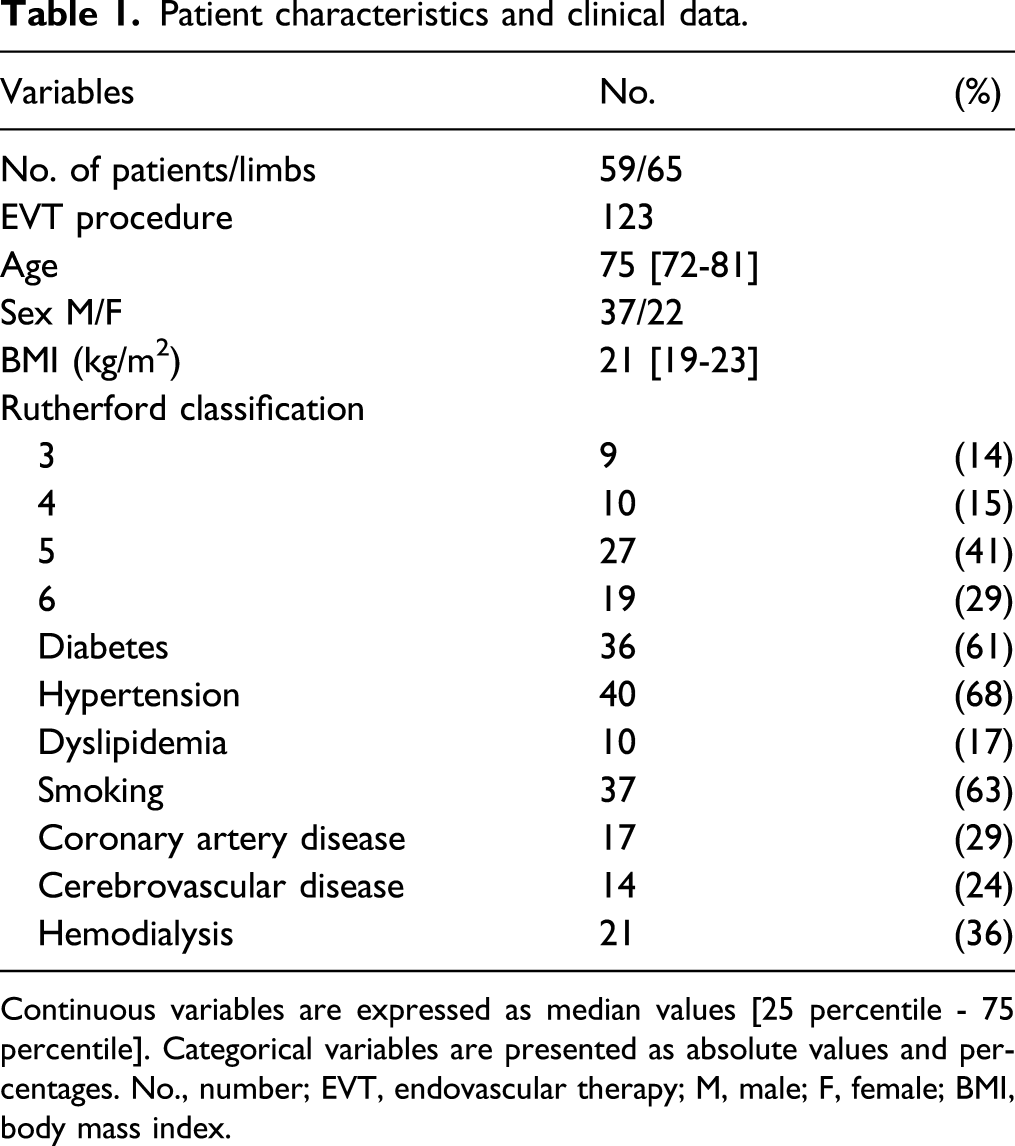
Continuous variables are expressed as median values [25 percentile - 75 percentile]. Categorical variables are presented as absolute values and percentages. No., number; EVT, endovascular therapy; M, male; F, female; BMI, body mass index.
Comparison of endovascular therapy details in initial ExoSeal (IE) and repeat ExoSeal (RE) groups.
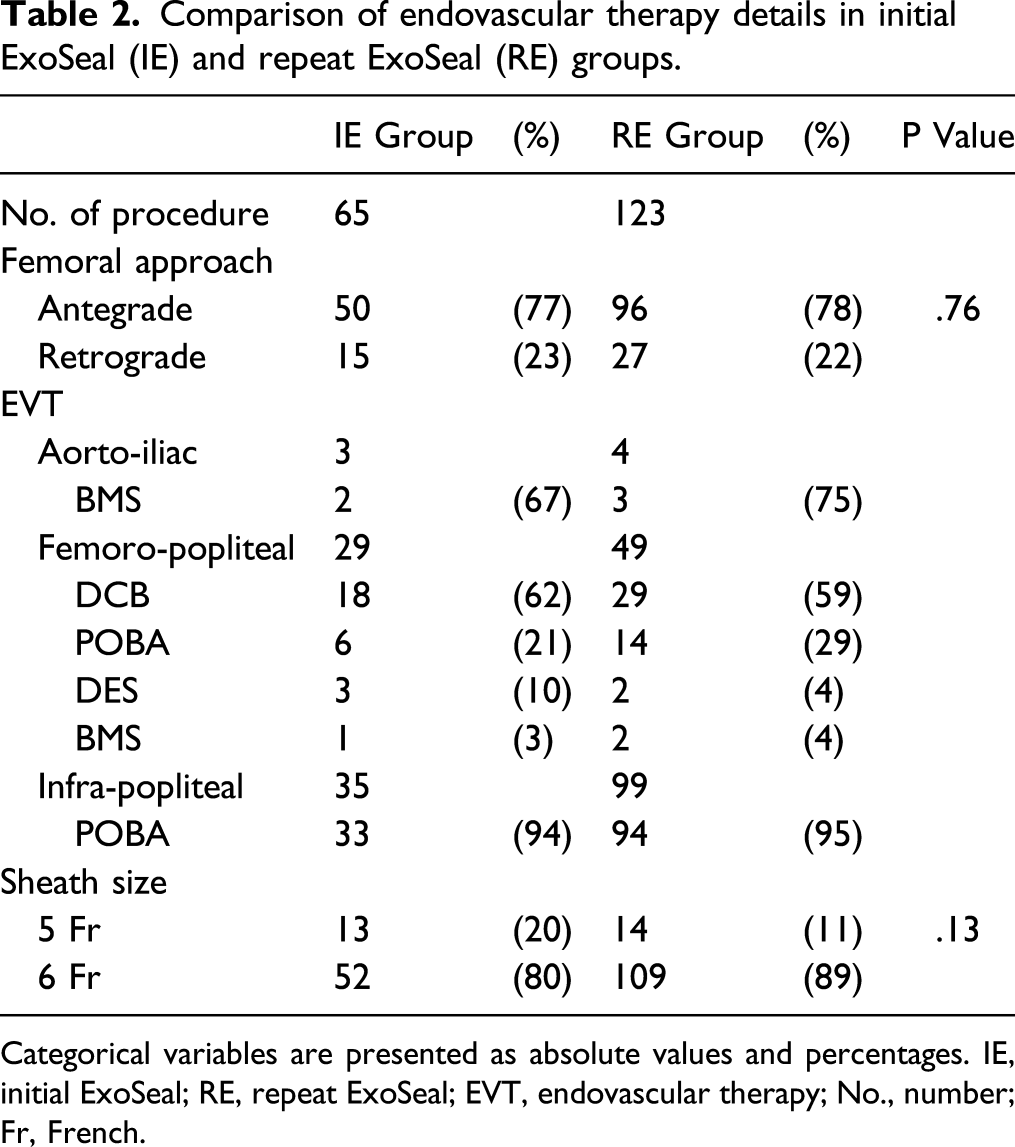
Categorical variables are presented as absolute values and percentages. IE, initial ExoSeal; RE, repeat ExoSeal; EVT, endovascular therapy; No., number; Fr, French.
Postprocedural outcomes in initial ExoSeal (IE) and repeat ExoSeal (RE) groups.
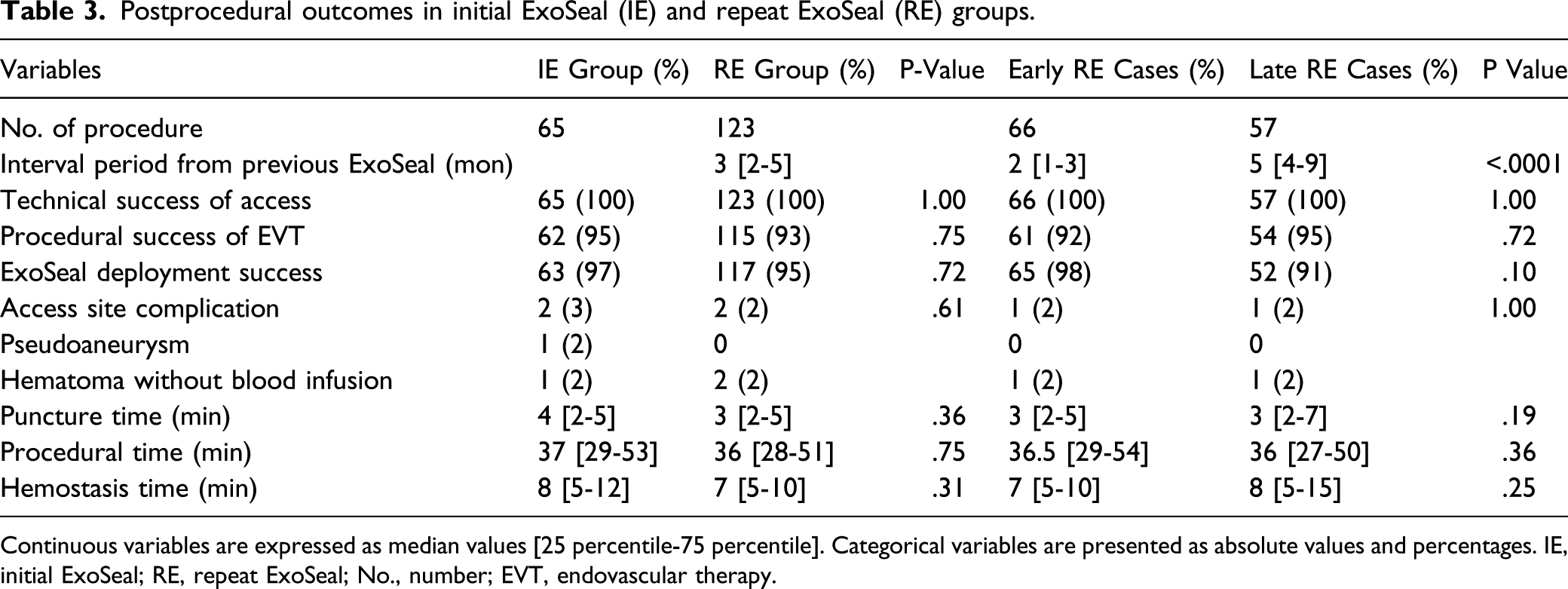
Continuous variables are expressed as median values [25 percentile-75 percentile]. Categorical variables are presented as absolute values and percentages. IE, initial ExoSeal; RE, repeat ExoSeal; No., number; EVT, endovascular therapy.
Early and late repeat ExoSeal closure was performed in 66 (54%) and 57 (46%) cases, respectively. The outcomes in early and late RE cases are summarized in Table 3. The technical success of access, procedural success of EVT, deployment success of ExoSeal, and access site complication rates, and the median puncture, procedural, and hemostasis times did not differ significantly in early and late cases.
Discussion
The 3 main results of this study were as follows: the procedural success rate of EVT of 93% in the RE group was favorable; the technical success of access in the RE group was 100% and the median puncture time in the RE group was 3 [2-5] min, both were acceptable; and the access site complication rate and median hemostasis time of 2% and 7 min in the RE group were comparable to those in the IE group.
Regarding the procedural success rate of EVT in the RE group, a femoral antegrade approach was mostly used (78% of cases) at the previous CFA access site for ExoSeal implantation. Whether a femoral antegrade or retrograde approach should be selected for EVT is controversial. In a series of 556 EVT procedures (antegrade approach, 461; retrograde approach, 95), Cragg et al. found that the femoral antegrade approach was associated with greater procedural success than the retrograde approach (83.8% vs 73.3%). 8 The manipulative complexity of the wire and catheter in the retrograde approach may reduce the success rate. Due to use of the previous ExoSeal site access, we often selected the antegrade approach, and this may have resulted in the high procedural success of EVT.
The median puncture time in the RE group was 3 [2-5] min, which was not longer than that in the IE group, and this time also did not differ significantly between early (within 3 months) and late repeat closure. Boschewitz et al. 6 previously showed the efficacy of repeat ExoSeal closure but did not examine the time dependence. After implantation, ExoSeal has been suggested to absorb completely in 2 to 3 months, but Choo et al. 9 found only partial absorption of an ExoSeal implant in follow-up ultrasound at 6 months. Thus, it is possible that the interval between ExoSeal implantation and complete absorption may differ among individuals. We selected the most preferable puncture site under ultrasound guidance. If ultrasound revealed incomplete absorption of the previous ExoSeal implant, the puncture needle was inserted approximately 5 mm proximally from the previous site under ultrasound guidance. This may explain the easy access in the RE group, regardless of the interval from the initial implantation.
Han et al. 10 reported a series of 176 ExoSeal cases with 5 Fr access that had an access site complication rate of .6%. Previous reports in ExoSeal series with 6 Fr access have found minor complication rates of 1-1.8% for pseudoaneurysm and 3.4-6.3% for inguinal hematoma.11-13 Thus, sheath size may influence the access site complication rate. In addition, Ramirez et al. 14 found that closure device use with CFA antegrade access had a higher risk than retrograde access (any access site hematoma, odds ratio = 1.46). In the current study, we most commonly used a 6 Fr sheath (89%) with a femoral antegrade approach (78%) in the RE group. Regardless of the interval from the previous procedure, access site complication in the RE group was comparable to that in the IE group and lower than for 6 Fr access in previous reports. Fujiwara et al. 15 have documented appropriate hemostasis by routine use of ultrasound echo-guided transfemoral access and a vascular closure device (including ExoSeal). Our lower rate of access site complications in repeat ExoSeal closure may also be due to appropriate hemostasis based on use of ultrasound for guidance of access.
In a systematic review of vascular closure systems, the mean hemostasis time was 7.6 min. 5 In the current study, this time was 7 min in repeat closure and thus was comparable to previous studies. In previous ExoSeal series, routine manual pressure after closure has been applied for 2 or 3 min.10,12 We performed light manual pressure for 5 min because of our use of mostly a femoral antegrade approach. Given the low rate of access site complications in this series, we may shorten the time for light manual pressure after vascular closure.
Limitations
The limitations of the study include its retrospective design at a single center. Also, several types of devices (drug-coated balloon, drug-eluting stent, and self-expandable nitinol stent) were used for different lesions, and procedural outcomes were not evaluated for each device and lesion because of the small sample size. We were also unable to assess the reasons for deployment failure because of the retrospective data collection. A lower body mass index (BMI) might influence the rates of a femoral antegrade approach and technical success of access, but again the small sample size prevented evaluation of the influence of BMI. We could not compare the outcomes of other closure devices with those of ExoSeal because we did not use the other closure devices in this study period.
Conclusion
Ultrasound-guided access facilitated higher technical success of repeat access and fewer access site complications in EVT with repeat use of ExoSeal, regardless of the interval between procedures.
Footnotes
Acknowledgments
We gratefully acknowledge the work of past and present members of our vascular team (ie, nurses, clinical engineers, radiologist, and medical secretaries). We especially thank Miss Haruka Ueno for data collection and for her support in data analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.