
Abstract
We present a 74-year-old gentleman, who presented with foot ischaemia requiring bilateral amputation in the absence of radiological signs of occlusive peripheral arterial disease. He was found to have COVID-19 pneumonitis and concurrent arterial and venous thromboemboli despite no initial respiratory symptoms or signs, nor pre-existing risk factors for cardiovascular disease. Patients who present with foot ischaemia with or without respiratory symptoms or signs warrant a high index of suspicion for COVID-19 infection, particularly in those with no predisposing risk factors.
Keywords
Introduction
The association between coronavirus disease 2019 (COVID-19) and venous and arterial thromboembolic complications is now well established, particularly in the intensive care unit (ICU) environment and in patients with pre-existing cardiovascular risk factors.1-4 Cutaneous lesions, such as ‘pseudo-chilblains,’ acral ischaemia or ‘COVID toes’, have also been widely documented in patients in the ICU setting, as well as in milder cases of COVID-19 in predominantly adolescent and young adult patients.5-7
We highlight a unique case of a 74-year-old gentleman who presented with bilateral foot ischaemia with no co-morbidities or smoking history. He was found to have COVID-19, concurrent arterial and venous thromboses with acute kidney and liver injury and was successfully treated with ward-based care and major amputation.
Case Presentation
A 74-year-old gentleman presented to the Accident and Emergency Department with a one-week history of reduced mobility due to bilateral foot pain and short-distance claudication. This was associated with discolouration and coldness of both feet. He denied having any respiratory symptoms or a diminished sense of smell or taste, and there was no history of trauma, rest pain, pain at night, sensory, motor or tissue loss. His body mass index was 25, and his past medical history was remarkable only for scalp psoriasis, laser eye treatment for a retinal tear and hearing loss. Notably, he was a never-smoker and had no history of thrombophilia, diabetes mellitus, cardio-, cerebro- or peripheral vascular disease. He also did not take any regular medications.
On examination, he had a normal temperature with no haemodynamic or respiratory compromise (temperature: 36.6 degrees Celsius; heart rate: 89 beats per minute; blood pressure: 116/93 mmHg; respiratory rate: 19 breaths per minute and oxygen saturation of 98% on room air). Both his feet were cold and discoloured (Figure 1) with reduced sensation over all toes and the soles of his feet, and impaired movement. He had palpable femoral and popliteal pulses bilaterally, but no distal pulses. Medical illustration photographic images, hospital admission Day 1. (A) Left foot, dorsum; (B) right foot, dorsum; and 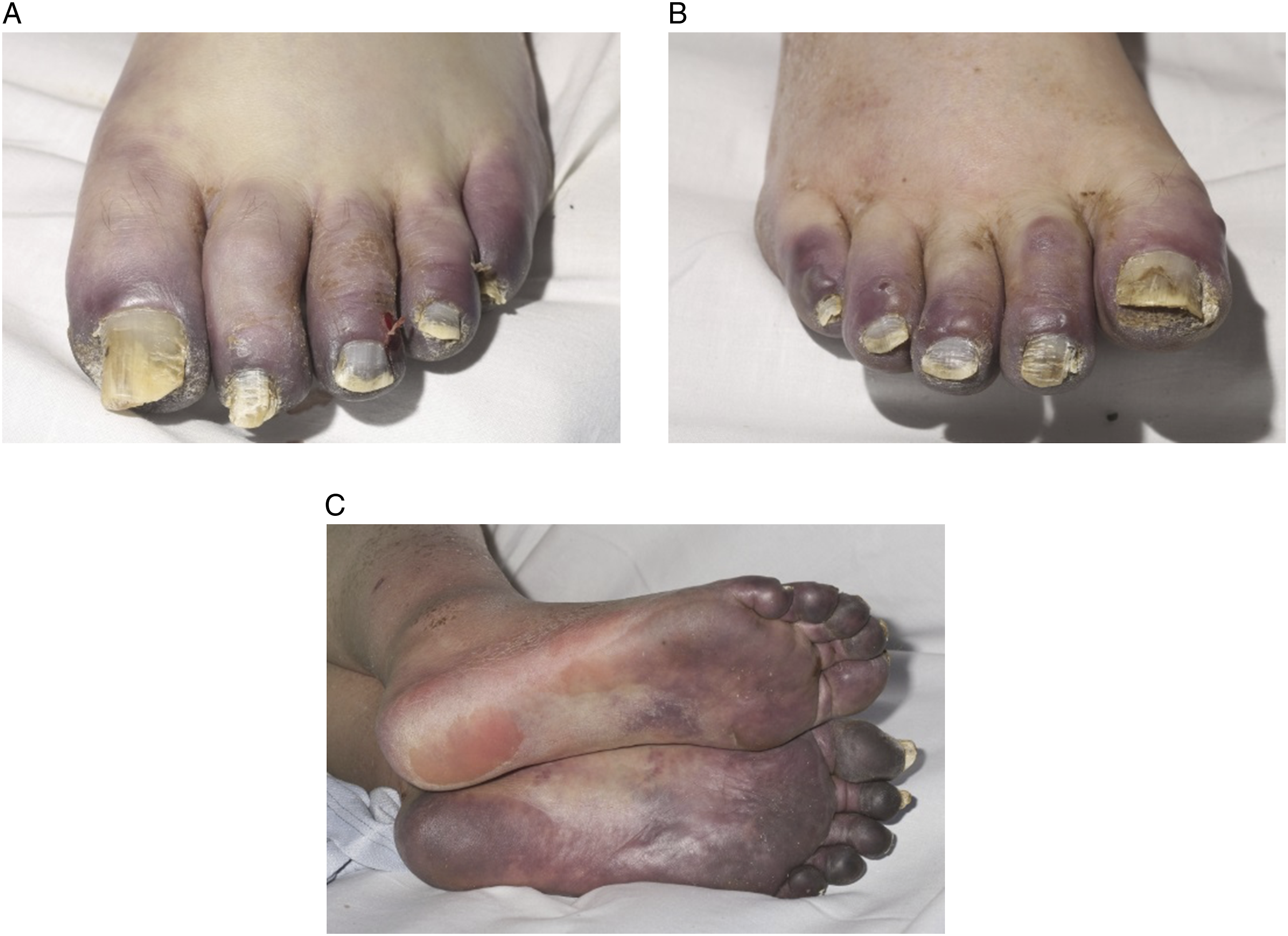
Investigations and screening were organised to identify a source of thromboembolism and to assess his peripheral vasculature. Electrocardiography showed normal sinus rhythm, and his blood results revealed markedly raised inflammatory markers, acute kidney and liver injury, and elevated prothrombin time and INR (international normalised ratio, Supplemental Table 1). Troponin I levels were normal, but D-dimer levels were not analysed. Transthoracic echocardiography showed no evidence of a cardiac thrombus nor left or right cardiac strain or failure. His valvular leaflets were thin and at most, minimally thickened, with no stenosis or regurgitation. Duplex ultrasound of his lower limbs demonstrated biphasic and triphasic waveforms throughout, and deep vein thrombosis (DVT) in his left popliteal and right peroneal veins, so ankle-brachial pressure indices were not possible.
SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) was confirmed on his admission nasopharyngeal swab 24 h later, using reverse-transcriptase polymerase chain reaction (rt-PCR) analysis. He subsequently developed a temperature of 38.2 degrees Celsius and a new oxygen requirement with normal respiratory rate (17 breaths per minute), but an oxygen saturation of 95% on 3 L of oxygen via nasal cannulae. The presence of serum SARS-CoV-2 immunoglobulin G antibodies was confirmed the following day. He was discussed at the vascular multi-disciplinary team meeting and started on therapeutic-dose (1.5 mg/kg once-daily) low-molecular weight heparin (LMWH) for his bilateral DVT and a glyceryl trinitrate (GTN) patch, which was placed on his feet.
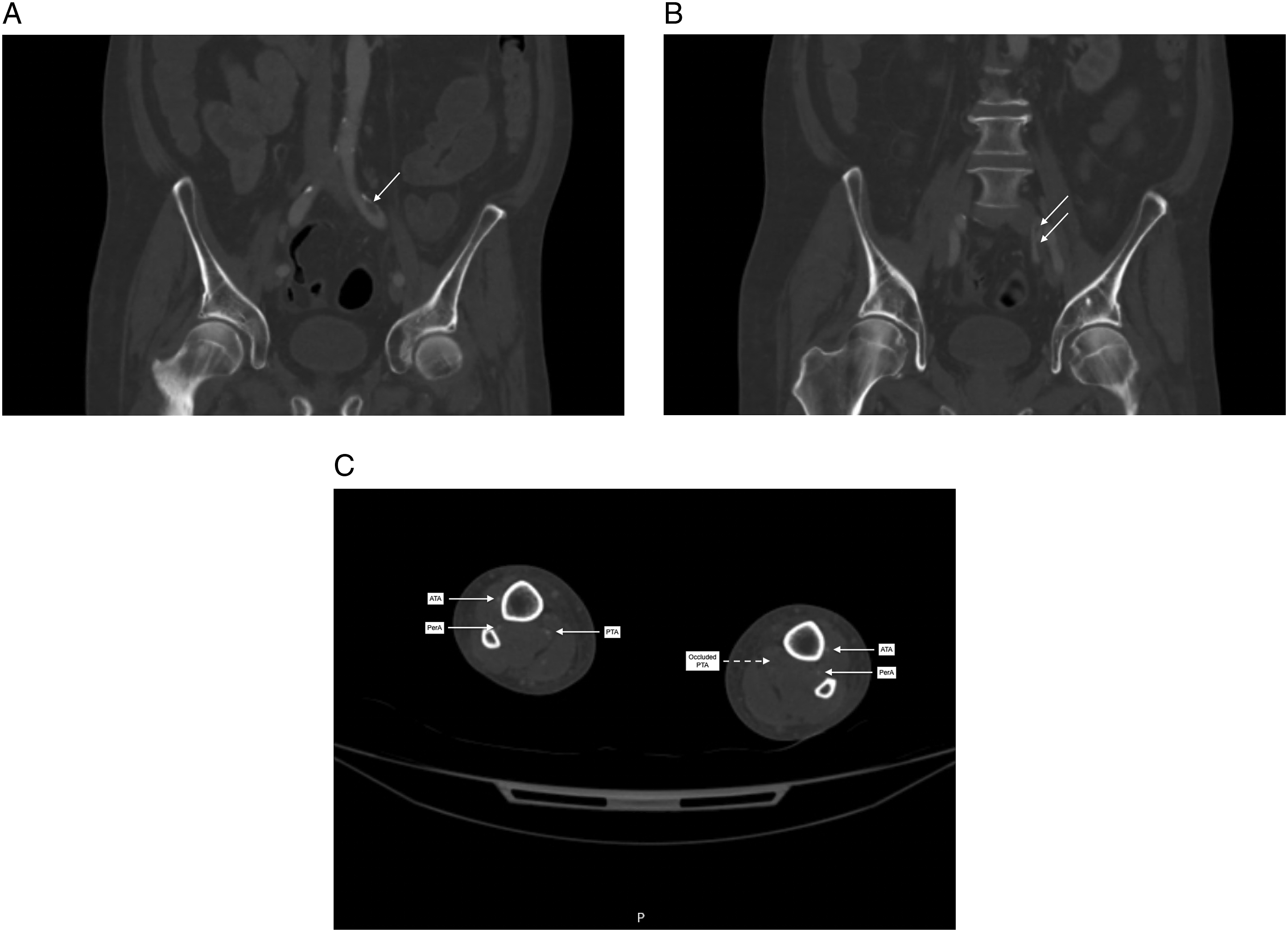
His thrombophilia and vasculitic screens came back negative but showed evidence of non-consumptive hypercoagulability (Supplemental Table 2). His glycosylated haemoglobin (HbA1c) was marginally elevated at 46 mmol/ml, which is not diagnostic for underlying diabetes mellitus. His chest X-ray was superseded by his need for full-body computed tomographic (CT) imaging so was not performed. CT scan of his thorax, abdomen and pelvis showed no evidence of underlying malignancy, but bilateral upper and lower lobar pulmonary emboli (PE) with extensive airspace consolidation in both lower lobes, in-keeping with COVID-19 pneumonitis (Figure 2). CT angiography of his whole aorta and lower limbs revealed a left-sided non-occlusive common iliac arterial thrombus (causing less than 50% stenosis) extending into the internal iliac artery and ipsilateral embolic occlusion of the distal posterior tibial artery (Figure 3). The rest of the arterial system was unremarkable, including his renal and hepatic arteries. Bilaterally, his external iliac; common, superficial and profunda femoral; and popliteal arteries were patent with three-vessel run-off to the ankle on the right and to the level of the distal posterior tibial artery occlusion on the left. Computed tomography of the thorax. Bilateral pulmonary emboli seen as filling defects in the pulmonary arteries (solid arrows) and bi-basal airspace consolidation suggesting COVID-19 pneumonitis (dashed arrows). Computed tomographic angiography of the aorta and lower limbs. (A) A non-occlusive thrombus of the left common iliac artery (solid arrow) causing less than 50% stenosis; (B) extending into the internal iliac artery (solid arrows) and (C) three-vessel run-off in the right lower limb and embolic occlusion of the left distal posterior tibial artery (dashed arrow). ATA, anterior tibial artery; PerA, peroneal artery; PTA, posterior tibial artery.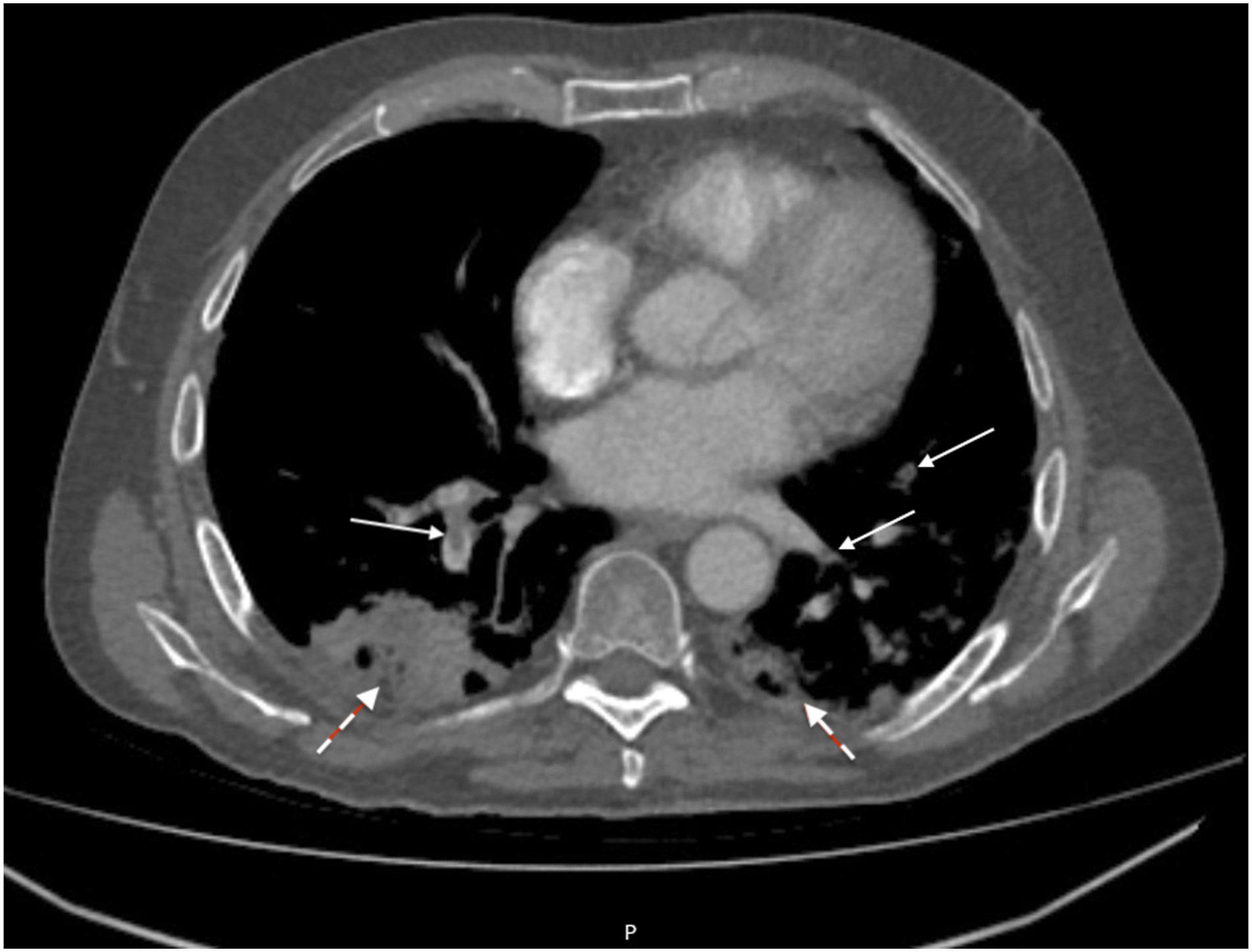
Further demarcation of his ischaemic feet was seen over the course of his inpatient stay and outpatient follow-up (Supplemental Figures 1, 2 and Figure 4). It did not progress, however, so he continued on a daily 1.5 mg/kg dose of LMWH whilst in hospital and was converted to apixaban on discharge. He otherwise made a full recovery from his COVID-19 pneumonia, venous thromboemboli, and acute renal and liver injury with ward-based care (Supplemental Table 1). He did not require any organ support, continuous positive-airway pressure (CPAP) ventilation or admission to high-dependency or intensive-level care. Community district nurse photographic images, taken on routine review at our patient’s residence on Day 81. 
Following a 31-day inpatient stay, he was discharged to a residential home on aspirin, a GTN patch and apixaban. He underwent elective left below-knee amputation and right transmetatarsal amputation four months later.
Discussion
Venous thromboembolism in the form of PE and DVT are common sequelae of COVID-191-4 with estimated incidences of 13.5% and 11.8%, respectively. 1 The same meta-analysis quotes much lower incidences of arterial thromboses, namely, acute coronary syndrome, including myocardial infarction (3.3%); cerebral infarcts (1.8%); mesenteric ischaemia (1.4%); and lower limb ischaemia (1.1%). The frequency with which these thromboembolic events occur is significantly higher in those with ‘severe’ COVID-19, therein defined as requiring ICU treatment.
The pathophysiology of COVID-19 coagulopathy is thought to arise from an inflammatory and pro-thrombotic cascade triggered by SARS-CoV-2 in the alveoli and pulmonary vasculature.2,8 It has been hypothesised that pulmonary thromboses may thus be secondary to local thrombosis, rather than embolisation from a DVT, for example. 1 This localised coagulopathy then develops and becomes systemic in progressive disease causing generalised macrovascular and microvascular thromboses, 2 that can occur directly in the cerebral, cardiac, gastrointestinal, hepatic, renal and lower limb vasculature.1,2,8,9
The risk of morbidity and mortality with SARS-CoV-2 and developing severe COVID-19 infection is increased in patients with a history of cardiovascular disease, respiratory disease, smoking, diabetes mellitus, hypertension, chronic kidney and chronic liver disease,1,3,10 sickle cell disease, cancer, obesity and pregnancy, 4 as well as non-modifiable factors, such as male sex and an age of over 65 years.4,11
An elevated D-dimer has been identified as an independent risk factor for poor outcome in COVID-19, including the need for mechanical ventilation, admission to the ICU and death.1,2,8,11 Patients with severe COVID-19 have been seen with D-dimers 2.5- to 9-fold higher than those with non-severe disease. 11 It is regrettable that our patient’s D-dimer level was not analysed, though he did have high levels of fibrinogen, factor VIIIc, von Willebrand factor (vWF) antigen and functional vWF, ristocetin co-factor (Supplemental Table 2), which have been associated with COVID-19-related hypercoagulability, particularly in severe disease. 8
We present a rare case, not only of concurrent venous and arterial thromboses in a patient who at presentation had asymptomatic or pre-symptomatic COVID-19 illness 4 but also of a patient with severe foot ischaemia in the absence of occlusive peripheral arterial disease on duplex ultrasound and CT angiography. The COVID-19 Treatment Guidelines Panel define ‘asymptomatic’ or ‘pre-symptomatic’ infections as those who have no symptoms that are consistent with COVID-19 at presentation but test positive for SARS-CoV-2 using a nucleic acid amplification test or antigen test. 4
Five classes of cutaneous lesions associated with COVID-19 infection have been described in a review of 1211 patients 5 in order of decreasing prevalence: pseudo-chilblains; rashes containing macules and papules; urticarial lesions; vesicular lesions and vaso-occlusive lesions. Vaso-occlusive lesions, which included acral ischaemia, were the least common (4.4%) but associated with severe disease requiring ICU treatment, increasing age and the lowest survival rate (78.9%). In antithesis to this, pseudo-chilblains, which resemble chilblains but lack documented exposure to chilblain risk factors or cold, were more common (40.9%), particularly in young adults, and had the highest survival rate (98.7%). Vaso-occlusive lesions tended to erupt at the same time as the development of COVID-19 symptoms in the majority of patients (68%), compared to after (24.5%) and before the onset of COVID-19 symptoms (3.8%).
Ordinarily, in a clinical picture of such profound acral ischaemia as in our patient’s case, one would expect to find a cause of hypercoagulability, such as malignancy, thrombophilia or vasculitis; and/or a source of arterial thromboemboli, such as atrial fibrillation, cardiac valvular vegetations or endocarditis, atherosclerosis, systemic sepsis or disseminated intravascular coagulopathy. This case supports growing evidence of the pathogenesis of in-situ thrombosis causing ischaemia and tissue injury.1,2,8,9 Results following histological analysis of vaso-occlusive lesions and COVID lung autopsy showed similar pathological processes with deposition of complement proteins C5b9 and C4d in a relatively inflammatory-poor environment. 12 These results suggest that microvascular injury and thrombosis seen in COVID-19 are secondary to complement activation. Due to reporting bias and limited numbers, more data are needed to determine whether factors, such as ethnicity, have a role in the pathogenesis of acral ischaemia.
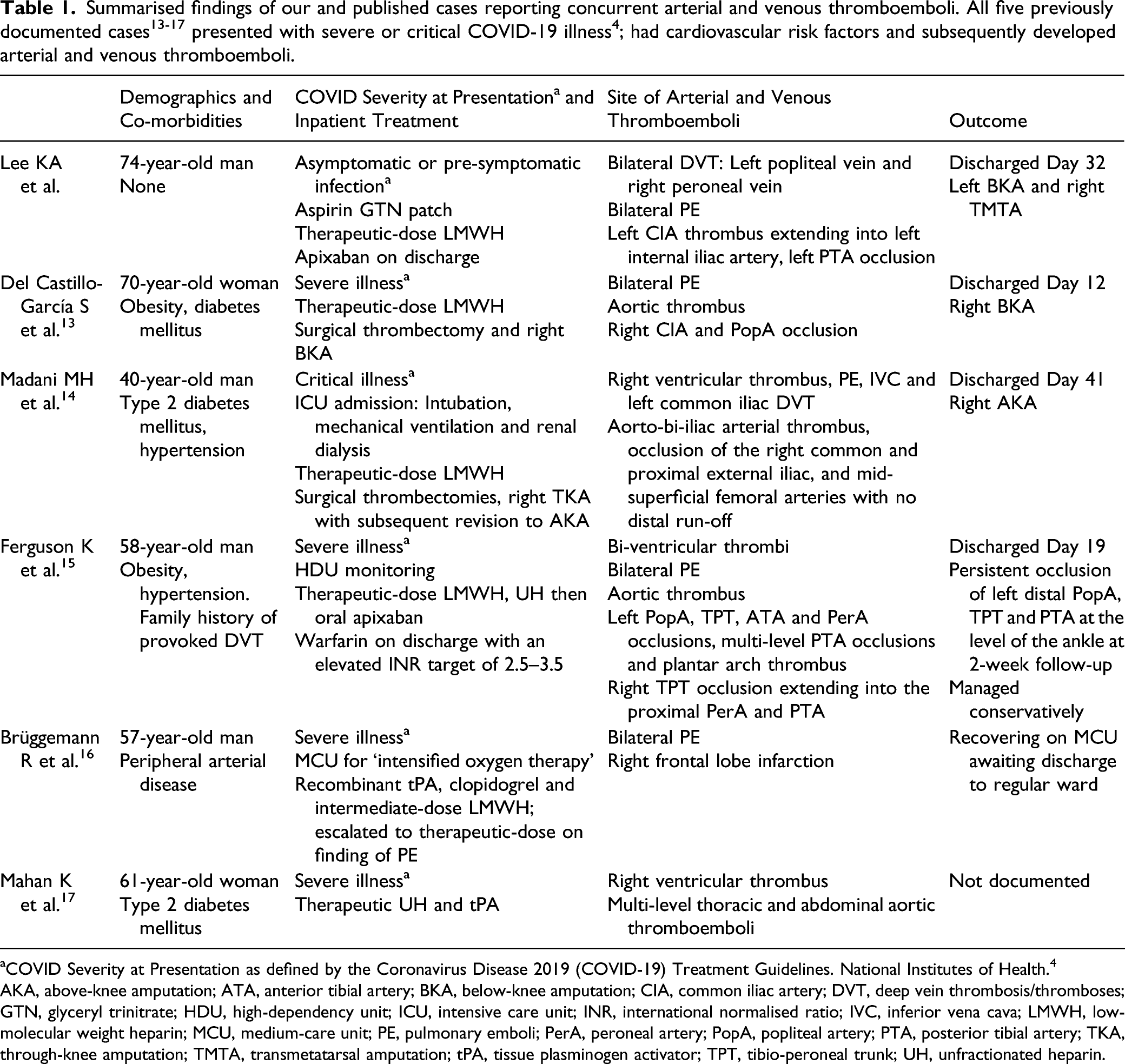
aCOVID Severity at Presentation as defined by the Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. 4
AKA, above-knee amputation; ATA, anterior tibial artery; BKA, below-knee amputation; CIA, common iliac artery; DVT, deep vein thrombosis/thromboses; GTN, glyceryl trinitrate; HDU, high-dependency unit; ICU, intensive care unit; INR, international normalised ratio; IVC, inferior vena cava; LMWH, low-molecular weight heparin; MCU, medium-care unit; PE, pulmonary emboli; PerA, peroneal artery; PopA, popliteal artery; PTA, posterior tibial artery; TKA, through-knee amputation; TMTA, transmetatarsal amputation; tPA, tissue plasminogen activator; TPT, tibio-peroneal trunk; UH, unfractionated heparin.
Conclusion
In patients presenting to primary and secondary care with digital discolouration, COVID-19 and its associated hypercoagulability must be considered as a differential diagnosis. It is essential to distinguish between those who have self-limiting cutaneous disease, such as pseudo-chilblains that predominantly affect children and young adults, 6 and those who have limb-threatening acral ischaemia secondary to thromboembolic complications of SARS-CoV-2. 7 A high index of suspicion must prevail in older patients even in the absence of respiratory symptoms or signs, or co-morbid risk factors.
Supplemental Material
sj-pdf-1-ves-10.1177_15385744211045600 – Supplemental Material for COVID Toes: Concurrent Lower Limb Arterial and Venous Thromboembolism in a Patient with COVID-19 Pneumonitis Presenting with Foot Ischaemia
Supplemental Material, sj-pdf-1-ves-10.1177_15385744211045600 for COVID Toes: Concurrent Lower Limb Arterial and Venous Thromboembolism in a Patient with COVID-19 Pneumonitis Presenting with Foot Ischaemia by Kathryn A. Lee, Richard S. McBride, Ranjeet Narlawar, Rebecca Myers and George A. Antoniou in Vascular and Endovascular Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.