
Abstract
Objective
This study aimed to evaluate the rate of asymptomatic bacterial infection of tunneled dialysis catheters (TDCs) removed due to maturation of native arteriovenous fistula (nAVF) or catheter dysfunction in hemodialysis patients with no clinically apparent infection.
Materials and Methods
A total of 229 patients (43.2% [n = 99] female and 56.8% [n = 130] male), who underwent hemodialysis through a TDC, were included in this study. Tip cultures of TDCs removed in an operating room and under sterile conditions were collected. All patients were asymptomatic for catheter infection and had not received antibiotic therapy for the last month.
Results
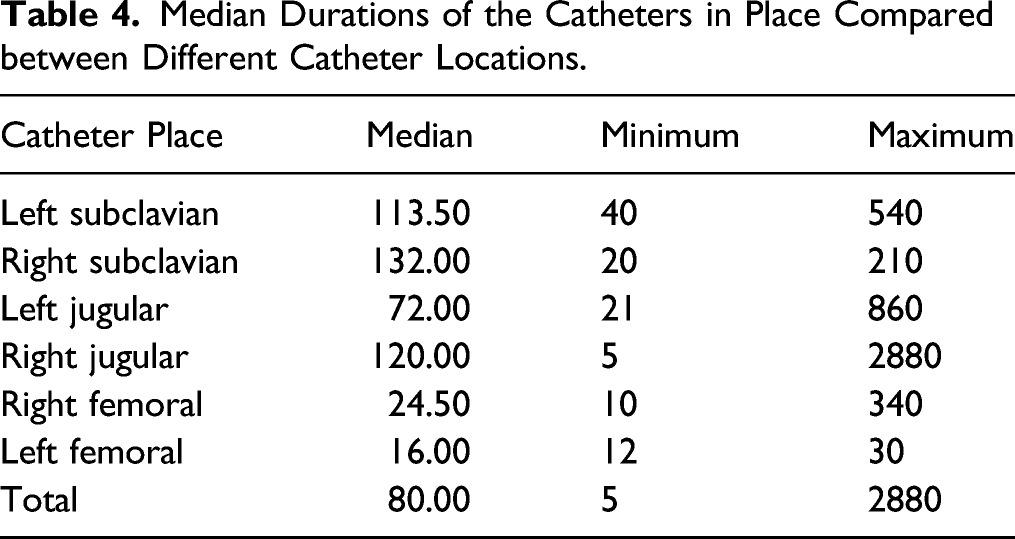
The median duration of catheterization was 80 days (min: 5, max: 2880). Bacterial growth was observed in a total of 62 (27.1%) patients. The most common microorganisms were Staphylococcus epidermidis and Staphylococcus aureus. The asymptomatic infection rate was highest in catheters placed through the right and left subclavian veins; however, this was not statistically significant due to the small number of patients. Placement and usage time of TDCs were found to be the most significant factors for bacterial growth in the catheter tip culture (P < .001).
Conclusion
Prolonged duration and use of the catheter is significant in terms of bacterial load. The use of TDC as vascular access in renal replacement therapy should be avoided as much as possible.
Keywords
Introduction
Despite the recommendations specified in the national guidelines and significant efforts by the nephrology community to reduce the use of tunneled dialysis catheters (TDCs), nearly 80% of patients initiate hemodialysis with a catheter. 1 Slightly more than half of these patients rely on a catheter as their mode of access after 4 months of treatment. 1 The use of TDCs is, unfortunately, associated with increased rates of infection, stenosis causing dysfunction in central veins, and formation of thrombus, as well as increased morbidity and mortality. 2 In 2004, the fistula-first breakthrough initiative (FFBI) set for an ambitious mandate to reduce the rate of TDCs and to increase arteriovenous fistula (AVF) placement to 65% by 2009, and currently, the prevalent AVF use has surpassed this goal (66%).3,4 The greatest unwanted consequence of FFBI is that 80% of patients still start hemodialysis with a TDC and furthermore, the use of TDCs after the initiation of hemodialysis treatment remains at undesired levels: 68.5% at 90 days and 18% at the end of 1 year. 3 According to the Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines which were updated in 2019, it is reasonable to have an AV access (AVF or AVG) in a patient requiring HD, when consistent with their ESKD Life-Plan and overall goals of care. KDOQI considers it reasonable in valid clinical circumstances to use tunneled CVCs for short-term or long-term durations for incident patients: AVF or AVG created but not ready for use and dialysis is required, acute transplant rejection or other complications requiring dialysis, PD patient with complications that require time-limited peritoneal rest or resolution of complication, patient has a living donor transplant confirmed with an operation date in the near future (e.g., < 90 days) but requires dialysis, and AVF or AVG complication such as major infiltration injury or cellulitis that results in temporary nonuse until the problem is resolved. 5 Again, according to the same guidelines for the diagnosis of catheter-related bloodstream infections (CRBSI), blood culture obtained from the arterial or venous CVC hub 3-fold higher count of colony-forming units (CFUs)/mm was compared with the peripheral venous blood culture. The blood culture from the CVC hub turning positive at least 2 hours before the peripheral blood culture; or the hemodialysis CVC tip growing the same microorganism as the peripheral venous culture. 5
This study aimed to investigate the growth rates in the bacterial culture of catheters removed due to catheter dysfunction or functional nAVF in patients, who underwent hemodialysis with TDCs and were asymptomatic for catheter infection, and some factors affecting these rates.
Methods
Study Design, Inclusion/Exclusion Criteria, and Ethics
This retrospective study evaluated the medical records of patients, for whom a permanent tunneled atrial catheter for hemodialysis was implanted within the period from August 2018 to August 2020 in Elazig Fethi Sekin City Hospital, Turkey. The study population consisted of 229 patients (43.2% [n = 99] female and 56.8% [n = 130] male). The mean age of the patients was 62.47 ± 13.46 years. The majority of the participants (84.7%) had comorbidities. Patients who underwent hemodialysis via TDC implanted in our clinic or at an external center were included in the study. The implantation time was learned from digital recordings of health ministry or hospital. The cultures of the catheters removed due to the development of nAVF or dysfunction of TDC were examined. Study inclusion criteria were having a TDC, regardless of which center it was implanted, and receiving hemodialysis through TDC. Those with active catheter infection, individuals who received antibiotic therapy in the last month, patients undergoing active cancer treatment, and those who rejected their data to be analyzed or did not provide consent for data analysis were excluded from the study.
The study was approved by the local university of the city, Fırat University non-interventional research ethics committee (2020/17-25). Before the procedure, an informed and signed consent form was obtained from the patient and the patient’s relatives and archived in the hospital paperback files of the patients. The investigation conforms to the principles outlined in the Declaration of Helsinki.
Collection of Catheter Culture
The tunneled catheters were removed by surgeons working in the Department of Cardiovascular Surgery either into the internal jugular, femoral, or subclavian vein. The catheter removal was performed under sterile conditions after local cleaning of the surgical incision site under operating room conditions. Standard monitoring procedures were performed after the patient was taken into the operating room. The surgical incision site was cleaned locally and was covered with sterile covers for the procedure. Local anesthesia was performed to dissect the cuff of the TDC from the subcutaneous tissue. The tip of the catheter removed using a small surgical set was held with an unused pick up available in the set and cut with unused scissors. Then, it was sent to the hospital’s microbiology laboratory under sterile conditions without waiting.
Statistics
The data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 25.0 software (SPSS Inc., Chicago, IL, USA). The results were presented as frequencies, percentages, medians (min-max), means, and standard deviations (SD). The Kolmogorov–Smirnov test was performed to test if the numerical variables were normally distributed. The independent samples t-test was used to compare data meeting parametric assumptions. The Mann-Whitney U test was used for skewed variables, and the chi-square test was used for categorical variables. A logistic regression analysis was performed to check for variables independently affecting culture positivity. A P value of < .05 was considered as statistically significant.
Results
Data for 229 participants were analyzed. Of the respondents, 99 (43.2%) were females and 130 (56.8%) were males. The mean age of the patients was 62.47 ± 13.46 years. Most of the participants (84.7%) had some co-morbidity.
Descriptive Findings
Descriptive Findings Concerning Catheter Place, Culture Results, and Reasons for Catheter Removal.
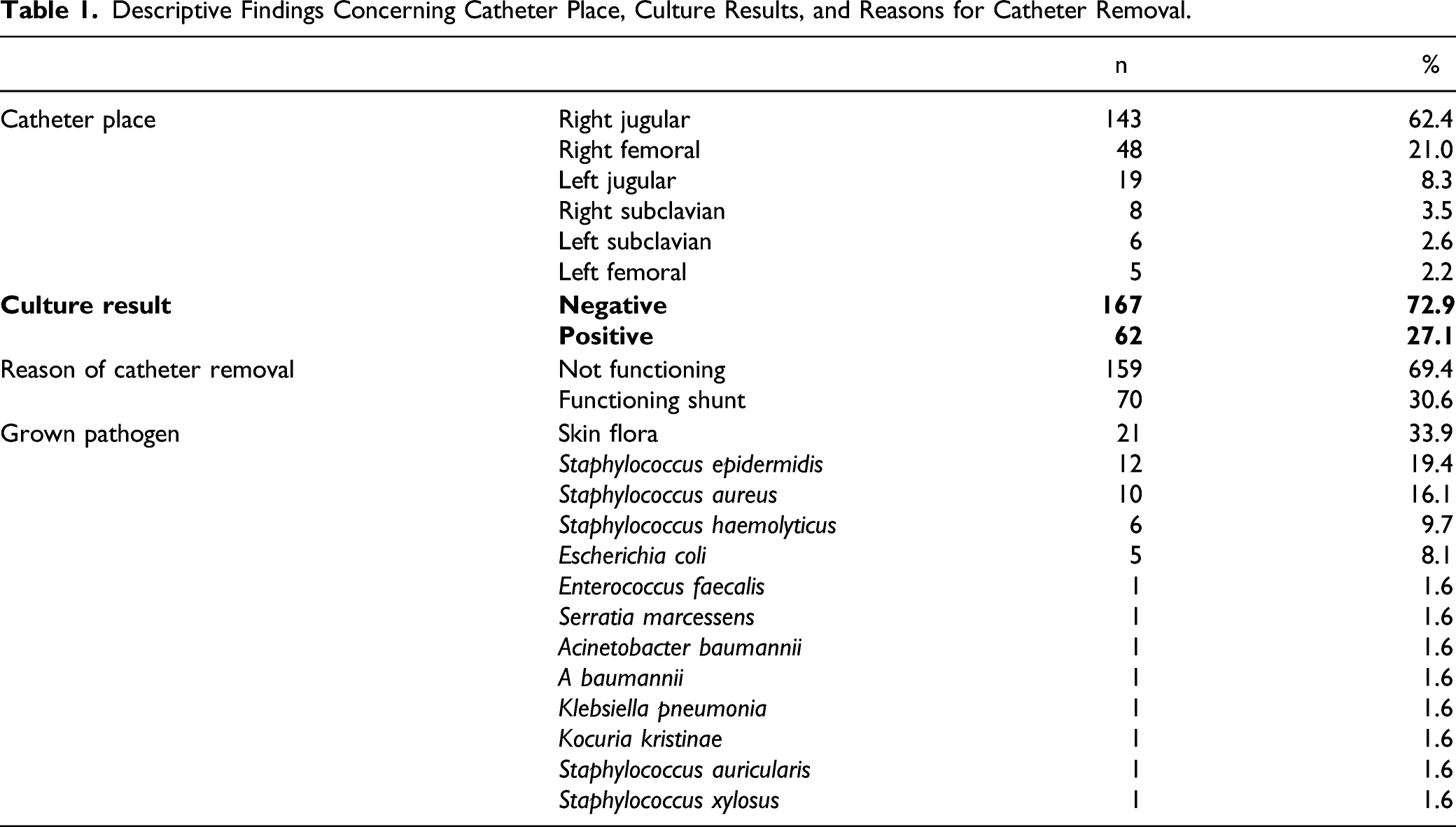
The median duration of catheters in place was 80 days (min. 5, max. 2880), while the median duration of CRF diagnosis was 4 years (min. .1, max. 20). The median duration of the active use of the AVF was 30 days (min. 10, max. 60).
Outcomes
Distribution of the Numerical Variables between the Culture-Positive and Culture-Negative Groups.
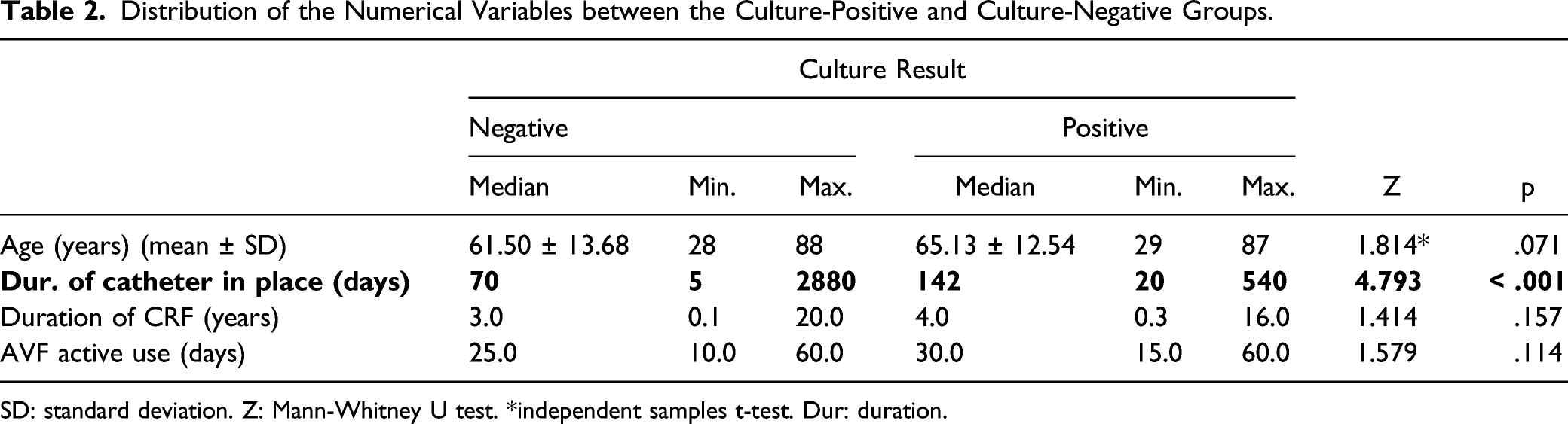
SD: standard deviation. Z: Mann-Whitney U test. *independent samples t-test. Dur: duration.
Distribution of the Categorical Variables between the Culture-Positive and Culture-Negative groups.
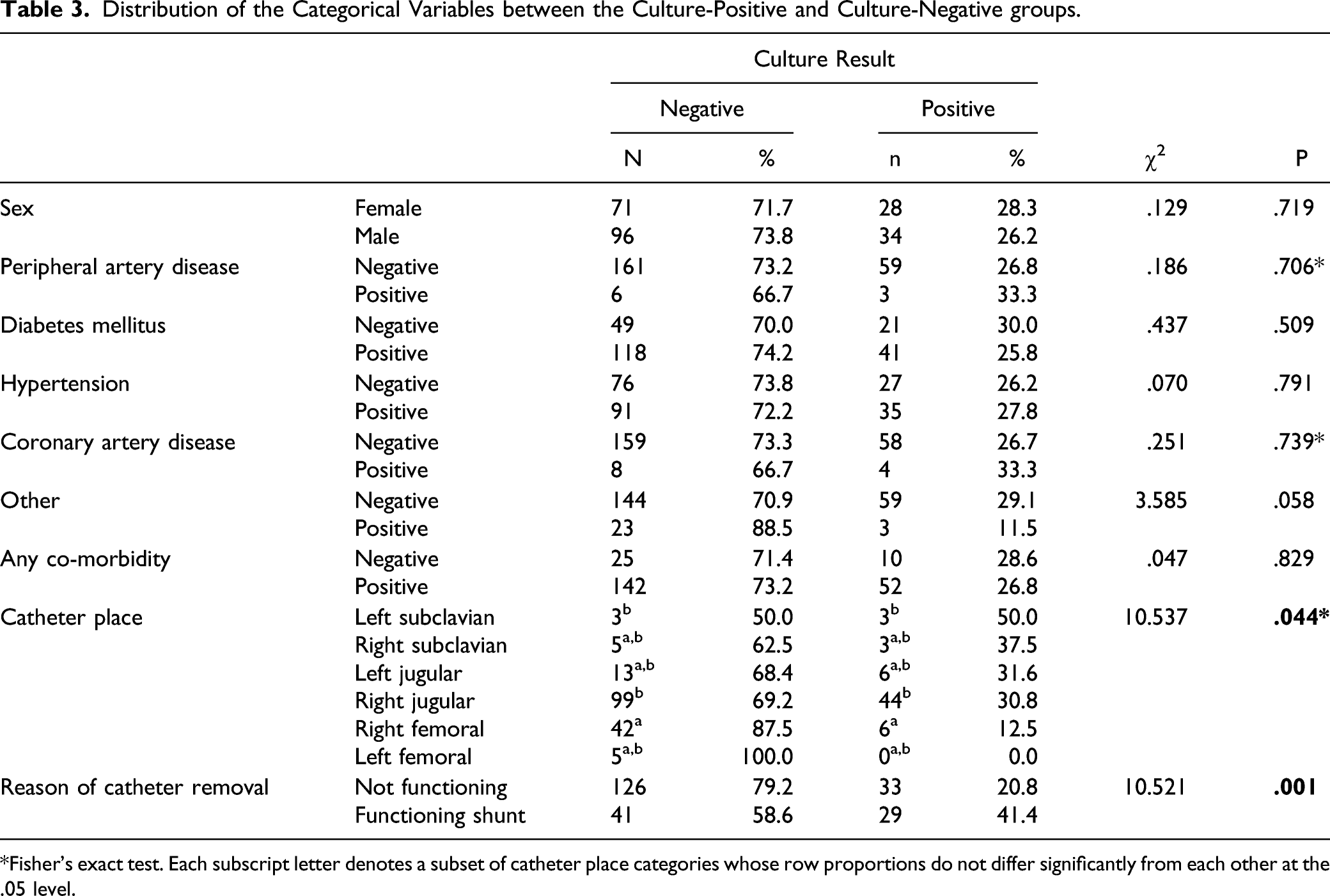
*Fisher’s exact test. Each subscript letter denotes a subset of catheter place categories whose row proportions do not differ significantly from each other at the .05 level.
Median Durations of the Catheters in Place Compared between Different Catheter Locations.
Logistic Regression Analysis Computer Output.

Discussion
All-cause mortality in the first 120 days is significantly higher in patients starting hemodialysis treatment with TDC instead of AVF. The crude all-cause mortality rate (deaths/100 patient-years; OR = 2.97, 95% CI: 2.17-4.06) was reported to be 2.76 for cardiovascular causes (OR = 1.84, 95% CI: 1.17-2.89) and 4.58 for infection-related causes (95% CI: 2.00-10.52).6,7 In a review conducted by Golestaneh and Mokrzycki in 2018, frequent use of TDC in hemodialysis patients led to increase in infection complications, hospitalization, and mortality. The authors have commented on clear strategies to prevent the development of such complications by avoiding and reducing the use of catheters. However, they have made a number of recommendations, including the use of antimicrobial locks to reduce catheter-related BSI (CRBSI) and hospitalization rates when the use of catheters is unavoidable. 8
Within 24 hours, all inserted catheters are colonized by microorganisms. 9 During the catheter hub manipulation, the surrounding skin flora or the hand flora of healthcare workers are introduced into the lumen. 10 Skin flora bacteria migrate along the outside of the catheter and can seed the bloodstream. A Dacron cuff is incorporated close to the hub of a tunneled dialysis catheter for prevention of bacterial growth. By inducing an inflammatory response, the cuff creates a fibrotic mechanical barrier against contamination. Ascending infection from the exit site may produce purulence to occur within the tunnel, necessitating removal of the catheter. Both externally and within the catheter lumen, bacteria forms biofilms and this forms the major source of catheter-related BSI. 11
Regardless of whether the patient is symptomatic or asymptomatic, bacterial load to growth occurs in 27.1% of the inserted TDCs, which can be implicated as one of the reasons for the high mortality rates due to TDC use in all the above-mentioned articles. It is not possible to rule out the human factor in hemodialysis applications. In hemodialysis treatment, both healthcare professionals performing the treatment, disposable treatment materials, solutions, comorbidities, and the hygiene status of the patient may be associated with bacterial deaths. 11 The right internal jugular vein is the most common site of TDC insertion. Although bacterial growth rates are high in catheters inserted through the right and left subclavian veins, an accurate statistical evaluation could not have been made due to the small number of these patients. The most significant correlation has been found to be between the duration and use of TDCs and bacterial growth. The most common microorganism was the skin flora and Staphylococcus species. In the review and meta-analysis conducted by Zhao et al. 12 in 2013, the authors evaluated 13 randomized controlled trials and reported that citrate locks of low to moderate concentrations, rather than high concentration, were superior to heparin locks in preventing CRBSI. The use of the antimicrobial lock is also recommended in cases where there is no alternative in terms of VA other than TDC.
The most important limitation of the present study is its single-center design. Renal replacement therapy is primarily a national and then a global problem. Good study planning can provide a more objective evaluation of the results obtained from multiple centers. As it would be unfounded to claim that none of the cultures with bacterial growth is contaminated, it is also not possible to say that all of them are contaminated. It is necessary to make an evaluation with a certain project in multiple centers to minimize the human factor.
Conclusion
Since the number of patients receiving renal replacement therapy is increasing gradually, TDCs have become a central problem in the field of nephrology. The best prophylaxis still remains avoidance of catheters. One of the reasons for the high mortality rates of using TDCs as VA in renal replacement therapy may be the bacterial load of the catheter, which is closely associated with the duration of use. Moreover, catheters made of materials resistant to infection and thrombosis in terms of technology and bioengineering can be developed. However, particularly inexperienced surgeons should be more aware of the VA they are dealing with frequently and patient approaches should be determined in accordance with recommendations specified in the national and international guidelines. Almost a third of TDCs in asymptomatic ESRD patients is infected, and the rate is increased with increased dwell time. If proven in additional studies, this will have major clinical implications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.