
Abstract
Introduction
Coarctation of the aorta (CoA) occurs in 4 of 10,000 live births. Aberrant right subclavian artery (ARSA) is the abnormal embryological development of the usual aortic arch branching pattern. This condition has an incidence of .4–.7%.1,2 Isolated CoA is seen in 82% of the cases, but it may be associated with other anomalies in other cases. One percent of patients with CoA have concurrent ARSA. 3 A few previous reports have described both open and hybrid treatment strategies for concurrent CoA and ARSA;4-6 however, every patient must be carefully examined for surgical planning, which depends on the site of coarctation and origin of both the subclavian arteries.
Herein, we describe a case of CoA and ARSA treated with a hybrid procedure comprising ARSA ligation and subclavian to carotid transposition followed by thoracic endovascular aortic repair (TEVAR). Informed consent was obtained from the patient for publication of the case report and images.
Case Report
A 35-year-old woman with uncontrolled hypertension treated with losartan and hydrochlorothiazide was found to have decreased lower extremity pulse and blood pressure. The resting CoA gradient was >60 mm Hg. Contrast-enhanced computed tomography (CT) angiography of the thorax demonstrated CoA located at the insertion of the ductus arteriosus, slightly distal to the left subclavian artery (Figure 1). Preoperative contrast-enhanced computed tomography (CT) angiography (left) and three-dimensional reconstruction of a CT scan (right) showing coarctation of the aorta (arrow) located at the insertion of the ductus arteriosus.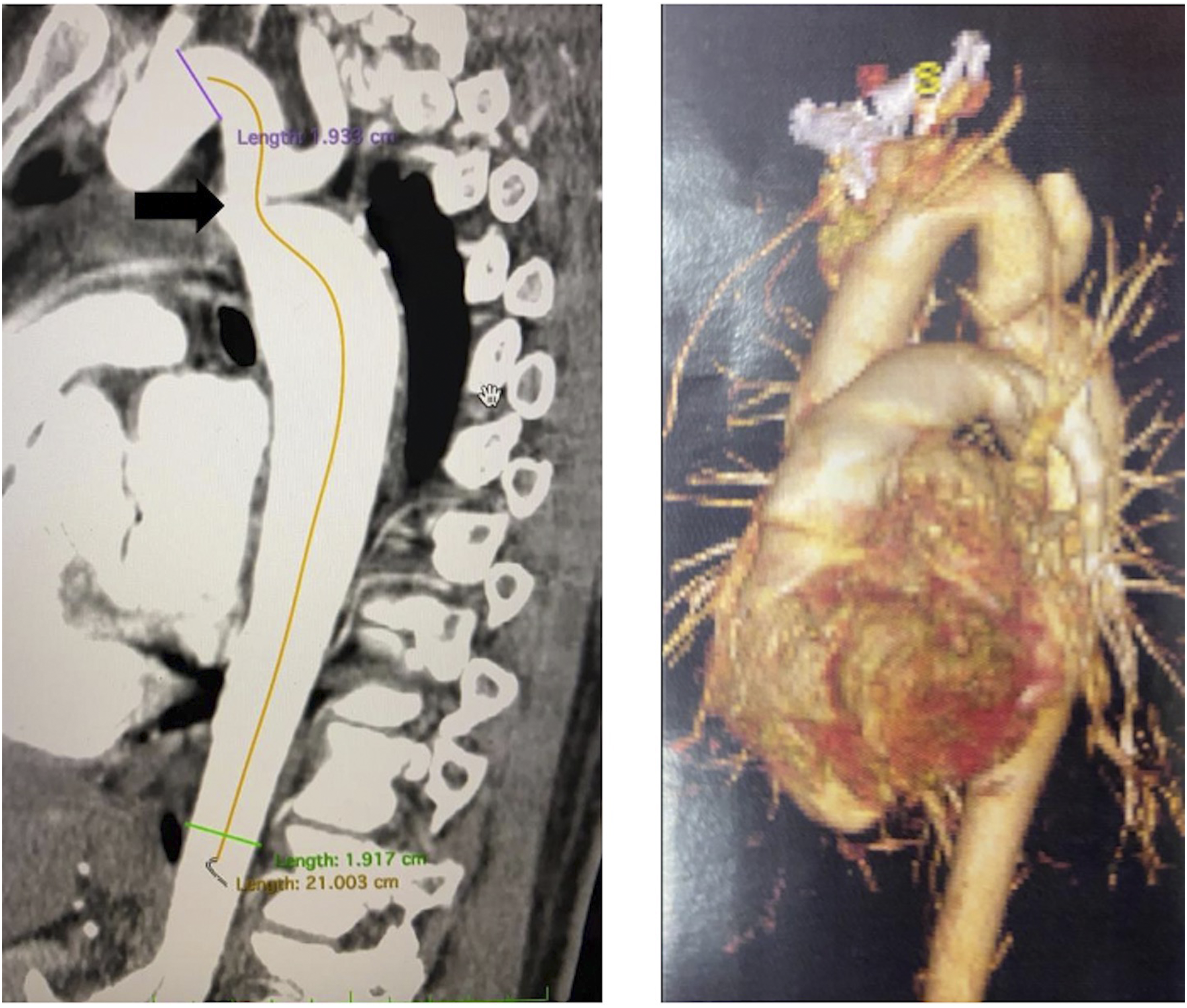
A hybrid procedure was planned. The surgical approach involved percutaneous access to the right common femoral artery (CFA) for a diagnostic angiogram (Figure 2). Diagnostic angiogram showing coarctation of the aorta (arrow head) and aberrant right subclavian artery (arrow).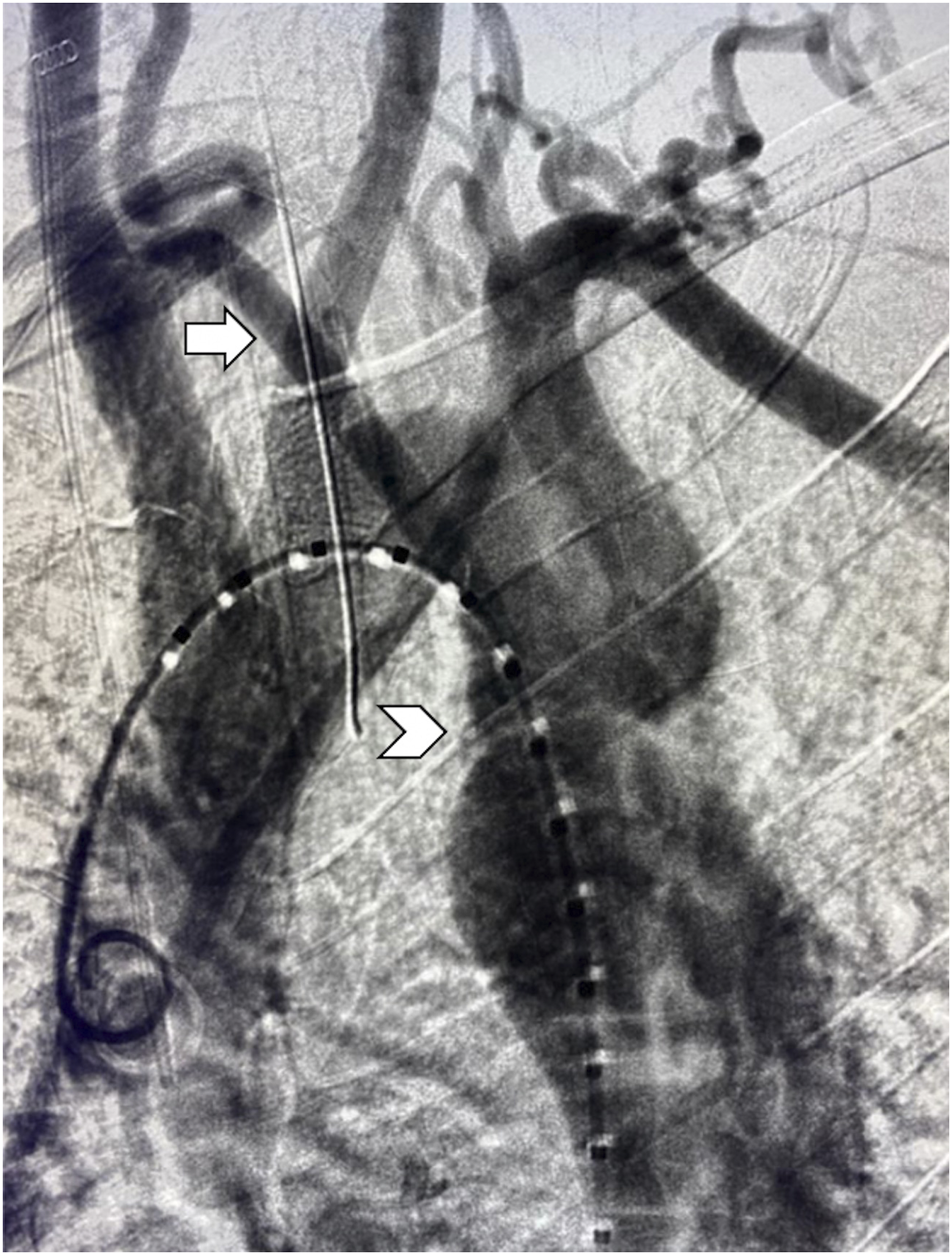
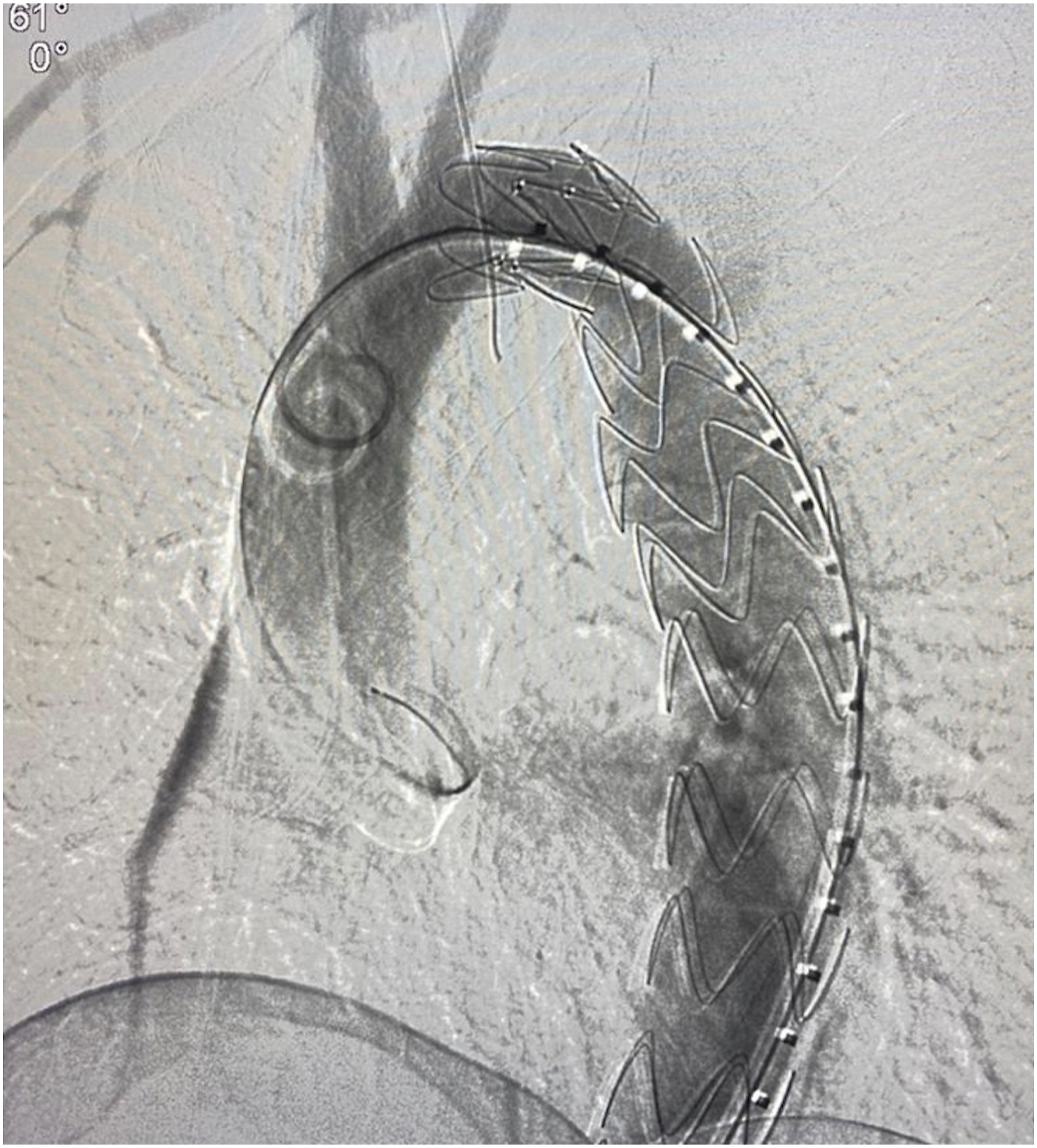
For the surgical procedure, a right supraclavicular incision (8 cm) was taken, following by division and over-sewing of the proximal ARSA and subclavian to carotid transposition with an end-to-side anastomosis (Figure 3). The right vertebral artery was preserved; it originated from the right common carotid artery. Subsequently, TEVAR was performed using a Zenith (Cook Medical, Bloomington, Indiana) 28 mm × 20 mm stent (Figure 4). The stent size was selected based on preoperatively measured aortic values (Figure 1) and the stent sizes available at our center at the time of the study. The graft was dilated after deployment for optimization of the de-coarctation procedure. Right supraclavicular incision showing the right common carotid artery (left). Division and over-sewing of the proximal aberrant right subclavian artery (right) to complete a subclavian to carotid transposition with an end-to-side anastomosis. Angiogram showing TEVAR performed using a Zenith (Cook Medical, Bloomington, Indiana) 28 mm × 20 mm stent.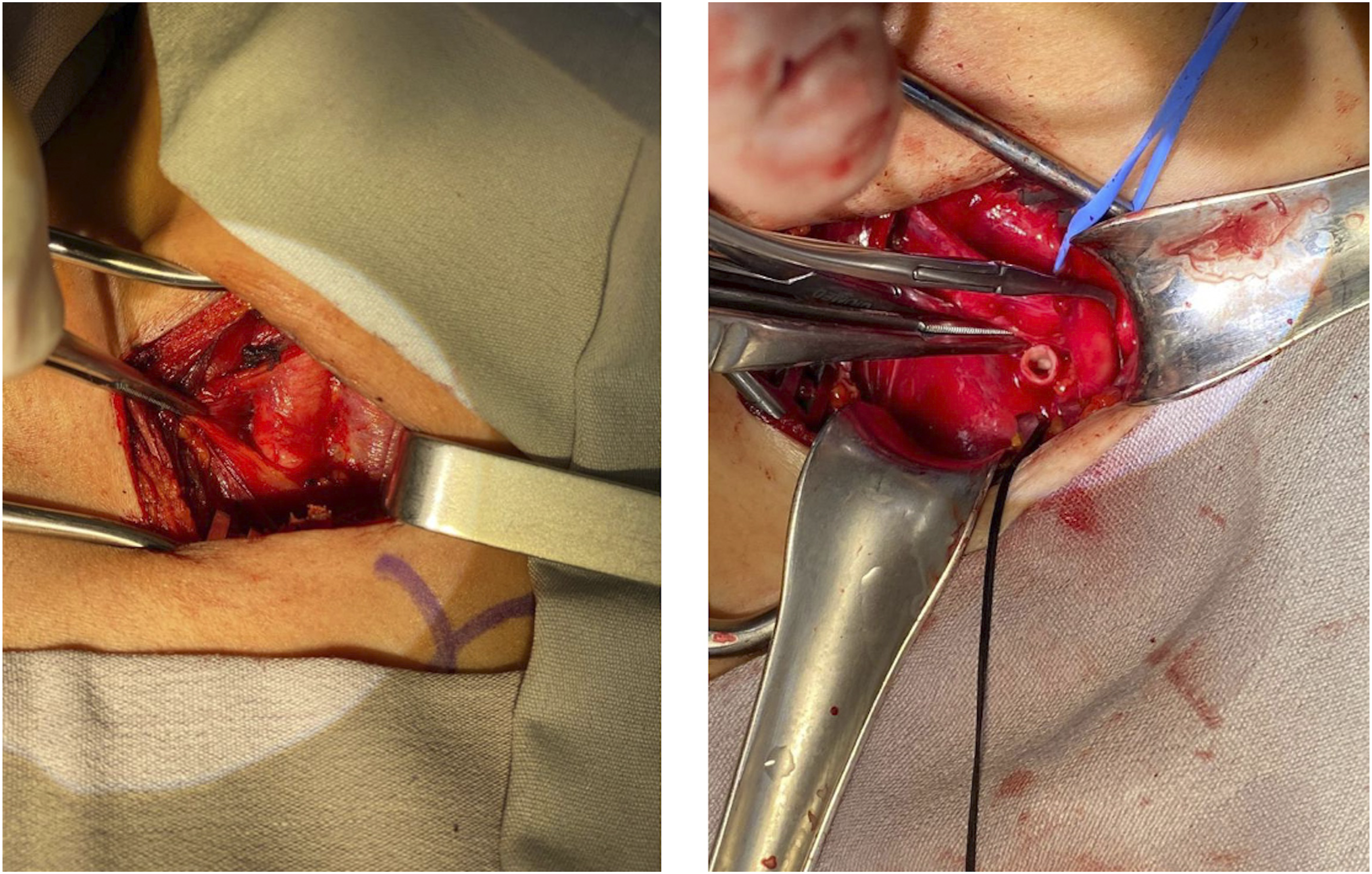
At the end of the procedure, the CFA was closed with a percutaneous arterial closure device (Angio-Seal®, St. Jude Medical, St. Paul, MN, United States).
No complications occurred during surgery. The postoperative course was uneventful; the patient was discharged on postoperative day two.
At the 3-month follow-up, the patient was asymptomatic with a normal physical exam. The patient’s left arm was mildly fatigable; however, there were no signs of vascular or vertebrobasilar insufficiency.
CT angiography 6 months postoperatively showed a patent right subclavian to carotid transposition and patent aortic graft (Figure 5). Three-dimensional reconstruction of CT angiography of the neck and chest at the 6-month follow-up showing a patent right subclavian to carotid transposition and TEVAR.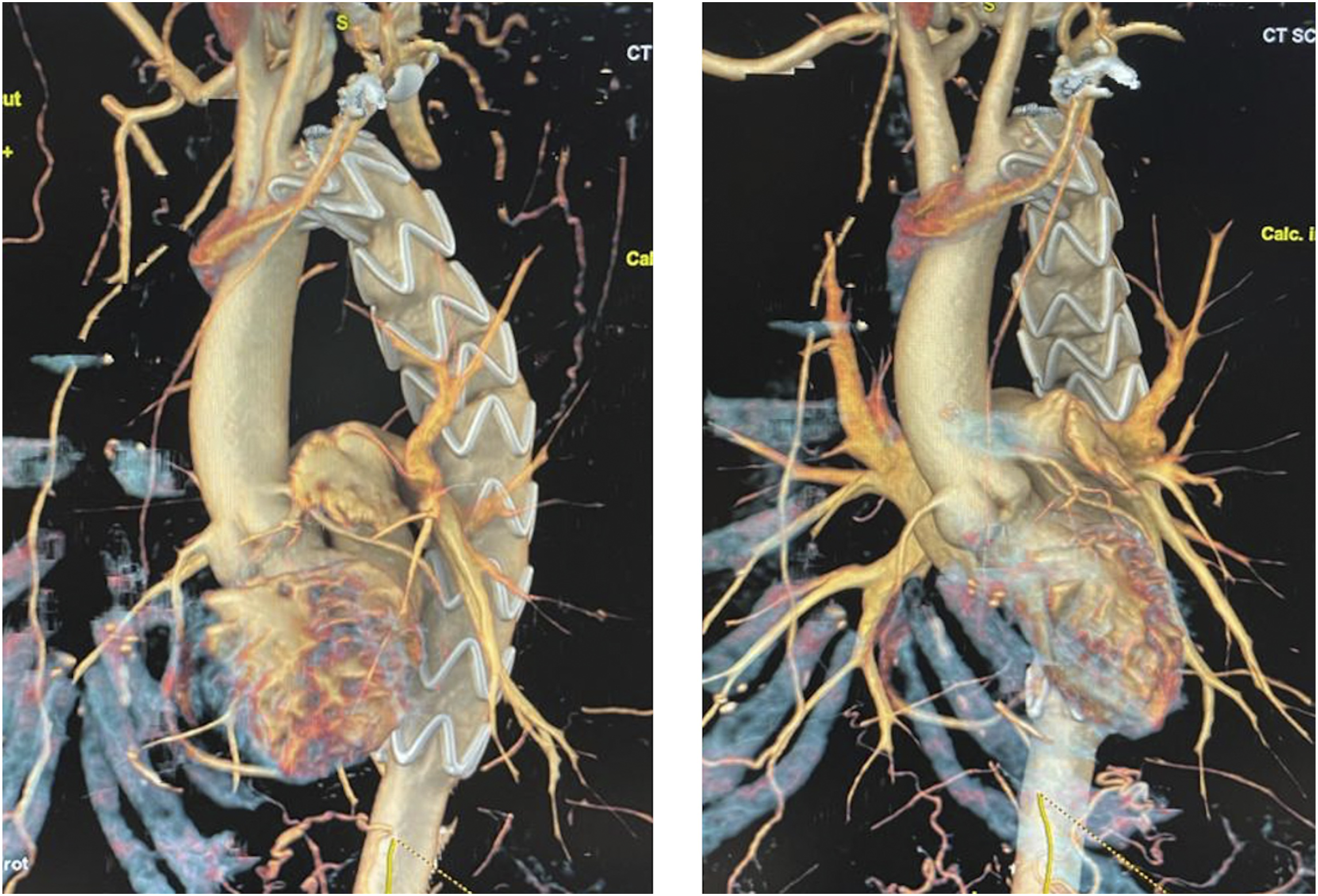
Discussion
CoA is a relatively common defect; it occurs in 4 per 10,000 live births and accounts for 4–8% of congenital heart defects, with an incidence that may be underestimated. 7 It is more common in females and caucasians. 7
Aortic development starts at the third week of gestation, and the complex development sequence may result in aortic arch anomalies, which can occur in isolation (82%) or are associated with several arch variations or structural congenital heart disease. 8
The primitive aorta forms from a paired ventral and dorsal segment with six paired aortic arches in between. The aortic arch develops after the regression of certain primitive arches regression and the persistence of others. 8 The first, second, and fifth aortic arches disappear during development. The third arch, known as the carotid arch, forms the bilateral common carotid arteries. The proximal and distal parts of the right subclavian artery are formed by the proximal right fourth arch and seven intersegmental arteries, respectively. The left fourth arch forms the definitive adult aortic arch. The sixth arch forms the bilateral pulmonary arteries and the ductus arteriosus. The left ductus arteriosus usually closes during the first days of life and becomes the ligamentum arteriosum. 9
The pathogenesis of CoA is believed to be an abnormal migration of ductal tissue into the aortic wall, which results in constriction. Another theory for pathogenesis of CoA is reduced intrauterine blood flow with a reduction in flow across the arch, which may cause underdevelopment and partial obstruction once the ductus arteriosus closes. 10
The most common anomaly concurrent with CoA is bicuspid aortic valve, occurring in 60% of cases. 3 Other cardiac defects associated with CoA include arch hypoplasia, ventricular septal defect, mitral valve abnormalities, and patent ductus arteriosus (PDAs). CoA is associated with ARSA in up to 1% of patients.3,11
ARSA results from involution of the fourth aortic arch and cranial part of the right dorsal aorta, along with persistence of the seventh intersegmental artery. The distal right dorsal aorta and the seventh intersegmental artery form the ARSA. 12
ARSA was first described by Hunauld in 1735 based on autopsy studies. 13 In 1761, Bayford described a patient with dysphagia; on autopsy, he observed an ARSA running anterior to the esophagus and causing compression. 14 He named the condition “dysphagia lusoria” (from “lusus naturae,” meaning dysphagia from “freaks of nature”). 14
ARSA can present as an isolated anomaly or it can be associated with other congenital cardiac malformations such as PDA, CoA, and carotid (20%) or vertebral anomalies (15.7%), as observed in this case. 15
The majority of patients with ARSA are asymptomatic; 10% may present with dysphagia or chest pain in the fourth or fifth decade of life. 12
In contrast, the majority of patients with complex CoA (CoA accompanied by other cardiac defects) are diagnosed during infancy due to hemodynamic compromise.
Undiagnosed adults with CoA are commonly asymptomatic; the condition is discovered during physical examination and additional work-up for systemic hypertension. Systolic pressure is generally higher in the arms than in the legs. Diastolic pressure usually does not differ, resulting in a widened pulse pressure in the arms. 16
The origin of the left subclavian artery is generally proximal to the coarctation. The origin of the left subclavian artery is rarely reported and can be either proximal or distal to the CoA site. 6 Herein, we observed that the ARSA was located proximal to the CoA site, which is commonly seen in CoA. When the ARSA is located distal to the CoA, the right arm, and leg may be equally decreased, which may make the condition challenging to diagnose.
It is recommended that the diagnosis of CoA in adults be confirmed by cardiovascular magnetic resonance imaging or computed tomography angiography (CTA), which helps identify the location and size of CoA and serves as a valuable preoperative tool for anatomic data prior to intervention. 17
Treatment of CoA is indicated for patients with a peak-to-peak gradient of >20 mm Hg, significant collateral flow, coarctation attributed systemic hypertension, or heart failure. 18
Several surgical techniques have been used for CoA repair, including the application of ARSA as a flap analogous to the subclavian flap technique.19,20
In adults, the treatment of choice is transcatheter intervention with stent placement, which has shown lower rates of recurrence and wall injury compared to those of balloon angioplasty alone.17,21 The latter is reserved for patients in whom stent placement is not feasible and those are not candidates for surgical intervention. 17
Endovascular treatment for CoA includes controlled tearing of the intima and media. Post-procedure adverse effects include aneurysm, recurrence of CoA, and aortic rupture. Significant aortic wall injury has been reported in only 2% of patients when angioplasty is combined with stent placement; this rate is significantly lower than that with balloon angioplasty alone. 22
It has been reported that TEVAR grafts for CoA must be oversized in the proximal aorta because of its tortuous anatomy and the proximal-distal aortic size mismatch. 23 The landing zone requires a greater radial force in the proximal stent; therefore, we used a stent with 20% oversizing. Lala et al 23 recently reported that there was no associated infolding at the proximal landing zone or at the site of coarctation despite oversizing.
The length of coverage is assessed using preoperative imaging. Permanent spinal cord ischemia and paraplegia is reported in up to 4–5% of patients who undergo TEVAR. 24 The factors predisposing to these conditions include coverage of >20 cm of descending thoracic aorta and a lack of collateral vessels to the spine. The stent size for our patient was selected based on preoperative imaging (measured aortic values and good collateral vessels) and the stents available at our center.
A few updated reports about treatment for concomitant CoA and ARSA have been published.4-6,25 When planning a surgical intervention for CoA with ARSA, careful preoperative evaluation of the complete aortic arch anatomy must be performed. 26 CTA helps to identify the origin of both the subclavian arteries in relation to the coarctation, along with the origin of vertebral arteries, aneurysm degeneration, or concomitant arch anomalies.
Failure to accurately identify the origin of the right subclavian artery may lead to occlusion after stent placement and postoperative subclavian steal syndrome. 6
During TEVAR, revascularization of the left subclavian artery was recommended by the Society of Vascular Surgery for non-emergency TEVAR; however, this recommendation was based on low quality of evidence. 27 To date, no evidence has been collected to support routine revascularization of the left subclavian artery.28,29 This decision is best based on patient-specific anatomy and circumstances where perfusion is compromised. 27 We chose not to perform a left subclavian to carotid transposition, and performed close patient follow-up to identify possible vascular symptoms of left arm ischemia or subclavian steal syndrome. Our patient continued to have no associated complications 8 months postoperatively.
TEVAR for adults with CoA has a 100% technical success rate and a reported 3-year survival rate of 95%. 23
Thus, an aortic endograft can safely treat CoA, and ARSA can be successfully treated with a subclavian to carotid transposition using a supraclavicular approach.
Conclusion
Patients with CoA should be thoroughly examined before surgical planning. A tailored surgical treatment approach is required for such patients, considering the possible coexistence of other congenital aortic arch defects, such as ARSA. Hybrid repair, when feasible, is a superior surgical approach to others, and causes fewer complications.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
Informed consent has been obtained from the patient for publication of the case report.