
Abstract
Objective
In this systematic review and meta-analysis, we aimed to compare drug-coated balloon (DCB) to drug-eluting stent (DES) in patients with femoropopliteal lesions in terms of restenosis, target lesion revascularization (TLR), and mortality.
Methods
A comprehensive literature search was performed through PubMed, Scopus, and Embase databases. The intervention group was patients receiving percutaneous balloon angioplasty using the DCB. The control group was patients receiving percutaneous intervention using the DES. The primary outcome was restenosis, and the secondary outcomes were TLR and mortality.
Results
There were 4 studies comprising 812 patients (906 lesions) included in this systematic review and meta-analysis. The rate of restenosis was .19 [.13, .26] in DCB and .24 [.20, .28] in DES. There was a trend toward lower rate of restenosis (OR .73 [.52, 1.03], P = .074; I2: 46.3%) for DCB use compared to DES use. The rate of TLR was .11 [.08, .14] in DCB and .17 [.14, .21] in DES. TLR was lower (OR .61 [.41, .92], P = .017; I2: 1.2%) in the DCB group compared to the DES group. There were no significant differences in mortality (OR 1.38 [.78, 2.44], P = .268; I2: 0%) among the two groups. Meta-regression analysis showed that the rate of restenosis in DCB in this pooled analysis was affected by sex (reference: male, coefficient −.004, P = .009), smoking (coefficient: .003, P = .010), and total occlusion (coefficient: .008, P = .004).
Conclusion
DCB use in patients with femoropopliteal lesion was associated with similar rate of restenosis, lower TLR, and similar mortality rate compared to DES use.
Introduction
Peripheral artery disease (PAD) in the lower extremity compromises blood supply and is a major cause of limb amputation worldwide. 1 Endovascular intervention is integral for salvaging ischemic limbs; nevertheless, restenosis of the lesion remains a significant issue in this field.1-5 The outcome in patients receiving femoropopliteal artery endovascular interventions improved with the use of drug-coated balloon (DCB) and drug-eluting stents (DES), which are superior to bare metal stents or plain old balloon angioplasty in the treatment of femoropopliteal artery disease.6,7
Both DCB and DES are frequently used; however, head-to-head comparison between them showed varying results. These might be caused by several factors, including the characteristics of patients enrolled in the study and the inadequate statistical power due to the small sample size. Meta-analysis is a method that can be used to pool the results of the studies in order to obtain a larger sample size. This systematic review and meta-analysis aimed to compare DCB to DES in patients with femoropopliteal lesions in terms of restenosis, target lesion revascularization (TLR), and mortality. We also aimed to assess factors that may affect the rate of restenosis in patients undergoing endovascular intervention with DCB and DEB.
Methods
This is a Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) compliant systematic review and meta-analysis (PROSPERO ID: CRD42021247788).
Search Strategy and Study Selection
A comprehensive literature search was performed through PubMed, Scopus, and Embase databases from the inception of databases until April 8, 2021 with the terms “(drug-coated balloon OR drug-eluting balloon OR paclitaxel-coated balloon OR DEB OR DCB) AND (drug-eluting stent OR DES) AND (peripheral artery disease OR peripheral vascular disease OR femoropopliteal disease) AND (percutaneous revascularization OR angioplasty OR balloon angioplasty OR revascularization)”. Two independent authors performed screening of title/abstracts, and the eligible articles based on the inclusion and exclusion criteria were collected. Discrepancies during the literature search and study selection were resolved by discussion.
Intervention and Outcome
The intervention group was patients receiving percutaneous balloon angioplasty using the DCB. The control group was patients receiving percutaneous intervention using the DES. The primary outcome was restenosis, defined as: 1) Peak velocity ≥180 cm/s or a lesion/adjacent segment velocity ratio ≥2.4 by duplex ultrasound, or 2) absence of significant (≥50%) restenosis from computed tomographic angiography, conventional angiography. The pooled effect estimate was odds ratio (OR). The secondary outcomes were TLR and mortality. The TLR was defined as re-intervention performed for ≥50% stenosis confirmed by angiography. Mortality was defined as clinically validated death. The pooled effect estimate was ORs.
Inclusion and Exclusion Criteria
Studies that met all the following criteria were included: 1) randomized controlled trials (RCTs) or observational studies comparing DCB and DES in femoropopliteal lesion endovascular intervention and 2) reporting either a) restenosis or b) TLR or c) mortality.
Studies that met one of the following criteria were excluded: 1) pre-prints, 2) abstracts-only publication and conference papers, 3) reviews, and 4) editorial/letter/commentaries. There is no language limitation
Data Extraction
Data extraction was performed by 2 independent authors, and discrepancies were resolved through discussion. The data of interests were the first author, year of publication, study design, details of the DCB and DES used, sample size, age, sex, diabetes, hypertension, smoking, coronary artery disease, renal insufficiency, popliteal lesion, total length of lesion, presence of severe calcification, and total occlusion.
Risk of Bias Assessment
Two independent authors used Cochrane Risk of Bias Assessment for the RCTs and Newcastle-Ottawa Scale (NOS) for the observational studies to assess the risk of bias of the included studies.
Statistical Analysis
STATA version 16.0 was used to perform the meta-analysis. The choice of random or fixed effects use was based on heterogeneity. Significant heterogeneity was defined as I 2 above 50% or P-value < .10. To calculate the ORs, the fixed-effects Mantel–Haenszel method was chosen for pooled effect estimates with non-significant heterogeneity and random-effects restricted maximum likelihood (REML) method used in case of significant heterogeneity. The model of meta-analysis of proportion was also based on heterogeneity. P-values ≤ .05 were considered statistically significant. Meta-regression analysis was performed for the primary outcome (restenosis) of the DCB and DES group, using the baseline clinical and procedural characteristics as covariates. Egger’s test and funnel-plot analyses were not performed due to the small number of studies.
Results
Baseline Characteristics
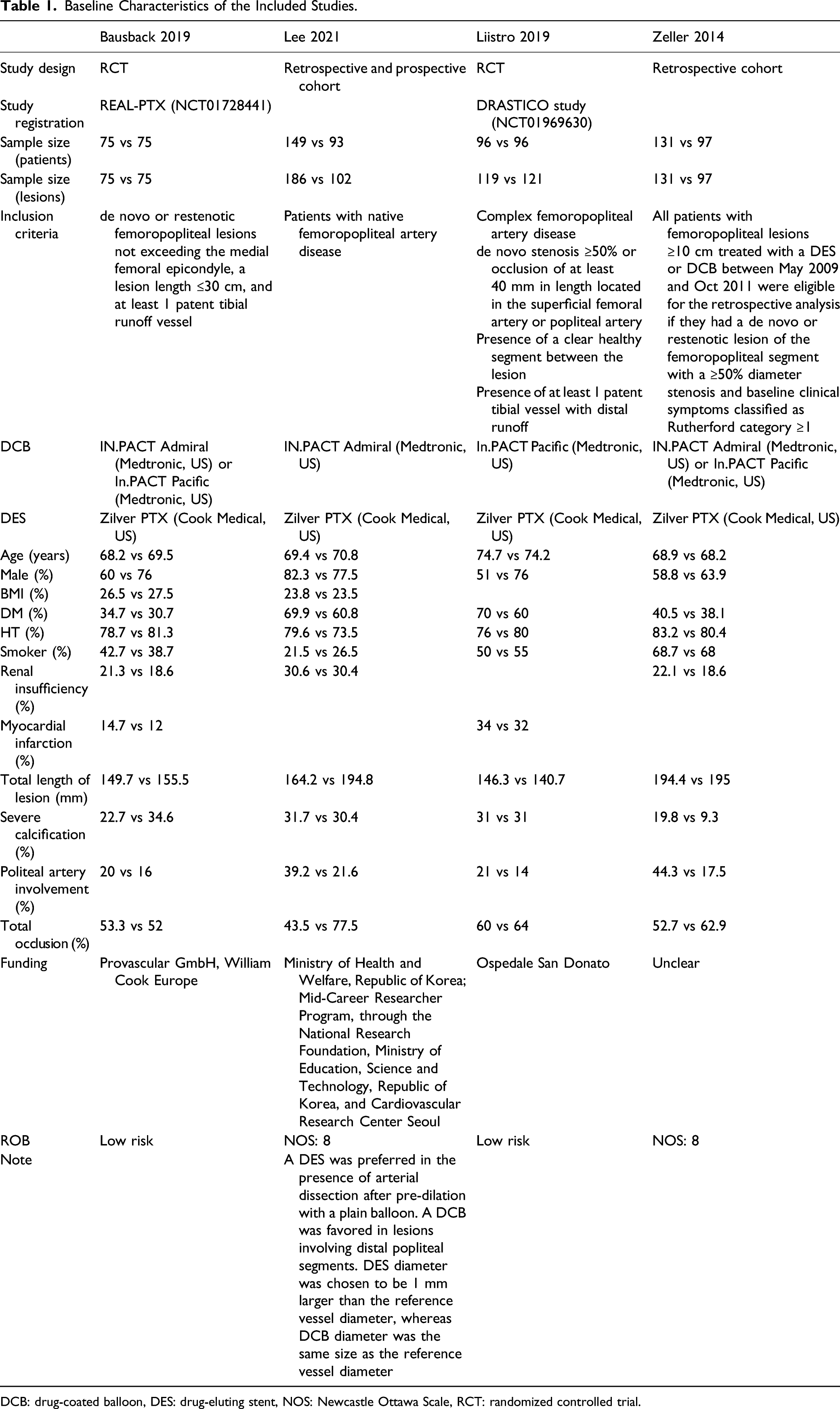
There were 4 studies comprising 812 patients (906 lesions) included in this systematic review and meta-analysis (Figure 1).1,8-10 The baseline characteristics can be seen in Table 1. PRISMA flowchart. Baseline Characteristics of the Included Studies. DCB: drug-coated balloon, DES: drug-eluting stent, NOS: Newcastle Ottawa Scale, RCT: randomized controlled trial.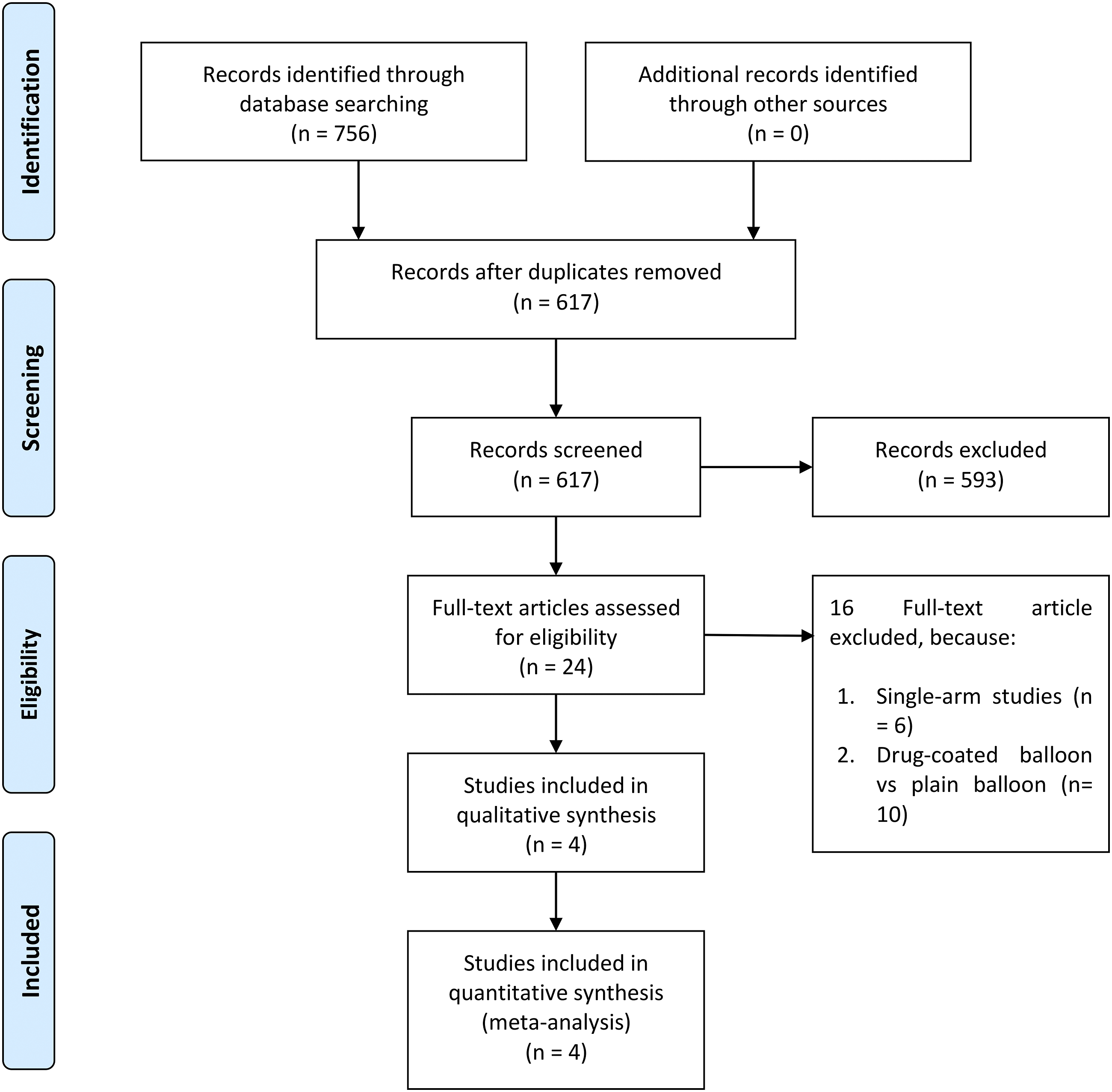
Rate of Restenosis
The rate of restenosis was .19 [.13, .26] in DCB and .24 [.20, .28] in DES. There was no significant difference between the rate of restenosis (OR .73 [.52, 1.03], P = .074; I2: 46.3%, P = .134) in DCB compared to DES group (Figure 2). Rate of restenosis.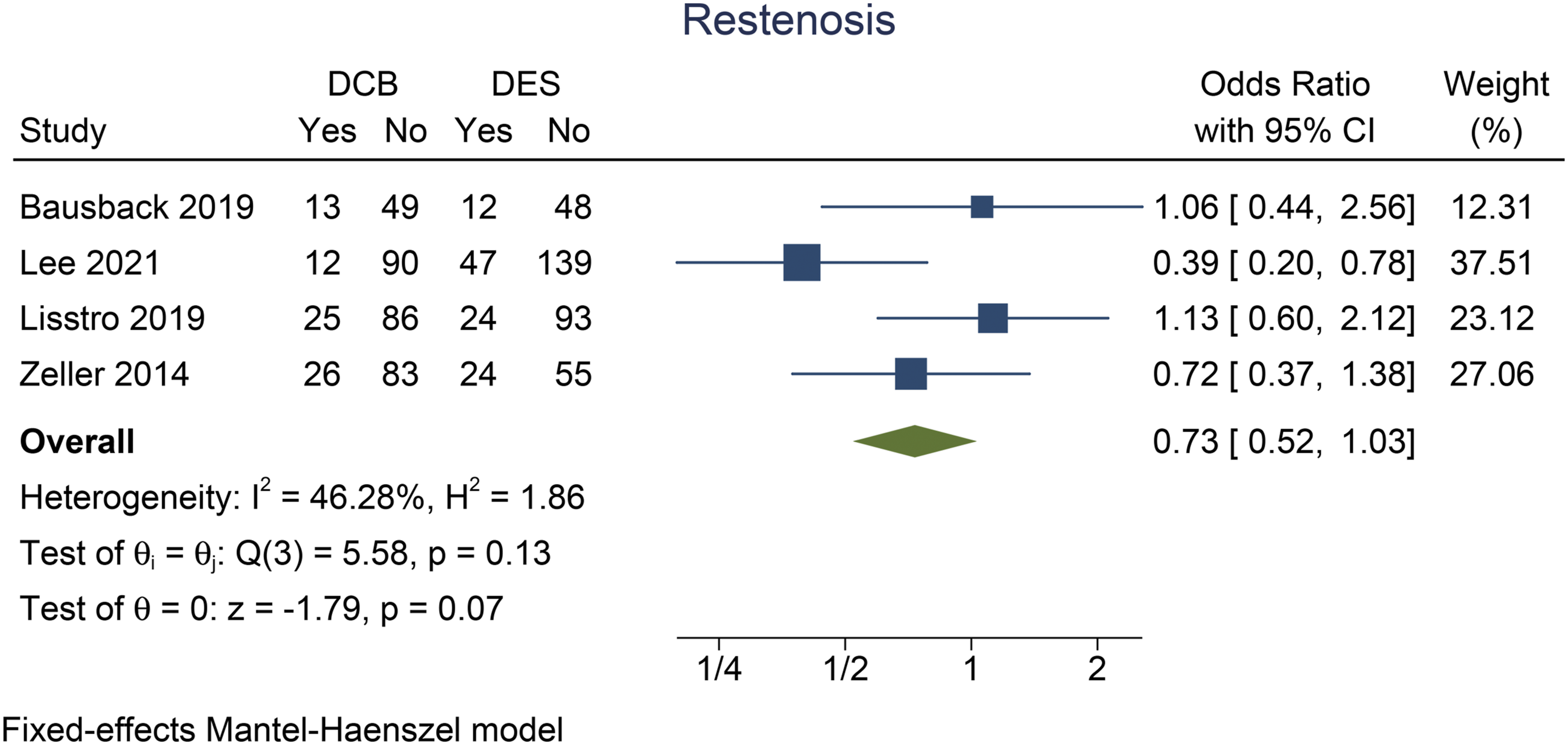
Target Lesion Revascularization
The rate of TLR was .11 [.08, .14] in DCB and .17 [.14, .21] in DES. TLR was lower (OR .61 [.41, .92], P = .017; I2: 1.2%, P = .386) in the DCB group compared to the DES group (Figure 3). Target lesion revascularization.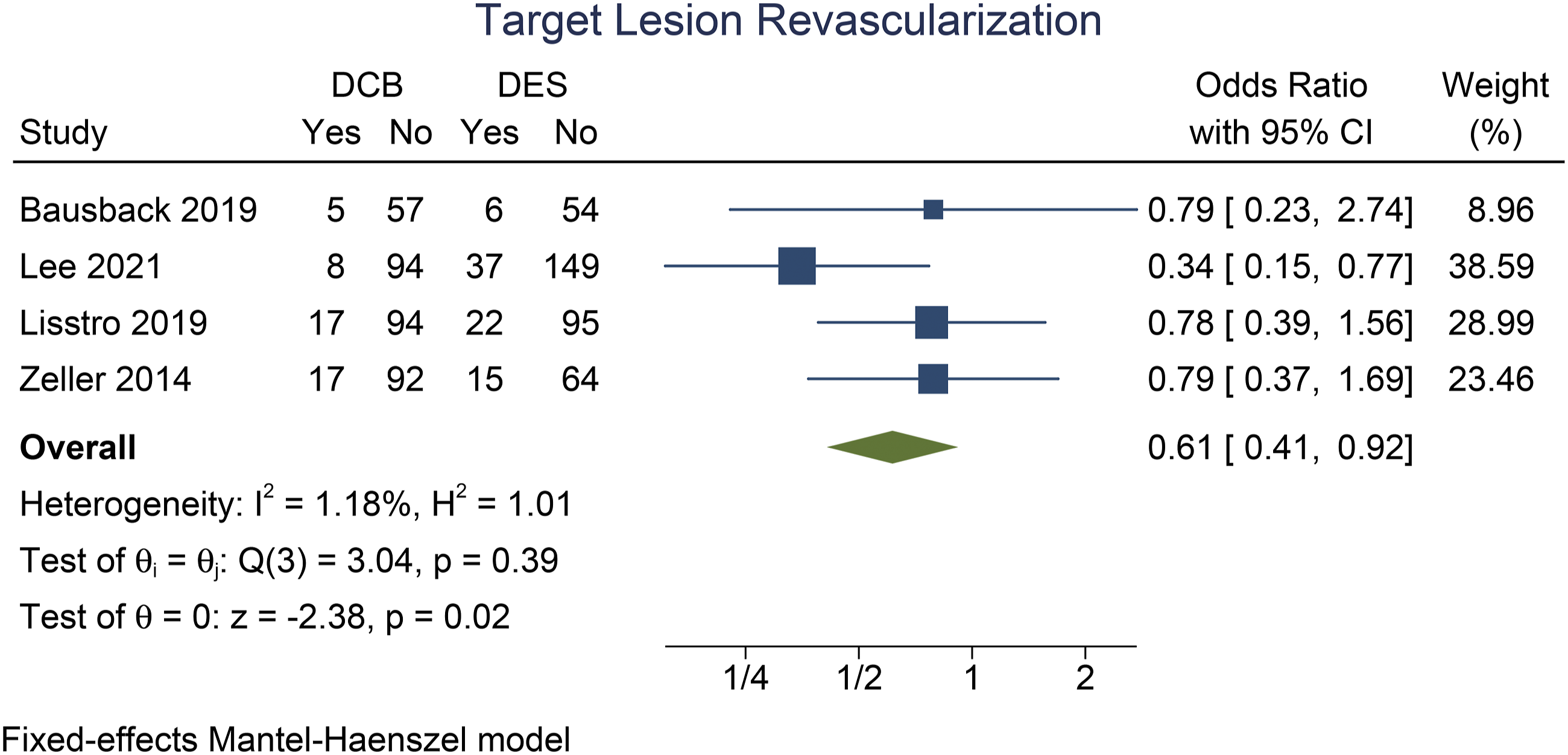
Mortality
Mortality rate was .06 [.04, .09] in DCB and .04 [.03, .06] in DES. There were no significant differences in terms of mortality (OR 1.38 [.78, 2.44], P = .268; I2: 0%, P = .716) among the two groups (Figure 4). Mortality.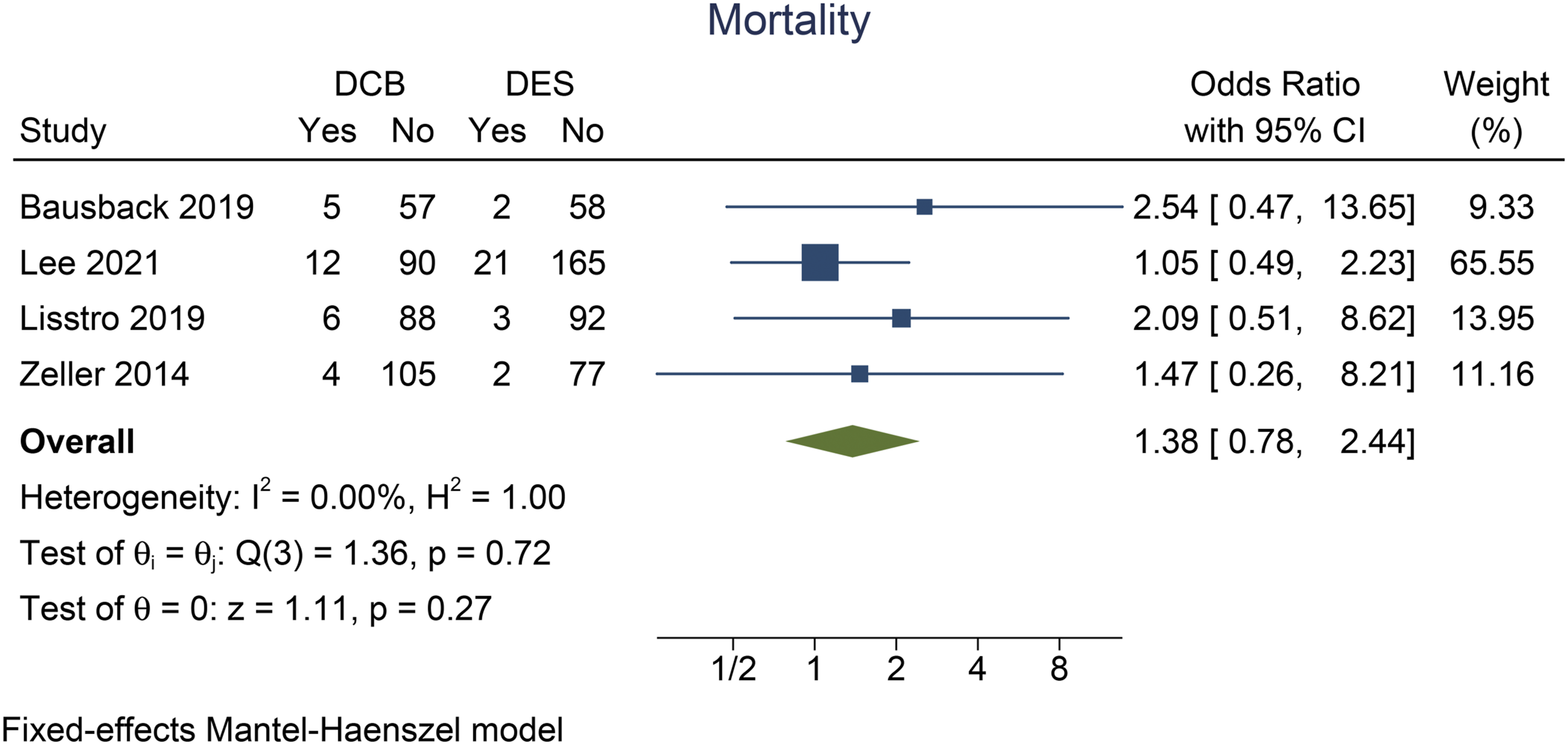
Meta-Regression for Restenosis Rate
Meta-regression analysis showed that the rate of restenosis in DCB in this pooled analysis was affected by sex (reference: male, coefficient −.004, P = .009), smoking (coefficient: .003, P = .010), and total occlusion (coefficient: .008, P = .004). However, it was not affected by age (P = .724), diabetes (P = .373), hypertension (P = .927), total length of lesion (P = .829), popliteal artery involvement (P = .720), and the presence of severe calcification (P = .262).
Meta-regression analysis showed that the rate of restenosis in DES in this pooled analysis was not affected by age (P = .224), sex (reference: male, P = .227), diabetes (P = .875), hypertension (P = .705), smoking (P = .718), popliteal lesion (coefficient: P = .363), total length of lesion (P = .123), presence of severe calcification (P = .132), popliteal artery involvement (P = .274), and total occlusion (P = .605).
Risk of Bias Assessment
The studies have low risk of bias based on NOS for observational studies (Table 1) and Cochrane Risk of Bias Assessment for RCTs (Figure 5). Cochrane risk of bias assessment.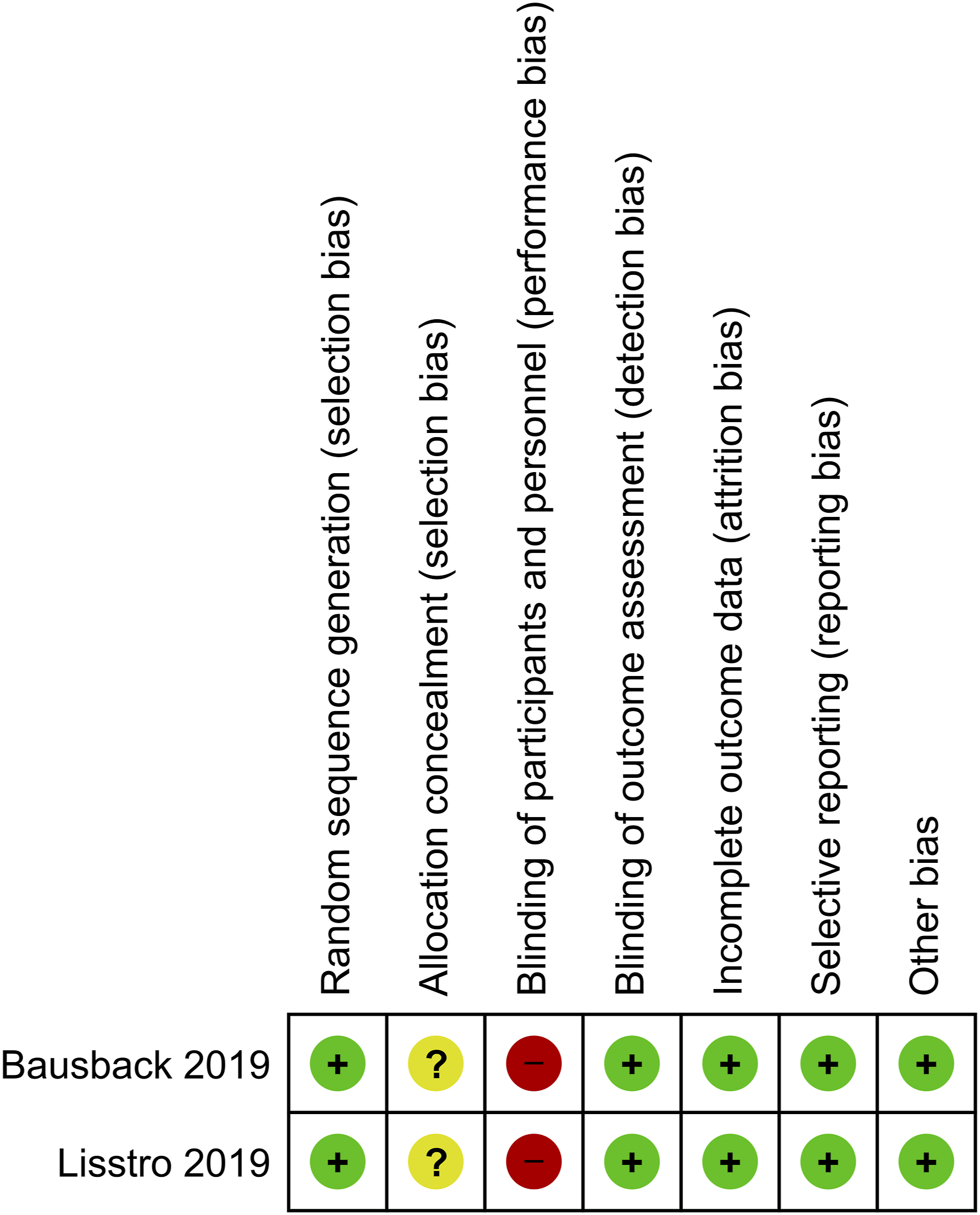
Discussion
This meta-analysis indicates that the use of DCB in patients with femoropopliteal lesions was associated with a similar rate of stenosis, lower TLR, and similar mortality rate compared to DES use with low heterogeneity. The benefit is most readily observed in Lee et al study that evaluates intervention in patients with native femoropopliteal artery disease, which has the highest sample size. It is unclear whether the statistical significance achieved was due to adequate statistical power or by chance. Low heterogeneity may indicate that the effect estimate is true, although RCTs with large sample size are required to confirm the finding. Based on this meta-analysis, we can conclude that DCB is at least non-inferior to DES.
The restenosis rate in the DCB group was affected by male sex, smoking, and total occlusion. Critical limb ischemia was shown to be an independent factor contributing to restenosis in patients receiving DCB, thus supporting total occlusion’s association with restenosis. 11 However, our finding was in contrast with a study that found the protective effect of smoking on restenosis in lower-limb intervention and coronary artery intervention.12,13 None of the factors were found to affect patients in DES group despite variations among the baseline characteristics of the studies. However, the possibility of type II error remains due to small number of studies. Based on the information of factors affecting restenosis in DCB and DES groups, future RCTs might be developed based on this finding. For example, since total occlusion reduces the benefit seen in patients receiving DCB, further trials should be designed to assess DCB vs DES in patients with total occlusion to determine which modality is superior.
The narrowing of peripheral arteries, as seen on PAD, compromises the blood supply to the lower extremities.1,2 Endovascular intervention is one of the modalities for treating PAD by increasing the luminal diameter of atherosclerotic vessels. 14 However, in-stent restenosis, is a common cause of treatment failure that may compromise long-term outcome.14-19 Development of restenosis was due to the synergistic effect between mechanical and biological mechanisms, including the immediate vessel recoil, negative vascular remodeling, and hyperplasia of the intima.20,21 Therefore, the addition of biological agents helps to inhibit vessel wall proliferation and reduces restenosis. 14 Paclitaxel is one of the antiproliferative drugs that is commonly mounted in DCB and DES; it is a promising agent in slowing restenosis with a good safety profile. 22 Paclitaxel binds to the beta subunit of tubulin, inhibiting microtubular function and cell division. 21 Paclitaxel is also favored due to its lipophilic properties which are often paired with a co-drug to facilitate drug absorption to the target vessel. 14 Percutaneous revascularization in both coronary and peripheral is well known for its high technical success, and DES is developed to reduce the rate of restenosis. 4 Paclitaxel, sirolimus, and everolimus are among the drugs that can be mounted on the stent’s surface, released at various rates, and capable of inhibiting post-procedure inflammation and neointimal hyperplasia.14,23,24
While DCB and DES remain at the forefront in managing PAD, careful selection is needed to ensure a maximal advantage on the long-term outcome. Endovascular treatment with balloon angioplasty is proven to be inferior to modern stent and DCB in the context of intimal hyperplasia and smooth muscle proliferation, which eventually will lead to restenosis. 1 DCB has recently gained more attention, mainly due to early studies that showed a significant variability of site-specific drug uptake and rapid drug washout. 25 However, compared to percutaneous transluminal angioplasty, the number of late lumen loss, rate of vascularization, death, and amputation are more favorable in the DCB group.26-28
The limitation of this systematic review and meta-analysis is due to the small number of studies. Additionally, meta-regression analysis was based on a small number of studies, although these studies have high variation in their baseline characteristics. The operators cannot be blinded to the intervention; however, it is unlikely that this will affect the outcome significantly. Further RCTs with large sample size were required for a definite conclusion.
Conclusion
This meta-analysis indicates that DCB use in patients with femoropopliteal lesion was associated with similar rate of restenosis, lower TLR, and similar mortality rate compared to DES use with low heterogeneity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Available on reasonable request